Necrotizing Soft Tissue Infections Caused by Morganella morganii: A Case Report and Review of the Literature
Masakazu Kakurai, Shigehiko Takeyama, Yoshihiro Moriyama

TL;DR
A rare case of necrotizing soft tissue infection caused by Morganella morganii in a 74-year-old man with underlying health conditions is reported and reviewed.
Contribution
This paper presents a rare clinical case of necrotizing soft tissue infection caused by Morganella morganii and reviews similar cases from the literature.
Findings
Morganella morganii was identified as the sole pathogen in pus and blood cultures from a necrotizing soft tissue infection.
The patient's condition deteriorated despite surgical debridement and antibiotic treatment, leading to death within 14 days.
Eight cases of necrotizing soft tissue infections caused by Morganella morganii were reviewed, including the presented case.
Abstract
Morganella morganii is an unusual opportunistic pathogen often isolated as a cause of nosocomial infections in adults, particularly in wound and urinary tract infections. Herein, we present a case of necrotizing soft tissue infections in the right lower leg to the foot caused by Morganella morganii. A 74-year-old Japanese male with a history of microscopic polyangiitis and chronic kidney disease was referred to our department with severe painful swelling, warmth, and purpura extending from the right lower leg to the foot. An exploratory incision revealed a discharge of a large amount of light yellowish pus, and the superficial fascia and overlying fat tissue were easily dissected using a swab. Surgical debridement was performed. Pus and two sets of blood cultures grew only Morganella morganii. Taken together, necrotizing soft tissue infections caused by Morganella morganii were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1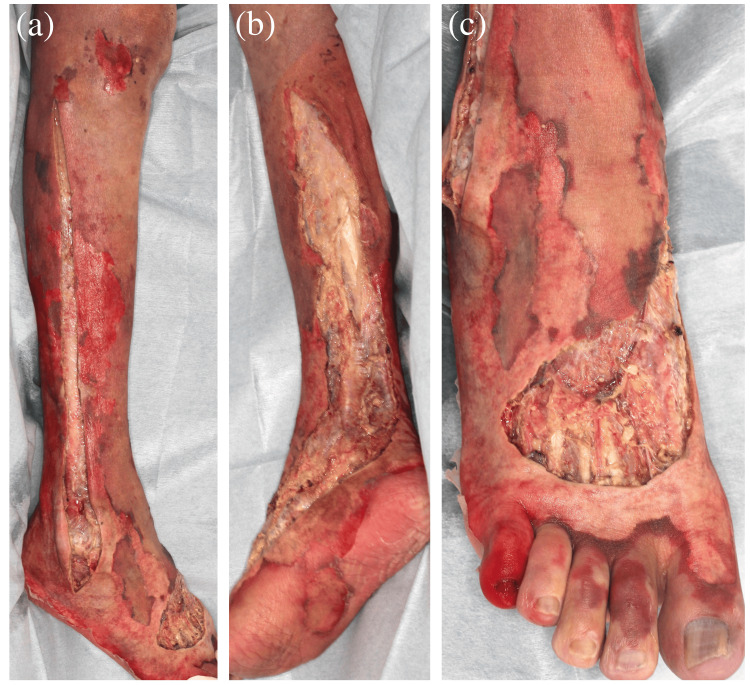 Figure 2
Figure 2| Blood test | Reference value (male) | On admission | On day 2 | On day 10 |
| Aspartate aminotransferase (U/L) | 8-38 | 21 | 168 | 113 |
| Alanine aminotransferase (U/L) | 4-44 | 10 | 35 | 21 |
| Lactate dehydrogenase (U/L) | 124-222 | 471 | 660 | 1148 |
| Sodium (mEq/L) | 135-147 | 142 | 140 | 139 |
| Potassium (mEq/L) | 3.6-5.0 | 4.9 | 4.3 | 4.1 |
| Urea nitrogen (mg/dL) | 8-20 | 43.9 | 31.4 | 47.7 |
| Creatinine (mg/dL) | 0.61-1.04 | 7.46 | 5.33 | 5.19 |
| Creatine kinase (U/L) | 57-197 | 109 | 4934 | 725 |
| C-reactive protein (mg/dL) | 0-0.20 | 2.03 | 30.50 | 26.22 |
| White blood cell (/μL) | 4,000-9,000 | 3,050 | 3,220 | 12,930 |
| Hemoglobin (g/dL) | 14.0-18.0 | 9.6 | 10.5 | 10.5 |
