Gastric Epithelioid Mesenchymal Tumor with the EWSR1::CREM Fusion Gene: A Case Report
Nao Yoshizawa, Hirokazu Yamaguchi, Taichiro Yoshimoto, Koji Uraushihara, Akihiko Yoshida

TL;DR
A rare gastric tumor with an EWSR1::CREM fusion gene was identified in a 58-year-old man, highlighting the need for careful follow-up due to potential malignancy.
Contribution
This case report adds to the understanding of rare gastric mesenchymal tumors with EWSR1::CREM fusion genes.
Findings
The tumor was composed of keratin-positive epithelioid cells and had an EWSR1::CREM fusion gene.
Despite initial benign appearance, the tumor's malignant potential necessitates cautious clinical follow-up.
The diagnosis was confirmed through pathology and molecular testing.
Abstract
In recent years, new molecularly defined tumor groups have been reported among tumors previously considered unclassifiable. Among them, gene fusions involving the CREB family of transcription factors, including cAMP-responsive element modulator (CREM), with genes encoding FET family RNA-binding proteins, such as Ewing sarcoma breakpoint region 1 (EWSR1), have recently been shown to be implicated in driving the pathogenesis of various tumor types. Here, we report our experience with a gastric mesenchymal tumor with epithelioid histology and an EWSR1::CREM fusion, which is rare but requires caution. A 58-year-old man with epigastric pain underwent esophagogastroduodenoscopy, which revealed a submucosal tumor, 40 × 30 mm in size, at the greater curvature of the upper gastric body. Surgical resection was scheduled because of easy bleeding from the tumor and because biopsy could not…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
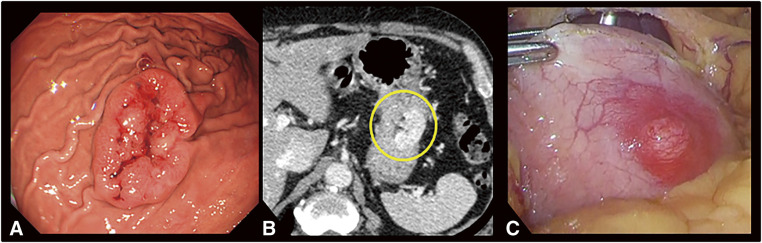 Fig. 1
Fig. 1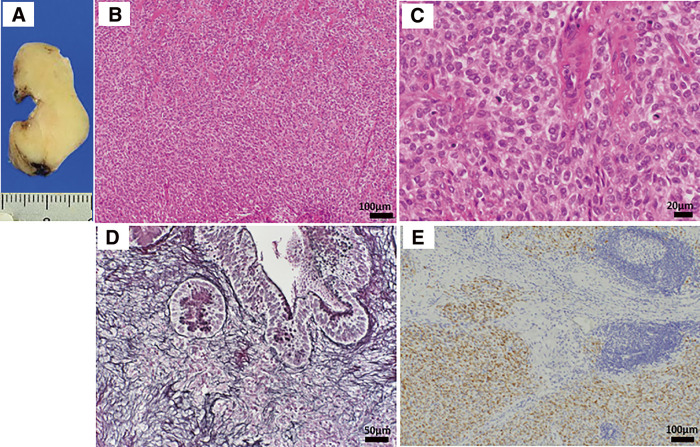 Fig. 2
Fig. 2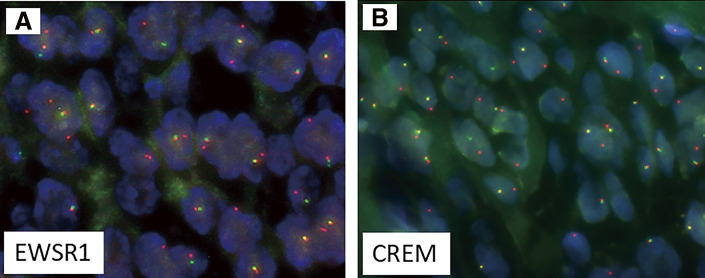 Fig. 3
Fig. 3| Case | Age | Sex | Primary site | Size (cm) | Metastasis | IHC-positive Epithelial markers | Fusion | Outcome (mo) | References | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 25 | M | Intra-abdominal continuing from fornix of the stomach | 7 | + | Liver | EMA |
| Rec (12) AWD (12) |
|
| 2 | 32 | M | Stomach | 3 | + | Liver Peritoneum Lung Spleen | AE1/AE3 |
| Rec (48, 56) AWD (122) |
|
| 3 | 64 | F | Stomach | 8 | − |
| NED (28) |
| ||
| Our case | 58 | M | Stomach | 4.5 | − | AE1/AE3 |
| NED (20) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberous Sclerosis Complex Research · Tumors and Oncological Cases · Gastrointestinal Tumor Research and Treatment
Abbreviations
AFH angiomatoid fibrous histiocytoma CCS clear cell sarcoma CCSLGT clear cell sarcoma-like tumors of the gastrointestinal tract CREM cAMP-responsive element modulator EWSR1 Ewing sarcoma breakpoint region 1 EWSR1/FUS::CREB fusion EWSR1 or FUS and CREB family fusion FISH fluorescence in situ hybridization FUS fused in sarcoma GNET gastrointestinal neuroectodermal tumor LECS laparoscopic and endoscopic cooperative surgery
INTRODUCTION
In recent years, the increasing use of genetic testing in routine surgical pathology practice has led to the discovery of fusion-associated neoplasms, and new molecularly defined tumor groups have been reported among tumors previously considered unclassifiable. Neoplasms with fusions between Ewing sarcoma breakpoint region 1 (EWSR1) or fused in sarcoma (FUS) genes and genes encoding the CREB family of transcription factors (ATF1, CREB1, and cAMP-responsive element modulator [CREM]) are one such tumor type. These fusions have been reported to drive the pathogenesis of various tumor types with mesenchymal, neuroectodermal, and epithelial lineages.^1)^
Most tumors in the gastrointestinal tract with EWSR1/FUS and CREB family fusions (EWSR1/FUS::CREB fusion) are reportedly clear cell sarcoma-like tumors of the gastrointestinal tract (CCSLGT).^2,3)^ Here, we report our experience with a gastric epithelioid mesenchymal tumor with an EWSR1::CREM fusion that was distinct from established entities.
