Association of time-to-treatment with prognosis in pneumocystis pneumonia among immunocompromised patients without HIV infection: a multi-center, retrospective observational cohort study
Haruka Fujioka, Hiroki Matsui, Yuya Homma, Tatsuya Nagai, Ayumu Otsuki, Hiroyuki Ito, Shinichiro Ohmura, Toshiaki Miyamoto, Daisuke Shichi, Watari Tomohisa, Yoshihito Otsuka, Kei Nakashima

TL;DR
This study found that early treatment of pneumocystis pneumonia in non-HIV patients did not significantly improve survival rates.
Contribution
The study provides new evidence that early treatment initiation does not significantly affect mortality in non-HIV pneumocystis pneumonia.
Findings
Early treatment within 2 days did not significantly reduce 30-day mortality compared to late treatment.
There was no significant difference in 180-day mortality between early and late treatment groups.
Subgroup analysis showed no significant mortality differences even in patients requiring oxygen.
Abstract
Pneumocystis jirovecii pneumonia (PCP) in non-human immunodeficiency virus (HIV) patients is associated with high morbidity and mortality. Although prior studies have linked delayed treatment to worse outcomes, they are often limited by small sample sizes and inadequate adjustment for confounders. Therefore, we evaluated whether early treatment after hospital admission improves mortality in non-HIV PCP, adjusting for patient characteristics. This multi-center, retrospective, observational cohort study included non-HIV PCP patients treated between January 2006 and March 2021 at three institutions. Participants were divided into the early treatment (initiated within 2 days) and late treatment (initiated between days 3 and 7) groups. The primary endpoint was 30-day mortality, and the secondary endpoints were 180-day mortality. Propensity score weighting was used to adjust for patient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
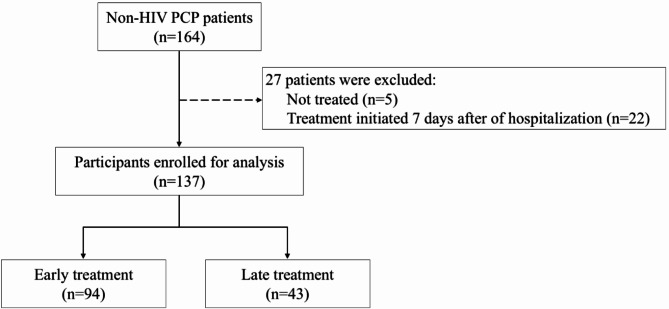 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumocystis jirovecii pneumonia detection and treatment · HIV/AIDS Research and Interventions · Pneumonia and Respiratory Infections
Background
Pneumocystis jirovecii pneumonia (PCP) is an opportunistic infection of patients with the human immunodeficiency virus (HIV)-infection-induced immunosuppression [1, 2]. PCP confers serious morbidity and mortality in immunocompromised patients, although the availability of highly active antiretroviral therapy has decreased the prevalence of acquired immunodeficiency syndrome in recent years [1, 3]. However, the number of patients with PCP but without HIV (non-HIV PCP) has increased as the number of those receiving anti-tumor chemotherapeutic agents, immunosuppressive therapy, and organ transplantation has been increasing [1, 4]. The mortality during the initial infection in patients with HIV PCP and non-HIV PCP is 10–20% and 30–60%, respectively [1, 2].
Prognostic factors for non-HIV PCP include several factors, such as advanced age, elevated lactate dehydrogenase (LDH) levels, low albumin, respiratory failure, hematological malignancies, increased blood urea nitrogen, concurrent bacteremia, and pre-existing lung disease [5, 6]. Furthermore, a delay in treatment is a prognostic factor for non-HIV PCP associated with worse outcomes [5, 7–10]. However, previous research on early treatment of non-HIV PCP had limitations, including a small sample and inadequate adjustment for confounding factors. For instance, a multi-center study conducted in France included both HIV PCP and non-HIV PCP cases, which made it difficult to accurately evaluate whether time-to-treatment contributes to mortality in non-HIV PCP [7]. Furthermore, another prior study noted the survival-related importance of early diagnosis and treatment initiation for non-HIV PCP patients; however, the study was limited by a small sample size of 23 patients and a retrospective single-center study design that impacted the scope and generalizability [10]. Sulfamethoxazole-trimethoprim (SMX/TMP), the first-line treatment for PCP, carries significant adverse effects in patients with non-HIV, including rash, cytopenia, and electrolyte abnormalities [11]. As a result, in patients with non-HIV PCP, the timing of treatment initiation becomes a critical clinical decision, balancing efficacy and toxicity.
Therefore, in this multi-center study, we evaluated whether an early interval from hospital admission to treatment, with adjustment for confounding factors, improved the prognosis of non-HIV PCP.