| Platelet (×104/μL) | 15.0-35.0 | 7.6 | 6.3 | 3.1 |
| Hemoglobin A1c (%) | 4.6-6.2 | 5.0 | – | – |
| PT-INR | 0.90-1.10 | 0.97 | 1.68 | 1.13 |
| FDP (μg/mL) | 0-5.0 | – | 57.0 | 47.5 |
| D-dimer (μg/mL) | 0-1.0 | 6.2 | 17.3 | 18.9 |
| Antimicrobial agent | MIC (μg/mL) | MIC interpretation |
| Ampicillin | >16 | R |
| Cefazolin | >16 | R |
| Ceftriaxone | ≤1 | S |
| Cefepime | ≤2 | S |
| Ampicillin-sulbactam | >16 | R |
| Piperacillin-tazobactam | ≤8 | S |
| Meropenem | ≤0.12 | S |
| Levofloxacin | ≤0.12 | S |
| Gentamicin | >8 | R |
| Sulfamethoxazole-trimethoprim | >2 | R |
| Author/year | Age/sex | Medical history | Affected sites | Other detected bacteria | Surgical treatment | Course |
| Krebs et al. (2001) [ | 0/F | Low birth weight, prematurity | Left leg | Escherichia coli | Above knee amputation | Dead |
| Lee et al. (2009) [ | 3/M | NA | Right ankle |
| Debridement | Improve |
| Soleimanian et al. (2011) [ | 67/M | DM | Right leg and right trunk | Escherichia coli, Proteus mirabilis, Enterococcus faecalis, Citrobacter freundii, Providencia rettgeri | Debridement | Improve |
| Richards et al. (2015) [ | 81/M | HT, heart failure, atrial fibrillation, stroke | Right lower extremity | Aeromonas hydrophila | Above knee amputation | Improve |
| Leiblein et al. (2020) [ | 64/M | Gastric bypass, cholecystectomy, appendectomy | Left groin | Proteus mirabilis, Enterococcus faecalis, Bacteroides fragilis | NA | Improve |
| Soedjana et al. (2024) [ | NA | NA | NA | Klebsiella pneumoniae | Debridement | Dead |
| NA | NA | NA | None | No surgery | Dead | |
| Our case | 74/M | MPA, CKD | Right lower leg and foot | None | Debridement | Dead |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Antimicrobial Resistance in Staphylococcus · Bacterial Identification and Susceptibility Testing
Introduction
Morganella morganii (M. morganii) is a facultative anaerobic, rod-shaped, Gram-negative enteric bacterium often associated with nosocomial infections in adults, specifically postoperative wound and urinary tract infections [1,2]. Its virulence and increasing drug resistance contribute to high mortality rates in some M. morganii infections [1,2]. Diseases caused by M. morganii include urinary tract infections, bacteremia, sepsis, septic arthritis, wound infections, cellulitis, and necrotizing soft tissue infections (NSTIs) [1,2]. The frequency of skin and soft tissue infections is relatively high in M. morganii infections [1,2]. However, NSTIs caused by M. morganii are rare, and no comprehensive literature exists to date.
