Relationship between vitamin B6 intake and thyroid function in US adults: NHANES 2007–2012 results
Lei Li, Jiangbo Wang, Jianping Chen

TL;DR
This study found that higher vitamin B6 intake is linked to lower thyroid hormone levels in US adults, especially in certain subgroups like males and older people.
Contribution
The study provides new evidence from a large population on the relationship between vitamin B6 intake and thyroid function.
Findings
Higher vitamin B6 intake was associated with lower total thyroxine (TT4) levels overall.
The negative correlation was stronger in males, older adults, and those with normal iodine intake.
No interactions were found between vitamin B6 and subgroups like gender, age, BMI, or iodine content.
Abstract
Existing studies have focused on the relationship between vitamin B6 and thyroid disease. However, there is a lack of large cross-sectional studies reporting on the relationship between vitamin B6 and thyroid function. Therefore, the present study aimed to assess the association between vitamin B6 intake and thyroid function in a population of US adults aged 20 years and older, using data from the National Health and Nutrition Examination Survey (NHANES) between 2007 and 2012. Demographic, dietary, thyroid function, and relevant data from NHANES 2007–2012 were collected. The relationship between vitamin B6 intake and thyroid function was analysed using weighted multiple regression and restricted cubic spline analysis, including subgroup and interaction analysis. The study included 6954 participants with a weighted mean age of 47.39 ± 16.60 years, mean vitamin B6 intake of 2.07 ± 1.15…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
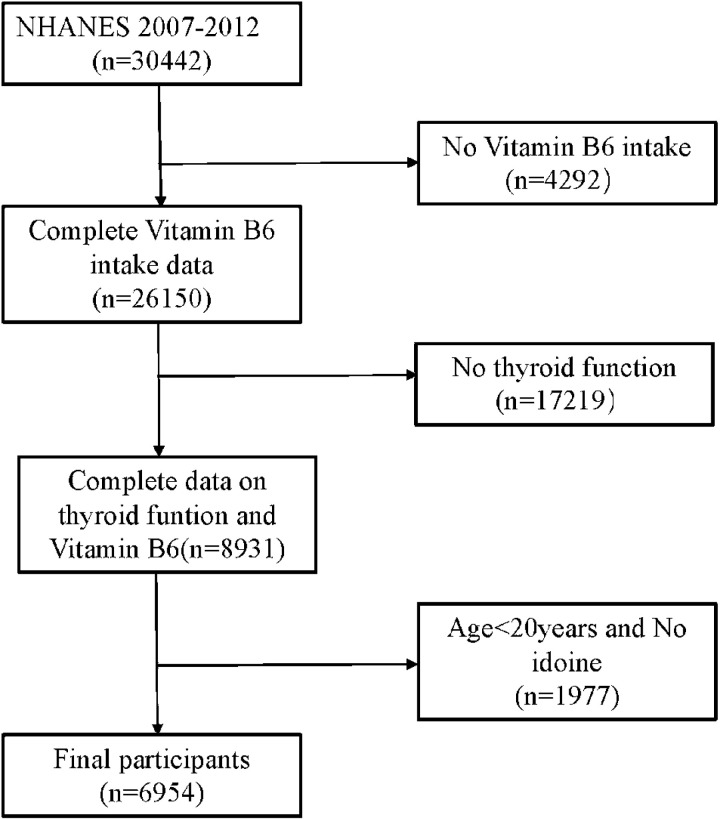 Fig 1
Fig 1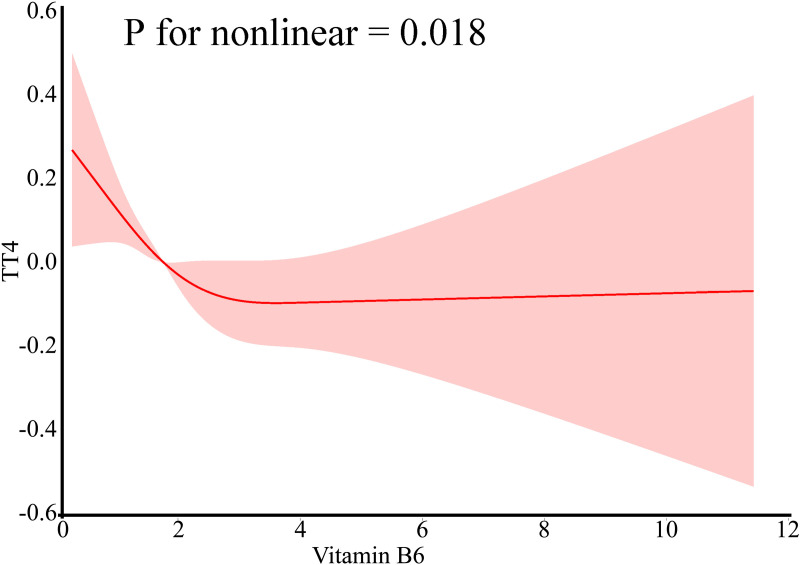 Fig 2
Fig 2- —http://dx.doi.org/10.13039/501100001809National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFolate and B Vitamins Research · Vitamin C and Antioxidants Research · Vitamin D Research Studies
Introduction
Vitamin B6, also known as pyridoxine, is a water-soluble nutrient crucial for human health and well-being [1]. Its active form, pyridoxal 5’-phosphate (PLP), serves as a cofactor in >150 enzymatic reactions and plays a role in inflammatory processes [2–4]. Studies have indicated a negative correlation between vitamin B6 intake and various inflammation markers [5]. Furthermore, both vitamin B6 intake and supplementation have been associated with improved immune function, particularly in individuals with vitamin B6 deficiency [6,7].
