Delayed Presentation of a Cervical Spine Fracture: A Case Report
Ahmed Mahmood, Moustafa Abouelkheir

TL;DR
A man in his seventies had a delayed diagnosis of cervical spine fractures after a minor car accident.
Contribution
This case highlights the importance of thorough follow-up in trauma patients with potential spinal injuries.
Findings
The patient was initially discharged after a minor injury.
Delayed symptoms led to the discovery of multiple cervical fractures.
The case emphasizes the risk of missed spinal injuries in trauma patients.
Abstract
The unique anatomy and flexibility of the cervical spine (C-spine) pose a risk of injury. Trauma to the C-spine encompasses a diverse range of injuries, ranging from minor muscular strains to life-threatening fractures and dislocations associated with spinal cord lesions. This case report concerns a man in his seventies who presented to the emergency department immediately after a road traffic collision with only a minor laceration on his forehead. The patient was discharged after a thorough evaluation and returned the next day, reporting left-hand paresthesia, although the examination yielded no significant findings. This prompted further investigations to confirm multiple cervical vertebrae fractures later.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
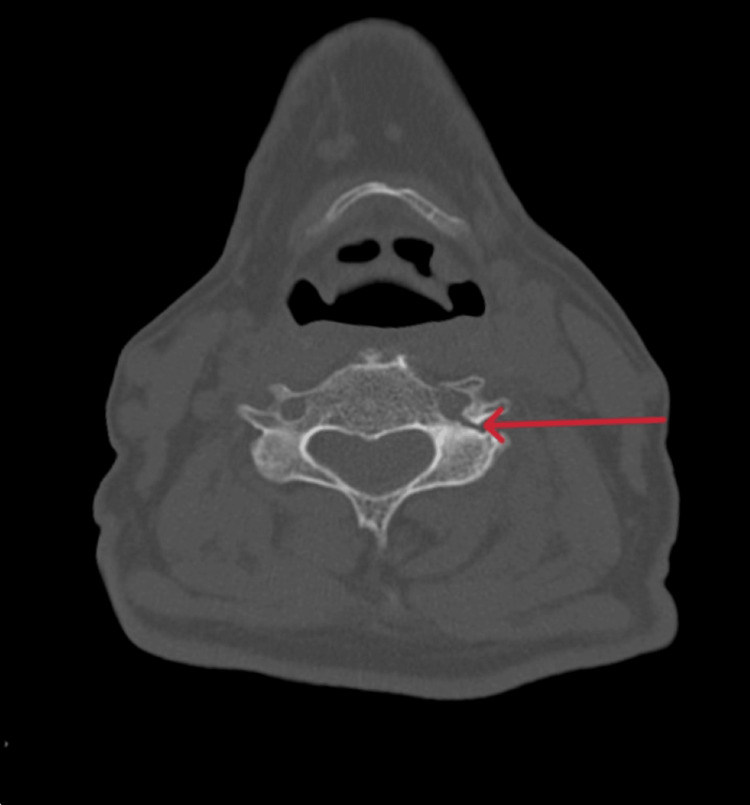 Figure 1
Figure 1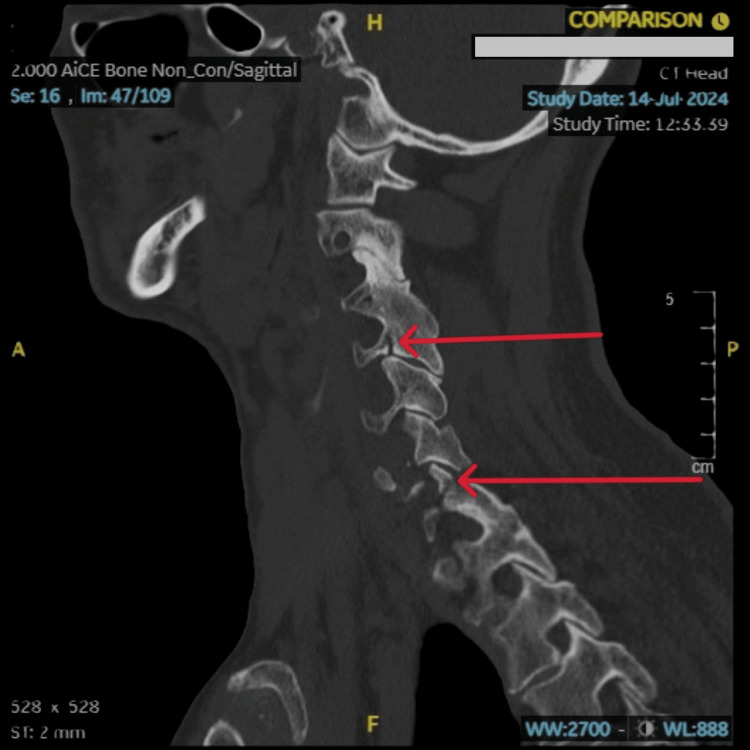 Figure 2
Figure 2 Figure 3
Figure 3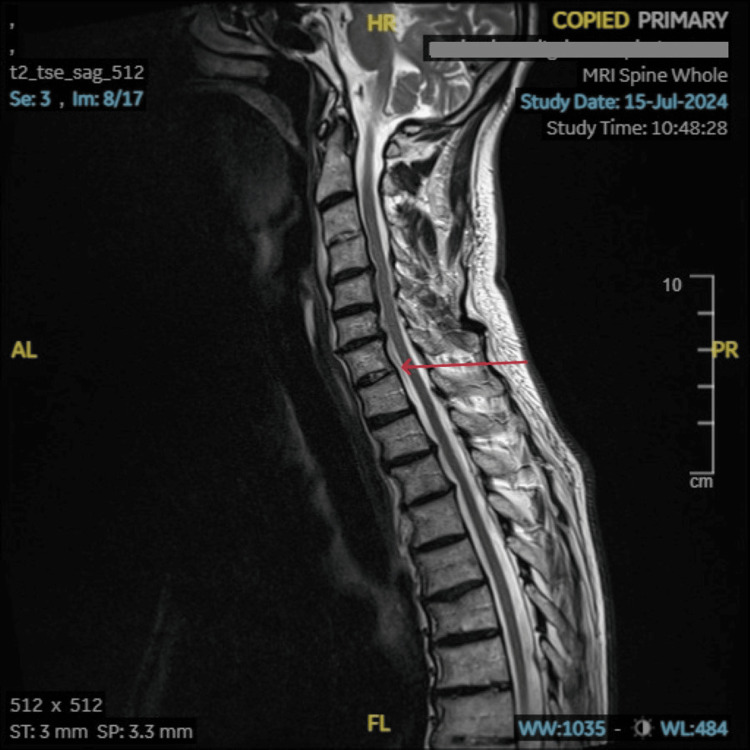 Figure 4
Figure 4| Parameters | Results | Reference values |
| Sodium | 135 | 133-146 (mmol/L) |
| Potassium | 4.5 | 3.5-5.3 (mmol/L) |
| Urea | 3.9 | 2.5-7.4 (mmol/L) |
| Creatinine | 70 | 59-104 (umol/L) |
| Glomerular filtration rate | 89 | 90-200 (mL/min) |
| Glucose | 15.8 | 3.0-6.0 (mmol/L) |
| Adjusted calcium | 2.48 | 2.20-2.60 (mmol/L) |
| C-reactive protein | 2.1 | 0-5 (mg/L) |
| Hemoglobin | 133 | 132-170 (g/L) |
| White cell count | 6.3 | 4.3-11.2 10^9 /L |
| Platelets | 4.63 | 150-400 10^9 /L |
| Investigation | Result |
| CT scan of the brain and spine | No CT evidence of acute intracranial injury/bleeding; Minimally displaced fracture of C4 left foramen transversarium; Mildly displaced fracture of left superior articular facet of C7 vertebra, with minimal diastasis of left-sided C6-7 facet joint; Undisplaced fracture of the left foramen transversarium of the C7 vertebra; Diminished intervertebral disc spaces at multiple cervical levels; No evidence of fracture of the cervical vertebral bodies or post-traumatic collapse |