NSTIs are rapidly progressing, life-threatening bacterial infections of soft tissue, resulting in widespread tissue destruction that may extend from the epidermis to the deep musculature [3]. This infection can occur after major traumatic injuries, minor breaches of the skin, or non-penetrating soft tissue injuries. The annual incidence of NSTIs ranges from 0.3 cases to 15.5 cases per 100,000 population [3]. NSTIs are largely distinguished by whether the cause is polymicrobial (type Ⅰ) or monomicrobial (type Ⅱ) [3]. Type Ⅰ infections are polymicrobial infections involving aerobic and anaerobic pathogens, whereas type Ⅱ infections, a monomicrobial infection, are mainly caused by group A Streptococcus [3]. Other less common type Ⅱ pathogens include Aeromonas hydrophila, Vibrio vulnificus, Bacteroides, and Escherichia coli [3].
We herein present a case of NSTIs extending from the right lower leg to the foot caused by M. morganii and review eight patients with M. morganii NSTIs, including ours.
Case presentation
A 74-year-old Japanese male presented to the emergency department with a two-day history of right lower leg pain that limited his ability to perform activities of daily living. On admission, he had a fever, chills, and right lower leg pain without warmth, swelling, or erythema. Intravenous cefepime dihydrochloride hydrate was initiated with a provisional diagnosis of cellulitis; however, during the following 36 hours, purpura developed from the right lower leg to the foot, and he was referred to our department. His medical history included microscopic polyangiitis and chronic kidney disease (CKD) on hemodialysis, and his medications included prednisolone (5 mg/day), vonoprazan fumarate, and sulfamethoxazole-trimethoprim. On examination, the patient had an axillary body temperature of 39.6℃, a heart rate of 90 beats per minute, a blood pressure of 92/61 mmHg, an oxygen saturation of 96% on room air, and a respiratory rate of 20 breaths per minute. The patient appeared unwell but showed no signs of impaired consciousness. Physical examination revealed severe, painful swelling and warmth, with irregularly shaped purpura accompanied by bullae extending from the right lower leg to the foot (Figures 1A, 1B). Skin lesions were limited to this region, with no skin ulcers; however, a skin fissure measuring 1 cm was observed on the right heel. Peristaltic sounds were normal, and no abdominal or costovertebral angle tenderness was noted. Blood tests revealed a white blood cell count of 3.22 × 10^3^/μL, hemoglobin of 10.5 g/dL, a platelet count of 6.3 × 10^4^/μL, blood urea nitrogen of 31.4 mg/dL, creatinine of 5.33 mg/dL, creatine kinase of 4934 U/L, C-reactive protein level of 30.50 mg/dL, prothrombin time-international normalized ratio of 1.68, and fibrinogen degradation products of 57.0 μg/mL (Table 1). Contrast-enhanced computed tomographic images ruled out acute limb ischemia and deep vein thrombosis. An exploratory incision was made to the depth above the superficial fascia on the right lower leg, which resulted in a discharge of a large amount of light yellowish pus with a slight odor; the superficial fascia and overlying fat tissue were easily dissected using a swab (Figures 1C, 1D).
Cutaneous findings.(a, b) Severe pain, swelling, and warmth with irregularly shaped purpura accompanied by bullae extending from the right lower leg to the foot. (c, d) Discharge of a large amount of light yellowish pus during exploratory incision. The superficial fascia and overlying fat tissue were easily dissected using a swab.
Because the patient refused amputation, surgical debridement was performed from the right lower leg to the foot (Figure 2). The wounds were left open for drainage.
Postoperative cutaneous images.The necrotic skin was removed from the right lower leg to the foot.
Postoperatively, the patient received circulatory and respiratory support in the intensive care unit, and cefepime dihydrochloride hydrate was changed to meropenem. On day three of hospitalization, two sets of blood cultures taken on admission grew M. morganii alone, whereas Gram staining of the urine did not reveal any microorganisms, and the urine culture was negative. Additionally, pus cultures grew only M. morganii. Therefore, the diagnosis of NSTIs caused by M. morganii was made. On day six, meropenem was switched to intravenous ciprofloxacin hydrochloride hydrate based on antibiotic susceptibility testing (Table 2).
Although skin necrosis did not spread after surgical debridement, the patient’s general condition gradually worsened, and the patient died 14 days after hospitalization.