Methods
From January 2006 to March 2021, we conducted a multi-center retrospective observational cohort study to assess non-HIV PCP patients at the Kameda Medical Center, Seirei Hamamatsu General Hospital, and Seirei Mikatahara General Hospital (registry named: RE-VISION-PCP: Registry to Provide New Evidence and Insights for the Management of Pneumocystis Pneumonia in Non-HIV-infected Patients).
The inclusion criteria were non-HIV patients aged 20 years who met the diagnostic criteria for PCP. Based on previous studies and a diagnostic guideline of non-HIV PCP [11–13], we defined the diagnosis criteria of PCP as all of the following: (1) host factor: possible immunocompromised status other than HIV; 2) clinical criteria: clinical symptoms consistent with those of PCP (dyspnoea, cough, fever, and hypoxemia) and chest radiograph or chest CT scan findings compatible with PCP (including bilateral or diffuse ground-glass opacities); and (3) microbial criteria: Pneumocystis species detected in respiratory specimens, such as sputum or bronchoalveolar lavage fluid, through conventional staining (Grocott methenamine silver or Diff-Quick staining) or DNA testing (loop-mediated isothermal amplification or polymerase chain reaction), or elevated β-D-glucan concentrations with an appropriate response to standard therapy for PCP. Serum β-D-glucan concentrations were measured using either the β-D-glucan test kit (Wako Pure Chemical Industries) or the FUNGITEC G test MKII (Nissui Pharmaceutical). Elevated β-D-glucan levels were defined as concentrations > 5 pg/mL (β-D-glucan test; Wako assay) or > 20 pg/mL (FUNGITEC G-test KM assay) [14–16]. The exclusion criteria for the study were as follows: (1) patients for whom treatment had not been initiated and (2) patients who did not initiate treatment within 7 days. In previous studies, treatment of non-HIV PCP patients has typically commenced within 7 days from the day of hospitalization [7, 17], and symptoms may worsen within the first 7 days of onset [1]. Thus, in this study, it was necessary to compare the timing of treatment initiation and prognosis in cases wherein PCP treatment was appropriately administered. Therefore, patients who did not initiate treatment within 7 days of hospitalization were excluded.
This study received ethical approval and a review of the research proposal from the Institutional Review Boards of the participating institutions, including Kameda Medical Center (#21–069–230801), Seirei Hamamatsu Hospital (#3584), and Seirei Mikatahara Hospital (#21–58). This study was conducted in accordance with the principles of the Declaration of Helsinki. As this study was retrospective and the patient information was anonymized, the requirement for written informed consent was waived, and information regarding the right to opt out of the study was provided.
Exposure definition
In this study, time to treatment was defined as the duration (days) from the day of hospitalization (Day 1) to treatment initiation. The cases were divided into two groups: the ‘early treatment group,’ which initiated treatment within 2 days, and the ‘late treatment group’, which started treatment between days 3 and 7. This classification was based on the median time to treatment initiation for non-HIV PCP reported in previous studies, which is approximately 2 to 3 days [7, 17, 18]. Additionally, international guidelines recommend initiating treatment promptly upon suspicion of non-HIV PCP [19], further supporting the rationale for defining early treatment as initiation within the first 2 days of hospitalization.
Setting and treatment strategy
Based on the international treatment guideline [20], the primary treatment of choice for PCP was SMX/TMP and in cases with treatment difficulties such as allergic reactions or side effects, treatment with alternative therapeutic agents was continued. Atovaquone and pentamidine were used as second-line treatments. Steroids were administered, especially in patients with respiratory failure, as per the treatment protocol for HIV PCP [21].
Data collection
The participants’ characteristics data included age, sex, weight, hospital, underlying diseases, and immunosuppressive agents used at the time of presentation, such as glucocorticoids (including daily dosage converted to prednisolone equivalent), immunosuppressants, biologic immunosuppressive drugs, and antineoplastic drugs. Glucocorticoid use at onset was defined as the oral administration of glucocorticoids, regardless of dosage, while excluding inhaled steroids. Recorded laboratory parameters included white blood cell count, neutrophil count, lymphocyte count, hemoglobin, platelet count, albumin, LDH, sodium, potassium, and creatinine, as well as creatinine clearance. Clinical characteristics included the presence of altered consciousness, presence of hypotension, and respiratory status (without oxygen, administration of oxygen, or mechanical ventilation). Treatment-related data included the initial therapeutic agents, dosage of SMX/TMP, total treatment duration, adjunctive steroid therapy, and duration (days) from hospitalization to treatment initiation. The dosage of SMX/TMP was adjusted using a correction factor based on creatinine clearance (CrCl), as dose modification is necessary according to the severity of renal dysfunction [22]. CrCl was estimated using the Cockcroft-Gault equation [23]. The correction factors applied were as follows: 1.0 for CrCl > 50 mL/min, 1.5 for CrCl 30–50 mL/min, 2.0 for CrCl 15–30 mL/min, and 3.0 for CrCl < 15 mL/min or patients undergoing hemodialysis [22]. The use of glucocorticoids was defined as an increase in the glucocorticoid dosage compared to the dose administered prior to PCP onset. Pulse therapy with glucocorticoids was defined as the administration of ≥ 500 mg methylprednisolone for three consecutive days or more. Mortality was assessed at 30 days and 180 days. As supplementary information, data on grade 3 or higher adverse events, as defined by the Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0, associated with SMX/TMP administration in treated patients were also collected [24]. However, information on the adverse effects of other drugs, such as atovaquone and pentamidine, was not originally included in this study.