The thyroid gland is a pivotal endocrine organ governing human growth, development, and metabolism through the secretion of thyroid hormones (THs) [8–10]. This process is intricately regulated by the hypothalamus–pituitary–thyroid axis, where thyroid stimulating hormone (TSH) synthesised by the pituitary gland directly influences TH synthesis and secretion. TSH serves as a crucial indicator for subclinical hyperthyroidism and hypothyroidism. TH synthesis commences with iodine oxidation, leading to the formation of thyroglobulin derivatives (MIT and DIT) and culminating in the production of T3 and T4 via parallel coupling [11]. The enzyme thyroid peroxidase (TPO) plays a central role in this synthesis process. Free TH (FT3 and FT4) constitutes the biologically active forms of TH, with total TH (TT3 and TT4) converted simultaneously into free forms to maintain physiological levels [8].
While iodine intake significantly impacts thyroid function [12], dietary nutrients also play a crucial role [13]. Selenium intake, for instance, has been linked to reduced risk of Hashimoto’s thyroiditis, an immune system-induced chronic inflammatory disease of the thyroid gland characterised by chronic lymphocytic infiltration and abnormally high levels of TGAb and TPOAb antibodies [14]. Thyroid function is also influenced by zinc, iron, and vitamin D intake [15–17]. The relationship between vitamin B6 and thyroid disease has been the focus of recent research. Researchers found that TSH secretion via the hypothalamus/pituitary gland was suppressed by intravenous vitamin B6 in patients with primary hypothyroidism in a double-blind, randomised, controlled clinical trial [18]. In addition, a controlled study showed that patients with Hashimoto’s thyroiditis had slightly lower serum vitamin B6 levels (but no statistically significant difference) and higher levels of free thyroid hormone than healthy controls. This suggests that monitoring vitamin B6 levels may help to control Hashimoto’s thyroiditis [19]. However, the specific relationship between vitamin B6 and thyroid function has not been investigated in large cross-sectional studies. In an animal study, researchers found that serum T3 and T4 and pituitary TSH levels were significantly reduced in rats in the vitamin B6-deficient group compared with rats in the normal and vitamin B6-supplemented groups, but there was no significant difference in serum TSH [20]. Therefore, our study aims to investigate this association among individuals aged ≥20 years using data from the National Health and Nutrition Examination Survey (NHANES) spanning from 2007 to 2012.
Methods
Population and design of the study
NHANES is a research programme conducted by the National Center for Health Statistics (NCHS) to evaluate the health and nutritional status of adults and children in the United States. Data collection involved interviews at participants’ homes and health measurements in specialised mobile centres to ensure the reliability of data collection. Our study utilised three NHANES cross-sections from 2007–2008, 2009–2010, and 2011–2012, approved by the NCHS Research Ethics Review Board (ERB). In this study, we selected dietary vitamin B6 data and thyroid function laboratory data. We excluded data from individuals with missing iodine data and age <20 years. A total of 7936 participants were included in our analyses (Fig 1).
