Increase in Brain-Derived Neurotrophic Factor After Cycling Exercise Resisting Electrically Stimulated Antagonist Muscle Contractions in Overweight Japanese People: A Randomized, Controlled, Single-Blind, Crossover Trial
Takahiro Sugimoto, Ryuki Hashida, Sohei Iwanaga, Eriko Baba, Masayuki Omoto, Dan Nakano, Sachiyo Yoshio, Takumi Kawaguchi, Hiroo Matsuse

TL;DR
A new exercise method combining cycling with electrical stimulation increases brain-derived neurotrophic factor more than regular cycling in overweight individuals.
Contribution
The study introduces a hybrid exercise method that significantly boosts BDNF levels in overweight people compared to traditional cycling.
Findings
HERG significantly increased BDNF levels more than CERG in overweight individuals.
Both HERG and CERG increased BDNF and lactate levels after exercise.
Lactate levels did not differ significantly between HERG and CERG.
Abstract
Background: A hybrid training system (HTS) combining antagonist muscle electrical stimulation and voluntary muscle contraction has been developed using electrically stimulated eccentric antagonist muscle contractions. The exercise method that combines a conventional cycle ergometer with HTS (HERG) adds additional exercise intensity to the conventional cycle ergometer through electrical stimulation. Exercise-induced brain-derived neurotrophic factor (BDNF) production appears to have neuroprotective effects and contributes to improved metabolic regulation. Changes in BDNF after exercise are related to exercise intensity. Therefore, combining a cycle ergometer with electrical stimulation may be an effective approach. Purpose: The purpose of this study was to evaluate the effect of the HERG on BDNF secretion. Participants and methods: Fourteen healthy adults participated in the study. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
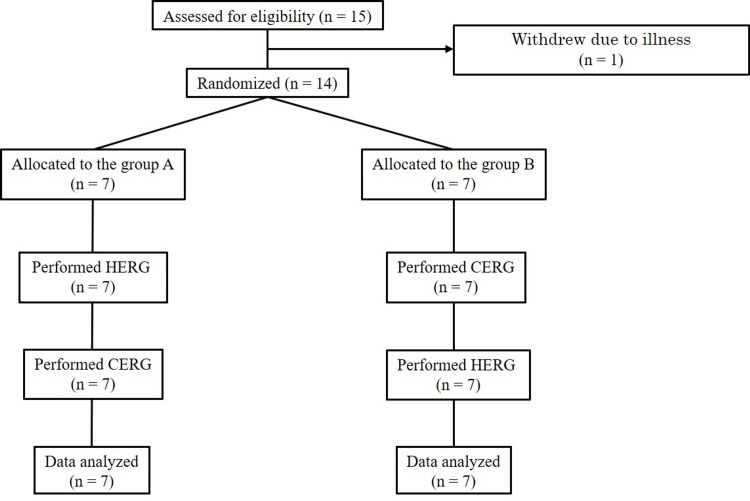 Figure 1
Figure 1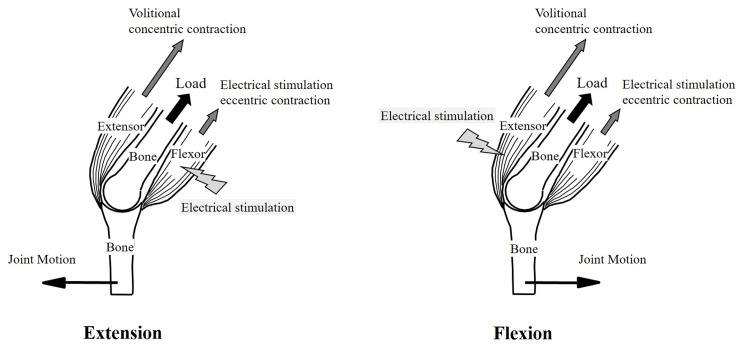 Figure 2
Figure 2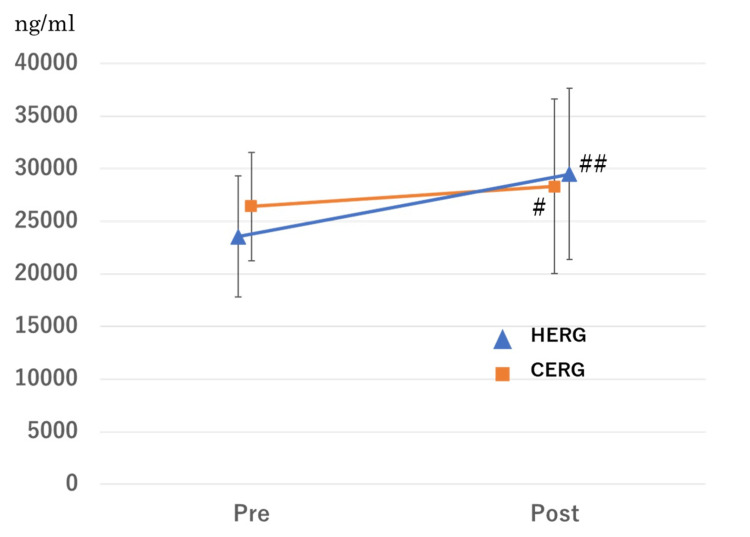 Figure 3
Figure 3| Mean±SD | |
| Number | N/A |
| Age (years) | 29±6.6 |
| Body weight (kg) | 68.6±9.1 |
| Height (cm) | 170.0±6.2 |
| BMI (kg/m2) | 23.6±2.7 |
| VO2 peak (ml/kg/min) | 31.3±4.2 |
| HERG | CERG | p-value# | |
| BDNF (ng/ml) | Δ5501.0±7963.8 | Δ1921.3±5308.2 | p=0.0339 |
| Lactate (mmol/l) | Δ0.85±1.2 | Δ0.73±1.4 | p=0.8632 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMuscle activation and electromyography studies · Transcranial Magnetic Stimulation Studies · Children's Physical and Motor Development
Introduction