Outcomes
The primary endpoint was the 30-day mortality rate, and the secondary endpoint was the 180-day mortality rate.
Statistical analysis
As this was a retrospective observational study, a sample-size calculation was not performed. Although one case had missing data for neutrophil and lymphocyte counts, these variables were not used for covariate adjustment. Continuous and categorical variables are presented as mean ± standard deviation and frequency (proportion), respectively. Intergroup comparisons were conducted using the Student’s t-test for continuous variables and the chi-square test for categorical variables. The baseline characteristics of the patients’ backgrounds and severity were compared between the early and late treatment groups. Balance in terms of baseline characteristics between the early and late treatment groups was evaluated using the standardized mean difference (SMD). Generally, a group is considered balanced when the SMD is < 0.1 [25]. To obtain a risk-adjusted cohort, inverse probability of treatment weighting (IPTW) with propensity scores was applied [25]. Propensity scores were calculated using logistic regression with exposure as the dependent variable and age, sex, hospital, prior malignancies, serum albumin levels, LDH levels, creatinine clearance, and respiratory status. These explanatory variables were chosen based on the results of hospital clustering and prognostic factors for non-HIV PCP [5, 19]. After IPTW, each patient was assigned a weight, resulting in an adjusted cohort size that may differ from the original sample size and may contain decimal values. The adjusted cohort size reflects the reweighted sample rather than the actual number of individuals. Subsequently, patient outcomes were compared between the early and late treatment groups. In addition, we conducted a subgroup analysis restricted to patients requiring oxygen supplementation to compare outcomes between the early and late treatment groups in severe cases. The significance level was set at p < 0.05.
Sensitivity analysis
We conducted a sensitivity analysis by truncating extreme weights. Specifically, following a previous study, we truncated the IPTW at the 1st and 99th percentiles [26]. Using these trimmed weights, we repeated the analysis in the overall population as well as in the subgroup requiring oxygen supplementation.
Results
Between 1 January 2006 and 31 March 2021, 164 patients were diagnosed with non-HIV PCP after being admitted to one of the three hospitals. Five individuals were excluded because they did not receive treatment. An additional 22 patients were excluded because they did not commence treatment within 7 days of hospitalization. Ultimately, 137 patients began treatment for non-HIV PCP within 7 days of hospital admission. All the eligible patients were treated with anti-PCP medications. The early and late treatment groups comprised 94 and 43 patients, respectively (Fig. 1).
Fig. 1. Patient selection flowchartHIV, human immunodeficiency virus; PCP, Pneumocystis jirovecii pneumonia
Patient characteristics are presented in Table 1. Among the 137 individuals in the study, the average time-to-treatment for the early treatment and late treatment groups was 0.13 (± 0.34) and 3.63 (± 1.45) days, respectively. Patient backgrounds before and after conducting weighted propensity score matching are described in ‘Before adjustment’ and ‘After adjustment,’ respectively. As expected with IPTW, the adjusted cohort size appears larger than the original sample size due to the assigned weights and included decimal values, reflecting the fractional nature of the population count, which helps balance covariates across groups. Before adjustment, an SMD greater than 0.1 was observed for several variables, including female sex, weight, hospital, underlying diseases, immunosuppressive agents used, hemoglobin, albumin, LDH, serum sodium, serum potassium, creatinine clearance, altered consciousness, hypotension, and respiratory status. Details of immunosuppressants and biologic immunosuppressive drugs in unadjusted cohort are shown in Supplementary Table 1. Regarding underlying diseases, a higher proportion of patients with malignancy was observed in the late treatment group. After adjustment, the SMD was reduced to less than 0.1 for most adjustment variables, such as age, sex, hospital, malignancy, albumin, LDH, and creatinine clearance. However, the SMD for respiratory status remained above 0.1, indicating residual imbalance for this variable.