Screening process for NHANES participants from 2007 to 2012
Evaluation of dietary vitamin B6
Dietary vitamin B6 served as the primary predictor variable. For the analysis, we used data from two sets of dietary recall interviews. The first 24 h dietary recall data were collected at the Mobile Examination Centre (MEC), and the second 24 h dietary recall data were obtained through a follow-up interview conducted by telephone 3 to 10 days later. The average of the two 24 h dietary recalls was used as the final data for vitamin B6. The method of the 24 h dietary recall was based on the NHANES protocol as described in detail in the Dietary Intake Survey Procedures Manual [21–23].
Thyroid gland function
Thyroid function, our outcome variable, encompassed eight measures assessed via serum immunoenzymatic assay: TSH, T3/FT3, T4/FT4, TT3(Total Triiodothyronine), TT4(Total Thyroxine), thyroglobulin, thyroglobulin antibody, and thyroid peroxidase antibody. Sample collection and processing adhered to NHANES Laboratory/Medical Technician Procedure Manual guidelines.
Covariates
Covariates included age, gender, race, education, annual household income and poverty ratio, marital status, smoking, urinary iodine concentration (UIC), body mass index (BMI), energy intake, dietary fibre, and total vitamin B6 supplementation. Following the NHANES article on thyroid function, we classified BMI as normal (BMI < 25 kg/m^2^), overweight (25 kg/m^2^ ≤ BMI < 30 kg/m^2^), and obese (BMI ≥ 30 kg/m^2^); smoking as never, sometimes, and daily; and urinary iodine as iodine deficiency (UIC < 100μg/L), normal iodine (100 μg/L ≤ UIC < 300μg/L), and iodine excess (UIC ≥ 300μg/L) [13,24]. Table 1 presents detailed breakdowns.
Table 1: Baseline characteristics of participants in 2007–2012 (weighted).
Statistical analyses
We applied NHANES guidelines for sampling weights and employed complex multistage sampling procedures to prevent oversampling bias. Continuous variables are expressed as mean ± standard deviation, and categorical variables as frequencies and percentages. We utilised weighted multiple linear regression models, including unadjusted, partially adjusted, and fully adjusted models, to assess the association between vitamin B6 intake and thyroid function. The partially adjusted model was adjusted for age, gender, ethnicity, education level, and UIC. Fully adjusted models included age, gender, race, education level, marital status, annual household income and poverty ratio, UIC, smoking, energy intake, dietary fibre, and BMI. Interaction and subgroup analyses were conducted for Age, Gender, BMI and UIC. Restricted cubic spline (RCS) analysis was used to construct regression curves. Statistical analyses were performed using software packages R (http://www.R-project.org; R Foundation) and EmpowerStats (www.empowerstats.com).
Ethics statement
The studies involving human participants received approval from the National Center for Health Statistics (NCHS) and the Research Ethics Review Board. The research was conducted in compliance with local legislation and institutional requirements. Participants provided their written informed consent to take part in this study.
Results
Baseline characteristics of the study population
A total of 6954 participants were included, with a mean age of 47.39 ± 16.60 years. Gender distribution was relatively balanced, comprising 53.3% Females and 46.7% males. Stratification of the results by vitamin B6 quartiles revealed significant differences in dietary (energy intake and dietary fibre; P < 0.05) and laboratory (FT3, FT4, TT4, and TG; P < 0.05) data, as well as demographic data such as smoking status, marital status, annual household income and poverty ratio, education level, age, and gender (all P < 0.05; Table 1). Notably, the highest vitamin intake group (Q4) had significantly lower TT4 levels, more females, higher education levels, increased energy and fibre intake than the lowest intake group (Q1).
Relationship between vitamin B6 intake and thyroid function
Weighted multivariable linear regression revealed correlations between vitamin B6 intake and thyroid function (Table 2). In the unadjusted model, positive correlations were observed with T3 (β = 0.03, 95% CI = 0.02–0.04, P = 0.001) and negative correlations with TT4 and TG (TT4: β = −0.17, 95% CI = −0.22 to −0.13, P < 0.001; TG: β = −0.99, 95% CI = −1.7 to −0.24, P = 0.011). Compared with model 1, model 2 reported a negative correlation only between TT4 and vitamin B6 intake (β = −0.10, 95% CI = −0.14 to −0.06, P < 0.001), after adjusting for age, gender, ethnicity, education level and UIC. In model 3, we further adjusted for marital status, annual household income and poverty ratio, smoking, energy intake, dietary fibre, and BMI and found that TT4 is negatively associated with vitamin B6 intake (TT4: β = −0.05, 95% CI = −0.10 to 0.00, P = 0.033). In addition, we examined the correlation between vitamin B6 supplementation and thyroid function, and the results showed no correlation between vitamin B6 supplementation and these 8 indicators of thyroid function. (Supplyment, S1 Table).