Aerobic exercises, such as using an ergometer, generally have high energy expenditure during the exercise and are effective in reducing body fat, increasing maximal oxygen uptake, improving exercise tolerance, and enhancing metabolic function. Furthermore, the ergometer is widely utilized as an exercise therapy not only for healthy individuals but also for those with relatively high exercise risks and low exercise tolerance, such as patients with musculoskeletal disorders, cardiovascular diseases, metabolic disorders, and frail elderly individuals [1-4]. This is because it allows for easy adjustment of exercise intensity and places less mechanical load on the lower joints compared with other types of aerobic exercises [5]. Therefore, ergometer exercise is particularly beneficial for individuals who require exercise, such as those with chronic conditions or overweight (obesity) at risk of joint disorders. These exercise benefits are more effective with higher exercise intensity [6]. However, when exercise tolerance is low, engaging in relatively high-intensity exercise can be challenging. Therefore, there is a need for exercise methods that are both feasible and more effective for patients with reduced exercise tolerance.
The mechanisms underlying the effects of exercise include the influence of myokines secreted by skeletal muscles during physical activity. One of these myokines is brain-derived neurotrophic factor (BDNF) [7]. In recent years, BDNF has been shown to have a relationship with metabolic function [7,8] and nutritional status [9]. BDNF secreted from skeletal muscles during exercise is considered an important factor in improving mitochondrial function [10]. In individuals with metabolic syndrome, the increase in BDNF levels after exercise has been shown to be associated with exercise benefits, including improvements in muscle strength [11], insulin resistance [12], and depressive symptoms [13]. BDNF has been shown to acutely increase immediately after exercise in the short term and to sustain elevated levels with regular exercise in the long term, potentially contributing to improvements in glucose and lipid metabolism induced by exercise [14]. Therefore, exercise that effectively stimulates sufficient BDNF secretion is preferable for individuals with metabolic syndrome or those who are overweight and at high risk of developing it. However, the magnitude of change in BDNF levels after aerobic exercise depends on the intensity of the exercise [15]. The increase in BDNF after exercise is observed in both obese and non-obese individuals. However, since the total relative energy expenditure at the same aerobic exercise intensity is significantly lower in obese individuals compared to non-obese individuals, the post-exercise BDNF response at a similar exercise intensity may be insufficient for improving insulin resistance or carbohydrate and fat utilization in obese individuals [16]. Therefore, obese individuals with low exercise tolerance may find it challenging to engage in exercise at a sufficient intensity to induce effective changes in BDNF levels after exercise. Thus, exercises that can increase BDNF levels even at relatively low intensity would be beneficial.