Table 1. Baseline characteristics of the study populationUnadjusted patient cohortAdjusted patient cohortEarly treatment group, n = 94Late treatment group, n = 43SMDEarly treatment group, n = 136.24Late treatment group, n = 135.81SMDAge, years71.03 (10.43)70.42 (8.59)0.06470.86 (10.47)70.43 (8.18)0.045Female54 (57.4)22 (51.2)0.12674.1 (54.4)72.3 (53.2)0.023Weight, kg52.00 (11.08)54.70 (12.13)0.23252.47 (10.94)53.35 (12.09)0.077Hospital Kameda Medical Center49 (52.1)25 (58.1)0.41472.8 (53.5)67.9 (50.0)0.083 Seirei Hamamatsu General Hospital37 (39.4)10 (23.3)47.6 (34.9)52.9 (38.9) Seirei Mikatahara General Hospital8 (8.5)8 (18.6)15.8 (11.6)15.0 (11.0)Underlying diseases Malignancy14 (14.9)11 (25.6)0.26824.8 (18.2)24.2 (17.8)0.009 Hematologic malignancy6 (6.4)5 (11.6)0.18410.1 (7.4)11.8 (8.7)0.047 Solid tumor9 (9.6)7 (16.3)0.20116.2 (11.9)14.1 (10.4)0.046 Connective tissue disease80 (85.1)28 (65.1)0.475112.9 (82.9)101.5 (74.8)0.199Immunosuppressive agents used Glucocorticoids58 (61.7)30 (69.8)0.17184.3 (61.9)90.5 (66.6)0.098 Glucocorticoid dose converted to prednisolone equivalent, mg/day12.26 (12.87)13.76 (13.53)12.03 (12.92)13.19 (13.26) Immunosuppressant70 (74.5)23 (53.5)0.44899.2 (72.8)88.6 (65.2)0.164 Biologic immunosuppressive drugs28 (29.8)10 (23.3)0.14837.7 (27.7)39.8 (29.3)0.035 Antineoplastic drugs5 (5.3)7 (16.3)0.3599.0 (6.6)15.5 (11.4)0.169Blood test findings White blood cell count, /µL8724.68 (4808.22)8853.95 (5067.86)0.0268979.85 (5131.52)9313.04 (5624.81)0.062 Neutrophil count ^a^, /µL6579.19 (3295.39)6799.71 (3697.74)0.0636653.96 (3279.26)6885.67 (3678.86)0.066 Lymphocyte count ^a^, /µL1146.43 (1157.49)1173.61 (1376.02)0.0211136.16 (1097.80)1383.34 (1817.69)0.165 Hemoglobin, g/dL11.74 (1.96)11.36 (1.74)0.20211.75 (1.94)11.38 (1.72)0.197 Platelet count, ×10⁴/µL21.39 (10.11)22.11 (10.12)0.07221.39 (9.98)22.65 (9.52)0.129 Albumin, g/dL3.07 (0.60)2.94 (0.63)0.2183.04 (0.60)3.07 (0.64)0.049 Lactate dehydrogenase, IU/L400.01 (151.99)417.88 (164.33)0.113408.42 (161.70)411.57 (151.22)0.020 Serum sodium, mEq/L137.39 (3.68)137.86 (5.24)0.103137.18 (3.62)137.39 (4.72)0.048 Serum potassium, mEq/L4.29 (0.49)4.07 (0.45)0.4634.29 (0.49)4.15 (0.40)0.302 Creatinine, mg/dL1.12 (1.30)1.10 (1.82)0.0111.11 (1.31)1.18 (1.91)0.046 Creatinine clearance, mL/min57.85 (26.47)64.31 (29.30)0.23159.24 (26.61)58.69 (27.05)0.021Altered consciousness1 (1.1)0 (0.0)0.1472.2 (1.6)0.0 (0.0)0.180Hypotension (systolic pressure < 90 mmHg)3 (3.2)0 (0.0)0.2573.0 (2.2)0.0 (0.0)0.212Respiratory status0.2510.138 Without oxygen59 (62.8)23 (53.5)82.9 (60.8)87.5 (64.4) Administration of oxygen34 (36.2)20 (46.5)52.4 (38.4)48.3 (35.6) 1–4 L/min23 (24.5)10 (23.3)33.5 (24.6)23.9 (17.6) 5–10 L/min4 (4.3)6 (14.0)5.9 (4.3)12.5 (9.2) 11–15 L/min7 (7.4)4 (9.3)12.9 (9.5)11.9 (8.8) Mechanical ventilation1 (1.1)0 (0.0)1.0 (0.7)0.0 (0.0)Time from admission to treatment initiation0.13 (0.34)3.63 (1.45)3.3310.14 (0.35)3.55 (1.50)3.142Initial therapeutic agents0.0690.168 SMX/TMP85 (90.4)38 (88.4)124.3 (91.2)116.7 (85.9) Dose of SMX/TMP administration, mg/kg/d17.71 (13.55)15.64 (9.43)17.10 (12.59)17.67 (11.00) Atovaquone7 (7.4)4 (9.3)9.4 (6.9)15.5 (11.4) Pentamidine2 (2.1)1 (2.3)2.6 (1.9)3.5 (2.6)Total treatment duration17.36 (6.91)19.86 (12.30)0.25116.96 (7.08)18.91 (11.15)0.209Adjunctive glucocorticoid