Relationship between vitamin B6 intake and thyroid function: RCS analysis
RCS curves for the modelling and visualisation of the association between vitamin B6 and eight indicators of thyroid function demonstrated a non-linear relationship between vitamin B6 and TT4 levels after full adjustment for confounders in model 3 (TT4: P for non-linear = 0.018). The results showed that among these eight indicators of thyroid function, only TT4 and vitamin B6 were found to correlate significantly (Fig 2). As shown in the appendix (Supplyment, S1 Fig), there was no correlation between the remaining 7 indicators of thyroid function and vitamin B6. We also analysed the relationship between vitamin B6 supplement intake and thyroid function by RCS. This showed no correlation between these 8 indicators of thyroid function and vitamin B6 supplement intake, as shown in the appendix (Supplyment, S2 Fig).
Subgroup analysis
In subgroup analyses according to gender, men had a more significant negative correlation between vitamin B6 intake and TT4 levels compared to female adults (β = −0.06, 95% CI = −0.11 to −0.01, P = 0.028); in subgroup analyses according to age, older adults (age: 60–80 years) had a more significant negative correlation between vitamin B6 intake and TT4 levels compared to the other agegroups (β = −0. 13, 95% CI = −0.23 to −0.04, P = 0.008); in the subgroup analysis of BMI, there was a more significant negative correlation between vitamin B6 intake and TT4 levels in the overweight population (BMI: 25–29.9 kg/m2) (β = −0. 13, 95% CI = −0.20 to −0.06, P = 0.001); in the UIC subgroup, vitamin B6 intake and TT4 levels were more negatively correlated in those with normal iodine intake (β = −0.07, 95% CI = −0.13 to −0.01, P = 0.021) (Tables 3). The interaction analysis did not show any significant interactions between gender, age, BMI, UIC and the relationship between vitamin B6 and TT4 levels (P for interaction > 0.05; Tables 3).
Discussion
This cross-sectional study included 6954 US adults aged ≥20 years from NHANES 2007–2012. We employed weighted multiple regression and RCS to explore the association between vitamin B6 intake and thyroid function and found a significant negative correlation between vitamin B6 intake and TT4 levels, particularly notable in the highest intake group (Q4) compared with the lowest intake group (Q1) in the fully adjusted model. RCS analyses further supported a non-linear negative correlation between vitamin B6 intake and TT4 levels. Gender, Age, BMI and UIC are known to influence thyroid function significantly. Thus, we conducted subgroup analyses stratified by Gender, Age, BMI and UIC to assess the relationship between vitamin B6 intake and TT4. Notably, the negative correlation between vitamin B6 intake and TT4 levels was more pronounced in male, overweight, older age groups (60–80 years), and individuals with normal iodine intake. An interaction analysis between vitamin B6 intake and gender, age, BMI and iodine levels demonstrated no correlation between vitamin B6 intake and TT4 levels in these subgroups (P > 0.05).
To the best of our knowledge, this is the first study to investigate the relationship between dietary B6 intake and thyroid function.Both iodine and tyrosine are raw materials for TH synthesis; thus, iodine intake certainly affects thyroid function. However, the impact of dietary factors other than iodine has also been highlighted in epidemiological studies. For instance, increased dietary selenium intake was negatively correlated with TT4 and TT4/TT3 in a study among US adults, and selenium is known for its anti-inflammatory properties that maintain TH levels and support thyroid function [25]. Moreover, a study in US adult males reported significant associations between the Dietary Inflammatory Index (DII) and increased TT4 and FT3 levels ([13]). The DII Disorder Number assesses the body’s inflammatory potential through dietary intake and predicts higher IL-6 and C-reaction protein(CRP) levels [26,27]. In large cross-sectional studies evaluating the immune-inflammatory index and thyroid function, the SII (immune-inflammatory index) was reported to be significantly negatively correlated with FT3 and FT3/FT4 and significantly positively correlated with TT4 [28]. These studies are mutually supportive of the important role of inflammation in the regulation of thyroid function.Although the mechanisms underlying the negative association between vitamin B6 intake and thyroid function remain unclear, our finding of a negative association between vitamin B6 intake and TT4 levels is biologically plausible. Tyrosine metabolism is involved in TH synthesis. Vitamin B6 is a cofactor that is directly or indirectly involved in TH synthesis [29]. Furthermore, higher vitamin B6 intake has been linked with reduced inflammation, as evidenced by its negative correlation with CRP in a large cross-sectional study in the United States and in a cross-sectional study in Boston, which reported that low serum vitamin B6 levels were associated with inflammation, higher