It has been reported that combining neuromuscular electrical stimulation (NMES) with voluntary contractions is more effective than using either NMES or voluntary contractions alone [17]. The hybrid training system (HTS) is an exercise that combines NMES with voluntary contractions simultaneously during exercises [18]. Using an ergometer for aerobic exercise has been tested and shown to work well with NMES [19]. We reported that oxygen uptake could be increased during ergometer exercise without increasing the workload by combining it with NMES [20]. Furthermore, it has been reported that HTS can improve insulin resistance and liver function in patients with non-alcoholic fatty liver disease [21]. Therefore, performing HTS simultaneously during exercise may be effective in stimulating BDNF secretion. It has also been reported that higher BMI is associated with BDNF secretion after exercise [21]. Consequently, it is hypothesized that a cycling ergometer combined with HTS (HERG) would be particularly effective as a stimulus for BDNF secretion in individuals with a higher BMI. In this study, we investigated the immediate effect of HERG on serum BDNF levels after exercise, taking into account the influence of BMI. By examining the immediate increase in BDNF after HERG in this study, we indirectly assess the potential long-term exercise effects of HERG.
Materials and methods
Participants
Fifteen healthy young men (mean±standard deviation (SD): age 29.4±6.5 years; height 170.0±6.1 cm; body mass 68.2±8.9 kg) agreed to participate. All participants were given an explanation of the purpose and methods of the study, both verbally and in writing, and written consent to participate in this study was obtained. The inclusion criteria were men aged 20 years or older, with no current medical conditions requiring treatment and no limitations in daily activities.
The exclusion criteria included a history of musculoskeletal disorders, cardiovascular disease, respiratory disease, neuromuscular disorders, and neuropsychiatric disorder. All participants first underwent a medical examination and cardiopulmonary exercise tests (CPX) conducted by a physician and/or physical therapist, followed by the completion of two different types of exercise sessions in a randomized order, as described later. The study was conducted in adherence with the standards of the World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects (2013 version). The Ethics Committee of Kurume University (Health Care and Medical Ethics) approved the clinical design of this study protocol (approval ID: 19055). This study was registered on the UMIN Clinical Trials Registry (UMIN000055280). The link to this study data is https://dataverse.harvard.edu/dataset.xhtml?persistentId=doi:10.7910/DVN/BYVT3U.
Study design
This study is a comparative research design using a 2×2 crossover method. Each participant performed two types of exercise: HERG and cycling ergometer alone (CERG) (Figure 1). Group A performed HERG first, while Group B performed CERG first. Participants were randomly assigned to Group A or Group B by staff members not involved in the study using a 1:1 random number generator sequence generated prior to the initiation of the study (Randomization.com). To ensure allocation concealment, computer-generated randomization and the envelope method were used. The participants were not blinded as they were aware of the type of exercise they would perform, but assessors and analysts were blinded. The washout period between the two types of exercise interventions (CERG or HERG) was set at one week, and participants were assessed (blood test) immediately before and after each exercise intervention. This study was designed in accordance with the CONSORT guidelines (www.consort-statement.org.) for reporting randomized controlled trials (Appendix, Table 3).
Diagram of participants’ flow throughout the study.HERG, conventional cycle ergometer with HTS; CERG, cycling ergometer alone.
Setting
The study was conducted in a rehabilitation room affiliated with the university hospital.
Ramp load test
To set the exercise load, CPX (Mobile aeromonitor AE-100i, Minato Medical Science Co., Ltd., Osaka, Japan) were performed to measure the anaerobic threshold (AT) and peak oxygen uptake (VO_2_peak). The ramp load test protocol was conducted based on our previous report [22]. The heart rate at the AT was set as the target heart rate for the exercise session.
CERG protocol
After a two-minute warm-up at 30W, participants performed ergometer exercise for 30 minutes at an exercise intensity corresponding to their AT. During the exercise, participants were instructed and monitored to maintain a cadence of 60-80 revolutions per minute and to maintain their target heart rate.
HERG protocol
NMES was combined with ergometer exercise simultaneously [18]. During HTS with the ergometer, as in previous studies, electrical stimulation was set so that the hamstrings were stimulated during knee extension and the quadriceps during knee flexion (Figure 2) [19]. After a two-minute warm-up at 30W, participants performed the ergometer exercise for 30 minutes. They were instructed to maintain a cadence of 60-80 revolutions per minute. In a previous study, we reported that the oxygen uptake during HERG has a linear relationship with workload similar to a conventional ergometer and that exercise intensity could be adjusted using heart rate [20]. The oxygen uptake during HERG was significantly higher than during CERG at an average of 21.2%. Based on these data, the workload was calculated (target heart rate) using a linear regression equation and adjusted during HERG to reach the same oxygen uptake as that attained during CERG. Therefore, the ratio of oxygen uptake to VO_2_peak in both the HERG and CERG groups was the same, at 40%.