therapy None10 (10.6)7 (16.3)0.16613.6 (10.0)21.1 (15.5)0.168 Yes (mild-to-moderate dose)29 (30.9)18 (41.9)0.23043.8 (32.2)51.4 (37.8)0.119 Yes (steroid pulse therapy)55 (58.5)18 (41.9)0.33878.8 (57.9)63.3 (46.6)0.227Continuous and categorical variables are expressed as the mean ± standard deviation and number (%), respectivelyAdjusted totals and numbers represent the effective sample size and event counts after inverse probability weighting, where each patient contributes a fractional weight rather than a discrete count^a^ Missing data were observed in one case each for neutrophil and lymphocyte countsSMD, standardized mean difference: SMX/TMP, Trimethoprim-sulfamethoxazole
Data on the primary and secondary endpoints are presented in Table 2. Before adjustment, the 30-day mortality rates were 11.7% and 11.6% in the early and late treatment groups, respectively (p = 1.000). At 180 days, the mortality rates were 19.1% and 25.6% in the early and late treatment groups, respectively (p = 0.529). After adjustment, there were no significant differences in the 30-day mortality (14.0% vs. 8.2%, p = 0.307) and 180-day mortality rates (21.5% vs. 17.7%, p = 0.600) between the early and late treatment groups. Data on CTCAE grade 3 or higher adverse events associated with SMX/TMP administration in the unadjusted cohort of treated patients are presented in Supplementary Table 2. Rash, hyponatremia, hyperkalemia, and nausea were the most frequently observed adverse effects, with approximately half of the patients experiencing CTCAE grade 3 or higher toxicity.
Table 2. Summary of clinical outcomesUnadjusted patient cohortAdjusted patient cohortEarly treatment group, n = 94Late treatment group, n = 43 P Early treatment group, n = 136.2Late treatment group, n = 135.8 P Primary endpoint 30-day mortality11 (11.7)5 (11.6)1.00019.0 (14.0)11.1 (8.2)0.307Secondary 180-day mortality18 (19.1)11 (25.6)0.52929.3 (21.5)24.1 (17.7)0.600Categorical variables are expressed as number (%)Adjusted totals and numbers represent the effective sample size and event counts after inverse probability weighting, where each patient contributes a fractional weight rather than a discrete count
Next, we performed a subgroup analysis restricted to patients requiring oxygen supplementation. The early treatment and late treatment groups included 35 and 20 patients, respectively. Patient characteristics of the subgroup are presented in Table 3. Before adjustment, an SMD greater than 0.1 was identified for several variables, including female sex, weight, hospital, underlying diseases, immunosuppressant, biologic immunosuppressive drugs, antineoplastic drugs, white blood cell count, neutrophil count, lymphocyte count, hemoglobin, albumin, LDH, serum sodium, serum potassium, creatinine clearance, hypotension, and respiratory status. Following adjustment, the SMD was reduced to below 0.1 for key variables such as age, malignancy, albumin, and LDH, indicating improved balance in these factors. The data on primary and secondary endpoints derived from the subgroup analysis are shown in Table 4. After weighting, the 30-day mortality (24.8% vs. 17.6%, p = 0.577) and the 180-day mortality rates (33.9% vs. 40.0%, p = 0.691) showed no significant difference between the early and late treatment groups.