| Intracranial CT angiogram | No evidence of arterial occlusion or dissection. |
| CT angiogram of the aortic arch | No evidence of arterial occlusion or dissection. |
| MRI of the spine | Degenerative changes involving the spine with disc degenerative changes as described above associated with indentation of the cord at C4-C5 and C5-C6 levels. No definite signal abnormality involving the cervical spinal cord at this level. Fracture with surrounding marrow edema/contusion of the left superior articular process at the C7 level, minimally displaced fracture involving the left transverse process of C4 with involvement of the left transverse foramina, and undisplaced fracture involving the left transverse process at C7 (correlated with CT scan). Minimal edema involving either aspect of the C6-C7 level intervertebral disc and pre-vertebral edema in the cervical spine. |
| Nexus C-Spine criteria | |
| No posterior midline cervical spinal tenderness | If YES to all, then no radiography is required. If NO to any question then radiography is required. |
| No evidence of intoxication | |
| Normal level of alertness | |
| No focal neurological deficit | |
| No painful distracting injuries | |
| The Canadian C-Spine rule | |
| Any high-risk factor? Age at least 65 years or dangerous mechanisms (including falls from at least 1 meter or 5 stairs, axial load to head such as diving, high-speed collision, rollover, ejection from vehicle bicycle collision, motorized recreational vehicles) or paraesthesia in extremities | If yes to any, then needs radiological investigation |
| Any low-risk factor that allows safe assessment of the range of motion? Simple rear-end motor vehicle collision (excluding rollover, hit by a high-speed vehicle, hit by a large vehicle, pushed into oncoming traffic) or sitting position in an emergency department or ambulatory at any time or delayed onset of neck pain or absence of midline C-spine tenderness | If no to any, then needs radiological investigation |
| Able to actively rotate neck? | If unable to rotate neck, then needs radiological investigation |
| If there is no high-risk factor, there is a low-risk factor that allows safe assessment of range of motion and the patient can actively rotate the neck, then there is no need for radiological investigation. | |
| Sub-axial Injury Classification and Severity Scale (SLICS) | |||
| Category | Parameter | Description | Points |
| 1 | Injury morphology | Compression | 1 |
| Burst | 2 | ||
| Distraction | 3 | ||
| Rotation/translation | 4 | ||