oxidative stress, and metabolic status in Puerto Rican older adults [30,31]. The kynurenine (tryptophan-kynurenine) pathway (KP) is the main pathway for tryptophan metabolism, in which vitamin B6 plays a key role [32,33]. KP plays an important role in various immune and inflammatory mechanisms, particularly kynurenine (KYNA), which has anti-inflammatory, pro-inflammatory, and immunosuppressive properties [34–36]. In a study of female patients with autoimmune thyroiditis, a negative correlation was found between serum KYNA levels and serum deiodinase levels. Deiodinase is involved in the biological process of converting free T4 to free T3 in the serum [37]. Therefore, we suggest that vitamin B6 may be able to downregulate serum TT4 levels through a mechanism that inhibits inflammation onset. In addition, the results of the present study showed a negative correlation between the intake of vitamin B6 and the level of TT4. Thyroid hormone deficiency and excess can lead to adverse outcomes. These include hypothyroidism, hyperthyroidism and thyroid nodules [38,39]. A previous controlled trial has shown that intravenous vitamin B6 is effective in the suppression of TSH secretion in patients with hypothyroidism [39]. In addition, in the process of inflammation, vitamin B6 plays an important role. Therefore, in a population with thyroid disease and excess thyroid hormone, we hypothesised that vitamin B6 supplementation would probably be beneficial. However, to confirm the efficacy and safety of vitamin B6 in treating patients with thyroid disease, further clinical trials are needed.
T3 showed a positive correlation with vitamin B6 in the unadjusted model. This correlation disappeared in the adjusted model. The possible reasons for this are as follows: 1. Uncontrolled confounding may have caused the positive association observed in the unadjusted model. For example, both vitamin B6 intake and T3 levels may be influenced by factors such as lifestyle, intake of other nutrients and health status. When these variables are included in the adjusted model, the original correlation may become weaker or disappear.2. Initial positive correlations may be found by chance (i.e., false positives) and are particularly likely to occur in initial analyses involving large numbers of unadjusted variables. The inclusion of additional control variables may reveal that the initial correlation is not statistically significant as model adjustments become deeper.
We found a negative association between dietary vitamin B6 intake and TT4 levels in male adults in a gender subgroup analysis. Previous studies have shown that oestrogen increases iodine uptake and has an effect on the redox state of the thyroid [40–42]. In contrast, the effect of vitamin B6 on thyroid hormones is less pronounced and would therefore be more important in men. However, this requires further research and investigation. It has previously been shown that thyroid hormone secretion declines with age, possibly due to age-related changes in the enzymes involved in TH synthesis [43], and in age subgroup analyses we found a negative association between vitamin B6 intake and TT4 levels in the elderly population. We found a negative association between vitamin B6 intake and TT4 levels in overweight individuals in BMI subgroup analyses. In a previous cross-sectional study of mildly overweight people with normal thyroid function, an association was found between accumulation of abdominal subcutaneous fat and decreased T4 and TSH levels [44]. This is similar to our findings. However, the association between BMI and vitamin B6 and thyroid hormones needs further investigation. We found a negative correlation between vitamin B6 and TT4 levels in the iodine-normal group in a subgroup analysis of UIC. Previous studies have shown that both iodine excess and deficiency in humans can affect thyroid function. Thus, abnormal iodine levels in humans may reduce the effect of vitamin B6 on thyroid function [45,46].
In addition to this, the results of our study showed that there was no significant correlation between the intake of food supplements and the eight tests related to thyroid function. Possible reasons for this are:1. Vitamin B6 in supplements may differ from vitamin B6 in food in terms of bioavailability and absorption, which may affect its potential effect on thyroid function.2. The doses of supplements used in the study may not have been sufficient to have an effect on thyroid function or may have been so high that they could not be effectively utilised in vivo.3. If the participants already had an adequate intake of vitamin B6, additional supplements may not have produced any additional physiological effects.4. It is possible that the sample size was not large enough, resulting in a study with insufficient statistical power to detect small effect sizes. Discuss this point and recommend an increase in sample size in future trials.5. Consider a long-term follow-up study to assess the effects of long-term vitamin B6 supplementation on thyroid function.