Table 3. Baseline characteristics of the subgroup requiring oxygen supplementationUnadjusted patient cohortAdjusted patient cohortEarly treatment group, n = 35Late treatment group, n = 20SMDEarly treatment group, n = 52.38Late treatment group, n = 49.63SMDAge, years71.89 (9.48)72.60 (8.04)0.08172.12 (9.55)72.54 (7.43)0.050Female16 (45.7)11 (55.0)0.18723.8 (45.4)26.9 (54.1)0.175Weight, kg53.20 (10.92)55.25 (11.31)0.18453.15 (10.79)54.80 (11.39)0.149Hospital Kameda Medical Center27 (77.1)17 (85.0)0.46942.0 (80.2)38.2 (76.9)0.207 Seirei Hamamatsu General Hospital8 (22.9)2 (10.0)10.4 (19.8)10.5 (21.1) Seirei Mikatahara General Hospital0 (0.0)1 (5.0)0.0 (0.0)1.0 (2.0)Underlying diseases Malignancy8 (22.9)8 (40.0)0.37615.4 (29.4)14.5 (29.2)0.004 Hematologic malignancy4 (11.4)3 (15.0)0.1067.4 (14.1)4.9 (9.9)0.131 Solid tumor4 (11.4)6 (30.0)0.4718.0 (15.3)11.4 (22.9)0.196 Connective tissue disease28 (80.0)9 (45.0)0.77539.4 (75.2)28.4 (57.2)0.387Immunosuppressive agents used Glucocorticoid26 (74.3)15 (75.0)0.01637.9 (72.3)42.5 (85.7)0.333 Glucocorticoid dose converted to prednisolone equivalent12.60 (14.71)13.54 (14.66)11.81 (13.57)14.60 (14.73) Immunosuppressant23 (65.7)5 (25.0)0.89632.8 (62.5)17.6 (35.5)0.561 Biologic immunosuppressive drugs5 (14.3)1 (5.0)0.3197.1 (13.6)2.0 (4.0)0.343 Antineoplastic drugs4 (11.4)5 (25.0)0.3577.9 (15.0)9.6 (19.3)0.114Blood test findings White blood cell count, /µL9670.29 (5173.56)8754.50 (3879.33)0.20010799.59 (6781.78)8975.83 (3767.54)0.332 Neutrophil count^a^, /µL7486.90 (3161.21)7139.82 (3078.48)0.1117676.17 (3285.66)7374.73 (3071.01)0.095 Lymphocyte count^a^, /µL1015.71 (716.18)921.35 (556.70)0.1471072.61 (743.18)967.53 (646.42)0.151 Hemoglobin, g/dL11.91 (2.23)11.70 (1.23)0.11411.79 (2.12)11.91 (1.24)0.068 Platelet count (×10⁴/µL)22.59 (11.54)21.76 (9.54)0.07822.35 (11.30)22.22 (10.34)0.012 Albumin, g/dL2.80 (0.54)2.68 (0.56)0.2162.77 (0.53)2.73 (0.52)0.072 Lactate dehydrogenase, IU/L418.34 (166.91)467.85 (188.61)0.278443.49 (189.98)450.92 (166.73)0.042 Serum sodium, mEq/L137.26 (4.07)139.50 (6.53)0.412136.96 (3.91)139.82 (5.30)0.615 Serum potassium, mEq/L4.22 (0.50)3.98 (0.50)0.4664.22 (0.53)4.13 (0.44)0.186 Creatinine, mg/dL1.34 (1.76)0.78 (0.27)0.4441.19 (1.59)0.80 (0.21)0.341 Creatinine clearance, mL/min54.60 (26.19)68.98 (28.82)0.52258.09 (26.20)62.82 (22.99)0.192Altered consciousness0 (0.0)0 (0.0)< 0.0010 (0.0)0 (0.0)< 0.001Hypotension (systolic pressure < 90 mmHg)2 (5.7)0 (0.0)0.3482.0 (3.8)0.0 (0.0)0.282Respiratory status0.2430.197 Administration of oxygen34 (97.1)20 (100.0)51.4 (98.1)49.6 (100.0) 1–4 L/min23 (65.7)10 (50.0)31.8 (60.8)21.5 (43.4) 5–10 L/min4 (11.4)6 (30.0)5.5 (10.4)14.5 (29.3) 11–15 L/min7 (20.0)4 (20.0)14.1 (26.9)13.6 (27.4) Mechanical ventilation1 (2.9)0 (0.0)1.0 (1.9)0.0 (0.0)Time from admission to treatment initiation0.11 (0.32)3.10 (1.12)3.6250.11 (0.32)2.91 (1.09)3.475Initial therapeutic agents0.0320.191 SMX/TMP33 (94.3)19 (95.0)49.3 (94.2)44.1 (89.0) Dose of SMX/TMP administration, mg/kg/d16.03 (7.21)12.49 (6.74)15.49 (6.87)13.74 (6.51) Atovaquone2 (5.7)1 (5.0)3.0 (5.8)5.5 (11.0)Total treatment duration16.71 (8.65)20.15 (11.23)0.34316.09 (8.64)21.58 (14.33)0.464Adjunctive glucocorticoid therapy None1 (2.9)2 (10.0)0.2941.1 (2.0)3.9 (7.8)0.270 Yes (mild-to-moderate dose)15 (42.9)11 (55.0)0.24522.9 (43.7)27.2 (54.8)0.223 Yes (steroid pulse therapy)19 (54.3)7 (35.0)0.39528.4 (54.3)18.6 (37.4)0.344Continuous and categorical variables are expressed as the mean ± standard deviation and number (%), respectivelyAdjusted totals and numbers represent the effective sample size and event counts after inverse probability weighting, where each patient contributes a fractional weight rather than a discrete count^a^ Missing data were observed in one case each for neutrophil and lymphocyte countsSMD, standardized mean difference: SMX/TMP, Trimethoprim-sulfamethoxazole
Table 4. Clinical outcomes of the subgroup requiring oxygen supplementationSurvivalUnadjusted patient cohortAdjusted patient cohortEarly treatment group, n = 35Late treatment group, n = 20 P Early treatment group, n = 52.4Late treatment group, n = 49.6 P Primary endpoint 30-day mortality7 (20.0)4 (20.0)1.00013.0 (24.8)8.7 (17.6)0.577Secondary endpoint 180-day mortality11 (31.4)9 (45.0)0.47517.7 (33.9)19.9 (40.0)0.691Categorical variables are expressed as number (%)Adjusted totals and numbers represent the effective sample size and event counts after inverse probability weighting, where each patient contributes a fractional weight rather than a discrete count