| 2 | Disco-ligamentous complex integrity | Intact | 0 |
| Suspected disruption | 1 | ||
| Disruption | 2 | ||
| 3 | Neurological status | Intact | 0 |
| Nerve root injury | 1 | ||
| Complete cord injury | 2 | ||
| Incomplete cord injury | 3 | ||
| Persistent cord injury | +1 | ||
| Management plan according to points | |||
| 1-3 points | Non-surgical management | ||
| 4 points | Surgical or non-surgical management | ||
| 5-10 points | Surgical management | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Fractures and Fixation Techniques · Spine and Intervertebral Disc Pathology · Pelvic and Acetabular Injuries
Introduction
The cervical spine (C-spine) is a dynamic structure located in the neck that safeguards the nerve innervation extending to the body and facilitates unrestricted movement of the head and neck. However, it is also susceptible to injuries. Cervical spine trauma constitutes a variety of injuries ranging from mild ligamentous or muscular strains to serious fractures or dislocations of bony vertebrae, which can result in significant spinal cord injury. Fractures of the C-spine are a leading cause of mobility loss and fatalities among trauma patients, responsible for 56% of cervical spinal cord injuries and approximately 500 to 600 people enduring acute traumatic spinal cord injury every year in the United Kingdom [1, 2].
Variations in underlying mechanisms such as hyperflexion, hyperextension, axial loading, rotational, and distraction forces predispose the C-spine to injuries [3]. Cervical spine injuries are commonly associated with trauma such as falls, road traffic collisions, sports-related diving injuries, and penetrating or blunt trauma [3]. Nevertheless, non-traumatic C-spine injuries can also occur, such as compression fractures from osteoporosis, arthritis, cancer, or inflammation of the spinal cord [3]. Passias et al. showed that road traffic collisions were the most prevalent cause in the United States, responsible for 29.3% of C-spine fractures and most frequently occurring at the C2 (32.0%) and C7 (20.9%) levels [4].
In some instances, injuries to the C-spine may go unnoticed during the initial assessment or may present symptoms at a later time. Given that the full extent of the injury may not be immediately apparent, it is essential for all patients suspected of C-spine trauma to receive a comprehensive evaluation using a standardized approach. This is vital for enhancing patient outcomes and preventing serious complications, including paralysis and death.