Discussion
M. morganii is a facultative anaerobic, rod-shaped, Gram-negative enteric bacterium found in the environment and intestinal tracts of humans, mammals, and reptiles as part of the normal flora [1,2]. Initially considered a cause of summer diarrhea and an insignificant pathogen, it is now recognized as an important pathogen, mainly responsible for nosocomial infections in adults, particularly postoperative wound and urinary tract infections [1,2]. A typical example of animal-to-human transmission is M. morganii-associated skin and soft tissue infections following snakebites [4]. Although case reports of M. morganii infections are scattered, infections are most commonly reported in Taiwan, Japan, the United States, and Spain [1].
Diseases caused by M. morganii are diverse and include urinary tract infections, pneumonia, peritonitis, pericarditis, meningitis, bacteremia, sepsis, septic arthritis, osteomyelitis, pyomyositis, wound infections, cellulitis, and NSTIs [1,2]. In a previous study of 136 patients with M. morganii infections, skin and soft tissue infections were the most common (19%), followed by sepsis (11%), abscess (10%), urinary tract infections (8%), and bacteremia (7%) [1]. In another study on patients with M. morganii bacteremia, skin and soft tissue infections were the most common sources of bacteremia, followed by primary bacteremia and urinary tract infections [2]. Therefore, the frequency of skin and soft tissue infections is relatively high among M. morganii infections, and the skin is one of the portals of entry. However, NSTIs caused by M. morganii are rare and poorly reported, and no comprehensive literature exists.
NSTIs are a life-threatening bacterial infection of the soft tissue and are largely distinguished by whether the cause is polymicrobial (type Ⅰ) or monomicrobial (type Ⅱ) [3]. Type Ⅰ infections are polymicrobial infections involving aerobic and anaerobic pathogens that usually occur in the elderly or those with underlying medical conditions, including diabetes mellitus (DM). Type Ⅱ infections are mainly caused by group A Streptococcus and often occur in healthy individuals of all ages [3]. Other less common type Ⅱ pathogens include Aeromonas hydrophila and Vibrio vulnificus [3]. In addition, monomicrobial NSTIs caused by Gram-negative pathogens such as Bacteroides and Escherichia coli have been reported. This may not align with the typical patient characteristics of type Ⅱ infections, as it mainly occurs in immunocompromised patients [3]. Similarly, in our case, an immunocompromised patient was infected by M. morganii alone and developed NSTIs.
To date, only eight patients with NSTIs caused by M. morganii, including ours, have been reported (Table 3) [5-10].
Among the six patients with documented age, onset ranged from 0 to 81 years, occurring in children up to three years old and the sixth and eighth decades of life. Five of the six patients were male. All five patients with a documented medical history had prematurity, DM, CKD, or multimorbidity. Our case was the only one involving immunosuppressant use (prednisolone). The affected sites were located on the lower extremities (6/6 patients) and trunk (1/6 patients), excluding the upper extremities and head and neck region. In three patients, including ours, the cause of NSTIs was presumed to be skin entry [5,6]. Another patient developed an NSTI after a peripheral bypass of the lower extremity [7]. In the remaining four patients, the entry of M. morganii was unknown [8-10]. Six out of eight patients had polymicrobial infections [5-10], and the remaining two patients, including ours, had monomicrobial infections [10]. In summary, NSTIs caused by M. morganii tend to affect the lower extremities of pediatric and elderly males who are immunosuppressed or have multiple morbidities. Most cases of M. morganii NSTIs are polymicrobial infections, but monomicrobial NSTIs of M. morganii can occur.
Although early aggressive surgical intervention is important in the initial treatment of NSTIs to reduce mortality [3,10], the prognosis varies widely depending on factors such as the pathogen and host conditions. In a study of 90 patients with NSTIs in which most of the causative pathogens (85%) were Gram-negative bacteria, the overall mortality rate was 13%, and the highest mortality rate was in the nonsurgical group (37%, 3/8 patients), followed by surgical debridement alone (29%, 8/28 patients) and debridement followed by skin grafting (4%, 1/24 patients) [10]. In our literature review, half of the patients with M. morganii NSTIs died despite surgical debridement or amputation and appropriate antibiotic therapy, suggesting a poor prognosis.