Finally, we conducted a sensitivity analysis using IPTW with truncation at the 1st and 99th percentiles. Patient characteristics for the overall population after trimming are shown in Supplementary Table 3, while primary and secondary endpoints are summarized in Supplementary Table 4. The results remained largely unchanged, showing no significant differences in the 30-day mortality and 180 mortality rates between the early and late treatment groups. Similarly, the results of the sensitivity analysis in the subgroup of patients requiring oxygen supplementation are presented in Supplementary Table 5 (patient characteristics) and Supplementary Table 6 (primary and secondary endpoints). Again, no significant differences were observed in the 30-day mortality and 180-day mortality rates between the treatment groups.
Discussion
In this study, no significant differences were observed in the 30-day and 180-day mortality between the early and late treatment groups in the management of non-HIV PCP, even among the subgroup requiring oxygen. Additionally, similar results were obtained in the sensitivity analysis using IPTW with truncation at the 1st and 99th percentiles. Utilizing data from the largest multicenter cohort to date to analyze the effects of early versus late treatment, this study demonstrated that treatment delay did not impact short-term mortality outcomes in non-HIV PCP.
Similar to our study, other research has reported no prognostic difference between early treatment and later treatment. Ko et al. investigated the interval from emergency room admission to the initiation of PCP treatment in 51 patients with non-HIV PCP and respiratory failure and found no association between the time to treatment initiation and increased mortality in non-HIV PCP [18]. Our study, which focused on cases of respiratory failure (patients requiring oxygen) and comprised approximately 50 cases, demonstrated a high level of reliability consistent with Ko et al.‘s research. Conversely, two other retrospective studies (Asai et al. and Overgaard et al.) on non-HIV PCP patients indicated that the time from hospital admission to treatment initiation was associated with in-hospital mortality [9, 10]. However, these studies had limitations, including small sample sizes (ranging from 23 to 48 cases) and the use of univariate analysis without adjusting for prognostic factors related to mortality. Li et al. reported that the longer time from hospitalization to treatment initiation in non-HIV PCP compared to HIV PCP might explain the higher mortality in non-HIV PCP. However, other factors, including age and pneumonia severity index differences, may have also contributed [8]. Without adjusting for prognostic factors, it is unclear whether early treatment directly impacts prognosis. Additionally, the median time to treatment in the late group of our study was 3.63 days, whereas in the studies by Asai et al., Li et al., and Overgaard et al., the median time to treatment initiation in the mortality groups was between 8.67 and 15 days [8–10], which may have contributed to the differing results.
In this study, we observed a higher percentages of patients with malignancies in the late treatment group within the unadjusted cohort. This difference was adequately balanced in our adjusted analysis, where malignancy was included as a variable in the propensity score weighting. One possible explanation for this initial imbalance is that in patients with malignancies presenting with respiratory symptoms or pulmonary infiltrates, the differential diagnosis tends to be broader, including disease progression, drug-induced pneumonitis, various infections, and PCP [27]. Furthermore, oncologists or hematologists, who primarily manage these patients, may have limited experience with diagnosing and treating PCP, potentially contributing to delays in initiating appropriate therapy until referral to pulmonologists occurs.
SMX/TMP, the first-line treatment for non-HIV PCP, is a therapeutic option that is associated with numerous side effects [11]. In our study, approximately half of the patients who received SMX/TMP experienced CTCAE grade 3 or higher adverse events. Therefore, it is crucial to diagnose and treat non-HIV PCP appropriately rather than empirically prescribing this treatment. Prognostic factors, such as age, LDH levels, respiratory failure, malignancy, and low albumin levels, have been reported, and these factors are associated with an increased mortality rate [5, 19]. Thus, it is important to assess the disease severity in patients based on these factors and to comprehensively consider patient management.