Case presentation
A 73-year-old male patient presented to the accident and emergency department following a low-speed (20 mph) collision with a stationary vehicle. He was in the front passenger seat wearing his seatbelt and extricated himself after the crash. Upon initial assessment, he had only a 3 cm laceration on the right side of his forehead above the eye, which did not expose bone. He reported no loss of consciousness and was able to recall the entire incident in detail, without any neurological deficit or cervical spine tenderness. Consequently, the National Emergency X-ray Utilization Study (NEXUS) score was determined to be 0. Primary closure of the wound was performed with Prolene 5-0 surgical sutures (Ethicon, part of J&J MedTech, Raritan, NJ) under aseptic conditions and local anesthesia. He was discharged with reassurance and appropriate safety netting, which included monitoring for red flag symptoms indicative of potential neck or head injury, such as paresthesia and paralysis of any limb, severe headache despite adequate analgesia, persistent vomiting, coordination issues, seizures, and lastly, coma.
Following the advice, he returned the next day to the accident and emergency department complaining of left-hand paresthesia. Upon re-assessment, there was no observable tenderness in the cervical spine or any neurological deficits. This included evaluations of deep tendon reflexes, limb strength, limb tone and range of motion, the Glasgow Coma Scale, cranial nerve function, and pupillary size and response. Additionally, he was capable of actively rotating his neck without experiencing any symptoms. The cardiovascular examination, respiratory examination, and abdominal examination were unremarkable. The presence of paresthesia, identified as a red flag symptom and a NEXUS score of one, necessitated further imaging.
The patient’s past medical history included hypothyroidism, type 1 diabetes mellitus, osteoarthritis, anxiety, and depression. He was prescribed levothyroxine 125 mcg, metformin 2 g, pravastatin 40 mg, and citalopram 10 mg to manage these conditions. He had no significant surgical history of note, and his social history consisted of him residing with his partner in their own house.
Initial investigations conducted included blood tests (Table 1) and CT scans of the brain and cervical spine (Figures 1, 2, and Table 2). After conducting initial investigations, the patient was referred to the orthopedic team for further evaluation, which included a CT angiogram of intracranial vessels, a CT angiogram of the aortic arch, and an MRI of the whole spine (Figures 3, 4, and Table 2). Following these investigations, a spinal surgery facility at a tertiary care hospital was contacted.
CT scan of the head and cervical spine The red arrow shows a minimally displaced fracture of the left foramen transversarium on an axial view of a non-contrast CT scan of the head and cervical spine.
CT scan of head and cervical spine Minimally displaced fracture of the left foramen transversarium of the C4 vertebra and mildly displaced fracture of the left superior articular facet of the C7 vertebra, with minimal diastasis of the left-sided C6-C7 facet joint on a sagittal view of a non-contrast CT scan of the head and cervical spine. These findings are marked by a red arrow on the scan.
MRI scan of the spine Fracture with surrounding marrow edema/contusion of the left superior articular process at the C7 level and an undisplaced fracture involving the left transverse process at the C7. There is minimal edema involving either aspect of the C6-C7 level intervertebral disc and prevertebral edema in the cervical spine. This is marked with a red arrow.
MRI scan of the spineA minimally displaced fracture involving the left transverse process of C4 with involvement of the left transverse foramina is seen. This is marked with a red arrow.
After an initial assessment, the patient was immediately placed on the Aspen® collar (Aspen Medical Products®, Irvine, CA) and referred to the orthopedic team for further management. The orthopedic team contacted the spinal surgery team at a tertiary trauma center, which suggested local admission for observation and conservative management, which included analgesia, hydration, and immobilization of the neck via collar application. The patient was discharged two days following presentation with outpatient follow-up.
Discussion
The C-spine is composed of seven vertebrae and serves as a protection for the spinal cord. Cervical spine injuries have the potential to cause significant and persistent disability. Cervical spine fractures can be classified based on the level involved and are typically categorized into three groups, namely C1, C2, and the sub-axial spine (C3 to C7) [2]. The sub-axial spine (C5, C6, and C7) represents 55% of C-spine injuries, followed by injury to C2 [3, 5]. The injuries are more prevalent among males and exhibit a bimodal distribution of age, with a prevalence of 15 years to 30 years and above 65 years [3].
Traumatic C-spine injuries can manifest in a diverse range of symptoms, including neck pain, neck stiffness, headache, dizziness, visual symptoms, paresthesia, limb weakness/paralysis, and respiratory compromise in the event of upper cervical fractures [6]. The goal of early detection and management of C-spine injuries, whether surgical or non-surgical, is to return to maximum functional ability, minimize residual pain, reduce any neurological deficit, and prevent further disability. Early detection can be achieved through various scoring systems such as the Canadian C-Spine rule or the NEXUS low-risk criteria (Tables 3, 4) [7, 8].