HTS.HTS creates resistance to the motion of voluntarily contracting agonist muscles through the force generated by its electrically stimulated antagonist muscles. In this process, electrical stimulation induces eccentric contractions in the antagonist muscles, while voluntary muscle contractions result in concentric contractions in the agonist muscles. HTS combines the effects of both electrical stimulation and voluntary movement. This figure was adapted from [19].HTS: hybrid training system.
HTS protocol
The stimulation waveform used a carrier frequency of 5,000 Hz, with a frequency of 40 Hz (2.4 ms on, 22.6 ms off), a pulse width of 200 μs, and a biphasic rectangular waveform. The electrical stimulation intensity was set at 80% of the maximum tolerable voltage, a level that previous studies have shown to be effective for improving muscle strength and mass while ensuring safety [18]. The electrical stimulation device used was the HTS from Panasonic Corporation (Home Appliance Development Center, Corporate Engineering Division, Appliance Company, Panasonic Corporation, Kusatsu City, Shiga, Japan). An accelerometer (EWTS9PD, Home Appliance Development Center, Corporate Engineering Division, Appliance Company, Panasonic Corporation, Kusatsu City, Shiga, Japan) was placed on the front of each leg to serve as a joint motion sensor. The motion sensor measures the hip joint angular velocity during pedaling, and the quadriceps or hamstrings are electrically stimulated in sync with the movement of the knee joint during pedaling. A pair of 5x12 cm low-impedance gel-coated silver fiber electrodes (Nihon Medix Co., Matsudo City, Chiba, Japan) were applied to the motor points of the quadriceps and hamstrings on both legs.
Blood sampling
Participants were instructed to fast and abstain from alcohol and caffeine for 12 hours before the exercise session. They were also advised to refrain from any sports activities for one week prior to the study and during the study period. To avoid circadian fluctuations in metabolism and hormone levels, the exercise interventions were conducted between 7:00 and 8:00 AM. Blood samples were drawn from the superficial veins of the forearm at two times: before exercise and immediately after exercise. Blood lactate concentration values were measured by finger prick using the Lactate Pro 2 (LT-1730, Arkray, Co., Kyoto City, Kyoto, Japan). After blood collection, the blood was centrifuged at 3000 rpm for 10 minutes, and the serum was stored at -80°C. For the analysis of BDNF, a Human Free BDNF Quantikine ELISA Kit (R&D Systems, Minneapolis, MN, USA) was used to analyze human serum samples.
Statistical analysis
Changes before and after each exercise (HERG and CERG) were compared using the Wilcoxon signed-rank test. The changes after each exercise were compared using a linear mixed model based on a 2x2 crossover design. In this study, individuals with a BMI of 25 or higher (considered overweight by WHO standards) were defined as obese according to Japanese standards. Additionally, the prevalence of metabolic syndrome significantly increases in overweight men with a BMI of 25 or higher [23]. The analyzed data were presented as mean±standard deviation. Since this was a preliminary study, a sample size was not set. Therefore, as an exploratory study, the effect size (Cohen’s d) and statistical power regarding BDNF, the primary outcome, were calculated based on the results of this study. All statistical analyses were performed by JMP Version 16.0 statistical software (SAS Institute Inc., Cary, NC, USA), and values of p<0.05 were considered to be statistically significant.
Results
Fifteen participants were initially enrolled in the study, but one withdrew due to illness just after the baseline assessment. Fourteen participants (age 29.1±6.6 years; height 170.0±6.2 cm; body mass 68.6±9.1 kg, BMI 23.6±2.7) completed the entire study. The characteristics of the participants are shown in Table 1. Of 14 individuals, six had a BMI of 25 or higher, classifying them as obese. No adverse events due to the intervention were observed.
Serum BDNF levels significantly increased after CERG from 26419.6±5161.9 ng/ml to 28340.8±8273.9 ng/ml (p=0.0259) (Figure 3). Similarly, serum BDNF levels significantly increased after HERG from 24294.9±5313.7 ng/ml to 29795.9±7519.9 ng/ml (p=0.0017) (Figure 3). The effect sizes (Cohen's d) for CERG and HERG were 0.28 and 0.85, respectively. The statistical power for HERG was 0.84.