This study includes diverse underlying conditions and has undergone sufficient adjustment for patient backgrounds, thereby presenting more accurate statistical results. Subgroup analyses based on severity were conducted to enhance external validity. However, larger prospective randomized controlled trials or cohort studies are required in the future because the study was small scale and limited severe cases.
Nevertheless, this study has some limitations. First, this was a retrospective observational study, and despite efforts to align patient backgrounds between the early and late treatment groups, there was a potential for selection bias. It cannot be ruled out that cases with mild symptoms, where observation without treatment was possible, may have selectively been included in the late treatment group. However, in the subgroup analysis of severe cases requiring oxygen at the time of admission, no significant difference was observed between the early and late treatment groups. Therefore, we speculated that the bias in patient severity was not substantial. Second, though this study examined short-term mortality outcomes, it did not evaluate long-term functional outcomes (Quality Of Life, respiratory function, and Activities of Daily Living). Therefore, the potential impact of early treatment initiation on long-term functional outcomes remains to be evaluated. Future prospective observational studies evaluating long-term outcomes are essential. Third, the inclusion of patients with diverse immunosuppressive conditions, such as autoimmune diseases, solid malignancies, hematologic malignancies, and other etiologies, inevitably introduces certain heterogeneity, potentially contributing to bias in our results. While we acknowledge this as a limitation, it reflects the real-world complexity of immunosuppression, making it difficult to fully standardize patient characteristics in such studies. Fourth, this study aimed to examine the relationship between early treatment initiation and prognosis in patients where PCP treatment was appropriately administered, specifically within 7 days, based on the descriptive from the clinical course of patients with non-HIV PCP [7, 17]. Given the rapidly progressive nature of non-HIV PCP, immediate initiation of treatment upon clinical suspicion is recommended [19]. Thus, we defined “early treatment” as therapy initiated ideally within 1 to 2 days after hospitalization [7, 17], and “late treatment” as therapy initiated between 3 and 7 days after hospitalization, representing a clinically meaningful delay. Cases where treatment began more than 7 days post-hospitalization were excluded from analysis, as such delays reflect atypical clinical practice. Thus, our findings may not be generalizable to patients whose treatment started beyond 7 days after hospitalization.
Conclusion
This study found no significant association between early treatment initiation and 30-day or 180-day mortality rates in non-HIV PCP patients compared to the late treatment initiation group. Given the considerable side effects associated with the treatment of non-HIV PCP, the results suggest that, rather than immediately resorting to empirical treatment, it is crucial to make an accurate diagnosis and implement management that is individualized based on the disease severity.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pereira-Díaz E, Moreno-Verdejo F, De La Horra C, Guerrero JA, Calderón EJ, Medrano FJ. Changing trends in the epidemiology and risk factors of Pneumocystis pneumonia in Spain. Front Public Health 2019, 7.10.3389/fpubh.2019.00275 PMC 678825631637227 · doi ↗ · pubmed ↗
- 2Li MC, Lee NY, Lee CC, Lee HC, Chang CM, Ko WC. Pneumocystis jiroveci pneumonia in immunocompromised patients: delayed diagnosis and poor outcomes in non-HIV-infected individuals. Journal of microbiology, immunology, and infection = Wei mian yu gan ran za zhi 2014, 47(1):42–47.10.1016/j.jmii.2012.08.02423063081 · doi ↗ · pubmed ↗
- 3Nagai T, Matsui H, Fujioka H, Homma Y, Otsuki A, Ito H, Ohmura S, Miyamoto T, Shichi D, Tomohisa W et al. Low-Dose vs Conventional-Dose Trimethoprim-Sulfamethoxazole Treatment for Pneumocystis Pneumonia in Patients Not Infected With HIV. CHEST 2024, 165(1):58–67.10.1016/j.chest.2023.08.00937574166 · doi ↗ · pubmed ↗
- 4Maschmeyer G, Helweg-Larsen J, Pagano L, Robin C, Cordonnier C, Schellongowski P. th European Conference on Infections in Leukemia ajvo TE Gf B, Marrow Transplantation TE Of R, Treatment of Cancer t IIHS, The European L: ECIL guidelines for treatment of Pneumocystis jirovecii pneumonia in non-HIV-infected haematology patients. J Antimicrob Chemother 2016, 71(9):2405–2413.10.1093/jac/dkw 15827550993 · doi ↗ · pubmed ↗
- 5Kosaka M, Ushiki A, Ikuyama Y, Hirai K, Matsuo A, Hachiya T, Hanaoka M. A Four-Center retrospective study of the efficacy and toxicity of Low-Dose Trimethoprim-Sulfamethoxazole for the treatment of Pneumocystis pneumonia in patients without HIV infection. Antimicrob Agents Chemother 2017, 61(12).10.1128/AAC.01173-17PMC 570035428893787 · doi ↗ · pubmed ↗