Different studies have found the Canadian C-spine rule is superior to the NEXUS low-risk criteria for better assessment of cervical spine injury [9]. Hence, the National Institute for Health and Care Excellence (NICE) and the Royal College of Emergency Medicine (RCEM) recommend utilizing the Canadian C-spine rule over NEXUS low-risk criteria [1, 10]. When a C-spine fracture is suspected, it is important that the patient be immobilized and urgently investigated using different radiological modalities as per NICE guidelines [1].
The treatment of cervical fractures varies based on the level and extent of injury. However, it can broadly be categorized into two distinct systems, namely upper cervical spinal injuries comprising C1, C2, and sub-axial spinal injuries comprising C3-C7 [11, 12]. Since the patient had a sub-axial cervical spinal fracture, largely only its management will be discussed. The Sub-axial Injury Classification and Severity Scale (SLICS) is used to assess and determine whether surgical correction or conservative management is necessary (Table 5) [2, 13].
The occurrence of missed or delayed C-spine injuries ranges from approximately 4.9% to 20% following the initial trauma assessment [14, 15]. The primary factors contributing to these missed or delayed diagnoses include insufficient or incomplete neurological evaluations, inadequate imaging or errors in interpreting the imaging results, and the existence of distracting injuries [10, 14, 15]. To avoid the risk of missing cervical spine injuries, various standardized scoring systems have been implemented, including the Canadian C-Spine Rule and NEXUS low-risk criteria [7, 8].
On the initial presentation, the NEXUS score was 0. However, subsequent presentation to the accident and emergency department revealed a NEXUS score of one, which necessitated radiological investigations, specifically a CT scan, due to its high priority as the gold standard investigation [16]. The CT scan revealed multiple sub-axial C-spine fractures, prompting the spinal team at the tertiary hospital to request an additional MRI scan to determine the severity as per the SLICS scoring system. The patient had a SLICS score of two, which reflected non-surgical or conservative management.
Conclusions
The objective of this case is to recognize the importance of early recognition of cervical spinal injuries, keeping a low threshold for investigating patients as these injuries are potentially serious and can lead to devastating consequences if not properly treated. Moreover, implementing a standardized protocol is crucial to prevent missing a C-spine fracture. Additionally, it is imperative that a multidisciplinary team approach be utilized as early as possible. This involves collaboration between emergency physicians, radiologists, orthopedic surgeons, spinal surgeons, nursing staff, and paramedics to provide comprehensive management to reduce patient mortality, morbidity, and disability.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Spinal Injury: Assessment and Initial Management National Clinical Guideline Centre London, UK National Clinical Guideline Centre 2016 https://www.nice.org.uk/guidance/ng 41/evidence/full-guideline-2358425776
- 2Cervical Spine Fractures Overview Mc Mordie JH Viswanathan VK Gillis CC Treasure Island, FL Stat Pearls [Internet], Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 448129/28846229 · pubmed ↗
- 3Cervical Injury Torlincasi AM Waseem M Treasure Island, FL Stat Pearls [Internet], Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 448146/28846253 · pubmed ↗
- 4Traumatic fractures of the cervical spine: analysis of changes in incidence, cause, concurrent injuries, and complications among 488,262 patients from 2005 to 2013 World Neurosurg Passias PG Poorman GW Segreto FA 037110201810.1016/j.wneu.2017.11.01129138069 · doi ↗ · pubmed ↗
- 5Surgical treatment of upper, middle and lower cervical injuries and non-unions by anterior procedures Eur Spine J Aebi M 0919 Suppl 1201010.1007/s 00586-009-1120-8PMC 289972219826842 · doi ↗ · pubmed ↗
- 6Pathology and treatment of traumatic cervical spine syndrome: whiplash injury Adv Orthop Tanaka N Atesok K Nakanishi K Kamei N Nakamae T Kotaka S Adachi N 4765050201820182968235410.1155/2018/4765050 PMC 5851023 · doi ↗ · pubmed ↗
- 7Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography Utilization Study Group N Engl J Med Hoffman JR Mower WR Wolfson AB Todd KH Zucker MI 949934320001089151610.1056/NEJM 200007133430203 · doi ↗ · pubmed ↗
- 8The Canadian C-spine rule for radiography in alert and stable trauma patients JAMA Stiell IG Wells GA Vandemheen KL 1841184828620011159728510.1001/jama.286.15.1841 · doi ↗ · pubmed ↗