Changes of BDNF after HERG and CERG.BDNF, brain-derived neurotrophic factor; HERG, conventional cycle ergometer with HTS; CERG, cycling ergometer alone; HTS, hybrid training system.p-value is analyzed using a Wilcoxon signed-rank test.#p<0.05, ##p<0.01.
The results of a linear mixed model showed that the type of exercise and the presence of overweight were significant factors associated with the change in BDNF levels after exercise. In obese individuals with a BMI of 25 or higher, the change in BDNF levels after HERG was significantly greater than after CERG [ΔBDNF: 5501.0±7965.8 ng/ml, 1921.3±5308.2 ng/ml, respectively; p=0.0339] (Table 2). A significant increase in lactate levels was observed after CERG from 1.45±0.46 mmol/l to 2.16±1.31 mmol/l (p=0.0381). A significant increase in lactate levels was observed after HERG from 1.39±0.52 mmol/l to 2.22±1.17 mmol/l (p=0.0093). However, in overweight individuals (obesity) with a BMI of 25 or higher, there was no significant difference in the change in lactate levels after exercise between HERG and CERG (p=0.8632) (Table 2).
Discussion
We investigated the effects of a combined exercise method involving ergometer and NMES (HTS) on post-exercise serum BDNF levels. Regardless of the presence of NMES, serum BDNF levels significantly increased after ergometer exercise at the AT level. Additionally, in individuals with overweight (BMI ≥ 25), despite exercising at the same intensity, the ergometer combined with NMES (HERG) significantly increased post-exercise serum BDNF levels more than the conventional ergometer (CERG). For individuals with overweight, combining NMES with ergometer exercise might be a more effective and accessible exercise method compared to conventional ergometer exercise.
The magnitude of the change in BDNF after exercise is related to the exercise intensity [15]. In this study, it is believed that exercise intensity influenced the change in BDNF after exercise. The target heart rates during exercise for both the HERG and CERG groups were comparable, and there was no difference in the change in lactate levels after exercise, suggesting that the aerobic exercise intensity was equivalent. HERG may have imposed a higher exercise load than the conventional ergometer (CERG). HTS allows for the simultaneous performance of resistance exercise using electrical stimulation during aerobic exercise [18]. HTS during aerobic exercise not only provides the benefits of aerobic exercise but also promotes muscle strength and hypertrophy [19]. Changes in BDNF after exercise are observed not only following aerobic exercise but also after resistance exercise. However, resistance training aimed at muscle hypertrophy to the point of fatigue has been shown to be particularly effective [24]. Therefore, the localized resistance exercise load from HTS may have contributed to the greater increase in BDNF after HERG. Additionally, the increase in BDNF after exercise has been shown to be more effective with interval training than with continuous exercise [25]. The electrical stimulation during HERG is intermittent because the flexors and extensors are alternately electrically stimulated in response to voluntary flexion and extension movements, making it a form of interval training that utilizes electrical stimulation. These factors, such as the mechanical intensity and the interval training characteristics, may have contributed to the greater increase in BDNF after HERG. Thus, combining aerobic exercise with NMES simultaneously (HTS) is believed to effectively stimulate BDNF secretion by increasing the exercise load (mechanical load) even at the same exercise intensity (oxygen uptake). Additionally, although HERG provides the same overall aerobic exercise intensity as CERG, the pedal load is lower due to the HTS, making it easier for individuals with lower fitness levels, including those who are overweight, to pedal comfortably.
NMES has been shown to increase BDNF levels comparable to those observed after moderate-intensity aerobic exercise [26]. On the other hand, Kimura et al. reported that NMES (1.41 METs) significantly increased BDNF levels compared to quadriceps isometric resistance exercise [27]. These reports suggest that NMES appears to increase BDNF levels even at lower intensities compared to typical aerobic or resistance exercises. Furthermore, the impact of electrical eccentric muscle contractions during HERG should also be considered. Responses from satellite cells, which are involved in muscle hypertrophy, have been observed after eccentric exercise [28], and it has been shown that these responses are associated with changes in BDNF after eccentric exercise [29]. Additionally, eccentric muscle contractions are useful for improving body composition, physical function, and metabolic health in patients with type 2 diabetes and obesity due to their ability to produce high muscle tension with lower energy expenditure [30]. Therefore, the significance of electrical eccentric muscle contractions was likely greater for obese patients compared to non-obese individuals and effective in stimulating post-exercise BDNF secretion even though the exercise intensity is relatively low. However, the results of this study do not clarify the mechanism. Furthermore, fundamental research is needed to verify the mechanisms underlying the effects on metabolic function mediated by changes in BDNF. Additionally, long-term intervention studies are necessary to demonstrate the sustained effects of this exercise.