M. morganii is normally susceptible to third- and fourth-generation cephalosporins, carbapenems, and quinolones, whereas it has intrinsic resistance to most first- and second-generation cephalosporins and ampicillin [1,2], consistent with our antibiotic susceptibility testing results. Recently, drug resistance has increased in M. morganii, resulting in high mortality rates in some M. morganii infections [1,2]. Additionally, M. morganii has been identified as a significant cause of nosocomial infections [1,2]. Therefore, appropriate antibiotic therapy and nosocomial infection control measures (e.g., hand washing and personal protective equipment) are important when M. morganii infections occur.
The limitations of this study include the limited number of cases and missing data from several reports. Additionally, among the polymicrobial NSTIs in which M. morganii was detected, its degree of contribution to infection remains unclear. Further accumulation of M. morganii NSTI cases is required to fully understand the pathogenesis, epidemiology, clinical characteristics, and appropriate treatments to reduce mortality.
Conclusions
Our case is unique as the patient developed NSTIs due to M. morganii, an unusual pathogen. To date, eight patients with M. morganii NSTIs, including ours, have been reported. Our review indicates that *M. morganii *NSTIs primarily affect the lower extremities of pediatric and elderly males with immunosuppression or multimorbidity. Most cases of M. morganii NSTIs are polymicrobial infections, but monomicrobial NSTIs of *M. morganii *can occur, as in our case. Half of the patients died despite surgical debridement or amputation, suggesting a poor prognosis. Further case accumulation is necessary to advance our understanding of its pathogenesis, epidemiology, and clinical characteristics, as well as to optimize treatment strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Morganella morganii, a non-negligent opportunistic pathogen Int J Infect Dis Liu H Zhu J Hu Q Rao X 10175020162742181810.1016/j.ijid.2016.07.006 · doi ↗ · pubmed ↗
- 2Clinical manifestations, risk factors and prognosis of patients with Morganella morganii sepsis J Microbiol Immunol Infect Erlanger D Assous MV Wiener-Well Y Yinnon AM Ben-Chetrit E 4434485220192891928310.1016/j.jmii.2017.08.010 · doi ↗ · pubmed ↗
- 3Necrotizing soft-tissue infections N Engl J Med Stevens DL Bryant AE 2253226537720172921167210.1056/NEJ Mra 1600673 · doi ↗ · pubmed ↗
- 4Necrotizing fasciitis following venomous snakebites in a tertiary hospital of southwest Taiwan Int J Infect Dis Tsai YH Hsu WH Huang KC Yu PA Chen CL Kuo LT 30366320172881122910.1016/j.ijid.2017.08.005 · doi ↗ · pubmed ↗
- 5Necrotizing fasciitis in a newborn infant: a case report Rev Hosp Clin Fac Med Sao Paulo Krebs VL Koga KM Diniz EM Ceccon ME Vaz FA 59625620011146020610.1590/s 0041-87812001000200005 · doi ↗ · pubmed ↗
- 6Haemorrhagic bullae associated with a chicken scratch Ann Trop Paediatr Lee CY Lee HF Huang FL Chen PY 3093112920091994175510.1179/027249309 X 12547917869168 · doi ↗ · pubmed ↗
- 7Necrotizing soft tissue infection following a peripheral bypass Ann Vasc Surg Richards CR Clark ME Bowen DK Uratake D Ayubi F Katras T Kellicut DC 84382229201510.1016/j.avsg.2014.12.03625733218 · doi ↗ · pubmed ↗
- 8Polymicrobial necrotizing fasciitis involving enterobacteria producing CTX-M-15 extended-spectrum β-lactamases J Med Microbiol Soleimanian S Gordon NC Wareham DW 1351376020112081384910.1099/jmm.0.021998-0 · doi ↗ · pubmed ↗