Despite the strengths of our study, such as a nationally representative sample in the United States, which increases the generalisability of our results, and careful adjustment for confounding variables, several limitations should be noted. The cross-sectional nature of the study meant that it was not possible to establish any cause-and-effect relationship between vitamin B6 intake and thyroid function, and future studies are needed to clarify the potential mechanism of vitamin B6 and thyroid function. Second, although the present study estimated vitamin B6 intake by averaging data from two dietary recalls, a method that reduces the random error of one-time measurements, large variations between individuals may still affect the accuracy of the data and may not necessarily reflect an individual’s regular intake. However, with a large sample size, these random errors can be cancelled out to some extent, resulting in more reliable statistical results. In addition, it is important to note that the biases inherent in self-reported dietary data, such as the tendency of respondents to report intakes that are lower than their actual intakes, are difficult to avoid completely [47]. Lastly, our study focused solely on US adults aged ≥20 years, excluding children.
Conclusion
Although the present study has shown an association between vitamin B6 and serum TT4 levels, we have not been able to infer a causal relationship from this observational study. This hypothesis should be the subject of future studies through the design of intervention trials. The dose-response relationship of vitamin B6 should be further investigated on this basis. In addition, this study did not include people under the age of 20. We suggest that future studies should be expanded to include this age group. This will not only improve the generalisability of the study. It will also help to understand the relationship between vitamin B6 and thyroid function at different stages of growth and development.
Non-linear relationship between vitamin B6 intake and eight thyroid functions based on RCS regression models: (A)Vitamin B6 intake andTT4.
Table 2: Relationship between vitamin B6 intake and thyroid function.
Table 3: Subgroup analyses.
Supporting information
S1 FigCorrelation between the remaining 7 indicators of thyroid function and vitamin B6.(TIF)
S2 FigCorrelation between 8 indicators of thyroid function and vitamin B6 supplement intake.(TIF)
S1 TableBaseline characteristics of participants based on total vitamin B6 supplementation, 2007–2012 (weighted).(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Percudani R, Peracchi A. The B 6 database: a tool for the description and classification of vitamin B 6-dependent enzymatic activities and of the corresponding protein families. BMC Bioinformatics. 2009;10:273. doi: 10.1186/1471-2105-10-273 19723314 PMC 2748086 · doi ↗ · pubmed ↗
- 2Chiang E-PI, Bagley PJ, Selhub J, Nadeau M, Roubenoff R. Abnormal vitamin B(6) status is associated with severity of symptoms in patients with rheumatoid arthritis. Am J Med. 2003;114(4):283–7. doi: 10.1016/s 0002-9343(02)01528-0 12681455 · doi ↗ · pubmed ↗
- 3Chiang E-P, et al. Inflammation causes tissue-specific depletion of vitamin B 6. Arthritis Res Ther. 2005;7(1):1–9.16277678 10.1186/ar 1821 PMC 1297572 · doi ↗ · pubmed ↗
- 4Chiang E-PI, Bagley PJ, Roubenoff R, Nadeau M, Selhub J. Plasma pyridoxal 5’-phosphate concentration is correlated with functional vitamin B-6 indices in patients with rheumatoid arthritis and marginal vitamin B-6 status. J Nutr. 2003;133(4):1056–9. doi: 10.1093/jn/133.4.1056 12672918 · doi ↗ · pubmed ↗
- 5Friedman AN, Hunsicker LG, Selhub J, Bostom AG. Clinical and nutritional correlates of C-reactive protein in type 2 diabetic nephropathy. Atherosclerosis. 2004;172(1):121–5. doi: 10.1016/j.atherosclerosis.2003.09.011 14709365 · doi ↗ · pubmed ↗
- 6Chandra RK, Sudhakaran L. Regulation of immune responses by vitamin B 6. Ann N Y Acad Sci. 1990;585:404–23. doi: 10.1111/j.1749-6632.1990.tb 28073.x 2192621 · doi ↗ · pubmed ↗
- 7Xu D, Michie SA, Zheng M, Takeda S, Wu M, Peltz G. Humanized thymidine kinase-NOG mice can be used to identify drugs that cause animal-specific hepatotoxicity: a case study with furosemide. J Pharmacol Exp Ther. 2015;354(1):73–8. doi: 10.1124/jpet.115.224493 25962391 PMC 4468429 · doi ↗ · pubmed ↗
- 8Cheng S-Y, Leonard JL, Davis PJ. Molecular aspects of thyroid hormone actions. Endocr Rev. 2010;31(2):139–70. doi: 10.1210/er.2009-0007 20051527 PMC 2852208 · doi ↗ · pubmed ↗