Limitations
The effect size (0.85) and statistical power (0.84) of the HERG intervention were favorable, and its effectiveness considering BMI was demonstrated statistically. However, there were only six participants with a BMI of 25 or higher, which was not a large number. Further studies, including a higher proportion of overweight (obesity) individuals with a BMI of 25 or higher, are needed. Since BDNF is influenced by cognitive function, physical function, and muscle mass, it is also important to investigate its effects in older adults. Additionally, BDNF has been reported to be associated with heart failure, dementia, Parkinson's disease, and depression. Therefore, it is necessary to consider not only BMI but also those factors. Additionally, in this study, obesity was defined as a BMI of 25 or higher for Japanese. However, the WHO defines obesity as a BMI of 30 or higher, so it is necessary to investigate cases with a higher BMI. Furthermore, since the subjects of this study are all male and young, future research is needed involving females and a broader age range. It is also necessary to adjust for habitual nutrition intake and physical activity levels, which are believed to influence BDNF levels after exercise. While this study was conducted on healthy individuals, it will be necessary to verify the effects of HERG on patients with various conditions in the future. Moreover, in this study, BDNF was measured only at one time point immediately after exercise, so the timing of peak values and the sustained increase in BDNF remain unknown. Future studies should repeatedly measure BDNF over a period of time after exercise. Of course, long-term intervention studies are also necessary to verify the long-term effects of HERG.
Conclusions
In individuals who are overweight, the combination of ergometer exercise and HTS increased post-exercise serum BDNF levels more than ergometer exercise alone. Combining ergometer exercise with NMES may be a beneficial form of exercise for individuals who are overweight.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Comparison of treadmill and cycle ergometer exercise during cardiac rehabilitation: a meta-analysis Arch Phys Med Rehabil Gerlach S Mermier C Kravitz L Degnan J Dalleck L Zuhl M 69069910120203173889310.1016/j.apmr.2019.10.184 · doi ↗ · pubmed ↗
- 2Cycle training induces muscle hypertrophy and strength gain: strategies and mechanisms Acta Physiol Hung Ozaki H Loenneke JP Thiebaud RS Abe T 12210220152580438610.1556/A Physiol.102.2015.1.1 · doi ↗ · pubmed ↗
- 3Effect of all-extremity high-intensity interval training vs. moderate-intensity continuous training on aerobic fitness in middle-aged and older adults with type 2 diabetes: a randomized controlled trial Exp Gerontol Hwang CL Lim J Yoo JK 465311620193057671610.1016/j.exger.2018.12.013PMC 6404965 · doi ↗ · pubmed ↗
- 4Physical activity in metabolic syndrome Front Physiol Chomiuk T Niezgoda N Mamcarz A ŚliżD 13657611520243844034910.3389/fphys.2024.1365761 PMC 10910017 · doi ↗ · pubmed ↗
- 5Health benefits of cycle ergometer training for older adults over 70: a review Eur Rev Aging Phys Act Bouaziz W Schmitt E Kaltenbach G Geny B Vogel T 81220152686587210.1186/s 11556-015-0152-9PMC 4748329 · doi ↗ · pubmed ↗
- 6Effects of different exercise modalities and intensities on body composition in overweight and obese children and adolescents: a systematic review and network meta-analysis Front Physiol Huang Z Li J Liu Y Zhou Y 11932231420233749743510.3389/fphys.2023.1193223 PMC 10366610 · doi ↗ · pubmed ↗
- 7The effect of physical activity on the brain derived neurotrophic factor: from animal to human studies J Physiol Pharmacol Zoladz JA Pilc A 53354161201021081796 · pubmed ↗
- 8Brain derived neutrophic factor, a link of aerobic metabolism to neuroplasticity J Physiol Pharmacol De Assis GG Gasanov EV de Sousa MBC Kozacz A Murawska-Cialowicz E 69201810.26402/jpp.2018.3.1230342429 · doi ↗ · pubmed ↗