CASE PRESENTATION
A 58-year-old man with a history of occasional epigastric pain for approximately 6 months underwent a medical checkup at a local hospital. Stomach fluoroscopy revealed a tumor located at the greater curvature of the upper gastric body, for which he was referred to our hospital.
Esophagogastroduodenoscopy showed a tumor 40 × 30 mm in size, with easy bleeding, an uneven shape, and a deep depression in the center (Fig. 1A). Since the entire tumor surface, including the depression, was covered by noncancerous epithelium, it was diagnosed as a gastric submucosal tumor. Hematoxylin–eosin staining of biopsy specimens showed a spindle cell tumor. However, no definitive diagnosis could be made despite using various types of immunostains. Endoscopic ultrasonography showed a uniform isoechoic mass that appeared to be derived from the fourth layer (i.e., the muscularis propria). A contrast computed tomography scan revealed a contrast-enhanced mass in the upper part of the stomach body (Fig. 1B), with neither invasion of the peripheral organs nor distant metastases. Positron emission tomography showed only mild accumulation in the gastric tumor, with no accumulation in other areas.
(A) Endoscopic findings. A protruding lesion measuring 40 × 30 mm, which had an uneven surface and bled easily, was observed along the greater curvature of the upper part of the stomach body. (B) CT findings. A contrast-enhanced mass (yellow circle) was observed in the upper part of the stomach body. (C) Laparoscopic findings. The serous surface of the tumor was smooth but appeared hyperemic.CT, computed tomography
Based on these results, we considered the possibility of malignancy to be low, but since the tumor bled very easily and could not be definitively diagnosed by biopsy, we decided to perform local gastric resection. Laparoscopic evaluation showed that the serous surface of the tumor was smooth but appeared hyperemic (Fig. 1C). The technique of laparoscopic and endoscopic cooperative surgery (LECS) was used to perform local gastrectomy. Due to the relatively large size of the tumor, the procedure was performed using inverted LECS with Crown methods,^4)^ which were designed to prevent the outflow of gastric contents. After excising the lesion, the open ends of the stomach wound were aligned and closed with a linear stapler. The surgical time was 182 min, and estimated blood loss was below measurable levels. The patient’s postoperative course was uneventful, and he was discharged 7 days after surgery. Currently, 1 and a half years after surgery, he remains alive without recurrence.
Pathological evaluation of the specimen showed that the tumor, measuring 4.5 × 2.7 × 1.6 cm, was slightly shiny and yellowish-white in color (Fig. 2A). Histopathological assessment revealed relatively homogeneous epithelioid cells extending from the mucosal lamina propria to the muscularis propria and slightly to the subserosal layer, with the cells proliferating in sheets with intervening hyalinized stroma (Fig. 2B). Scattered lymphoid follicles were observed at the periphery of the tumor. The tumor cells had relatively uniform nuclei with a round to oval shape and scant eosinophilic cytoplasm (Fig. 2C). The mitotic count was 3/10 high-power fields, and the cell boundaries were indistinct (Fig. 2C). Silver impregnation staining showed the presence of argyrophil fibers between the tumor cells, suggesting that it was a mesenchymal tumor (Fig. 2D). The surgical margin was negative.
(A) Cut surface of the tumor. The tumor consisted of a solid lesion that was shiny and yellowish-white in color. (B) H&E staining with ×10 magnification showed relatively uniform epithelioid cells with sheet-like proliferation and intervening hyalinized eosinophilic stroma. (C) H&E staining (×40 magnification). The tumor cells had a relatively uniform round-to-oval nucleus and scant eosinophilic cytoplasm. (D) Silver impregnation staining (×20 magnification). Argyrophil fibers were present between the tumor cells. (E) Immunohistochemical findings (×10 magnification). AE1/AE3 was partially weakly positive. Lymphoid follicles were observed at the periphery of the tumor.H&E, hematoxylin–eosin
The tumor cells were immunohistochemically positive for D2-40 (diffuse), α-smooth muscle actin (diffuse), Bcl-2 (diffuse), AE1/AE3 (focal) (Fig. 2E), and Kit (focal), and negative for DOG1, desmin, S100, CD34, EMA, β-catenin, ALK, CD21, LCA, and CD68. The Ki-67 proliferation index was approximately 7%. Fluorescence in situ hybridization (FISH) assays showed negative evidence of SS18 rearrangement. Gastrointestinal stromal tumor, solitary fibrous tumor, smooth muscle tumor, desmoid fibromatosis, inflammatory myofibroblastic tumor, follicular dendritic cell sarcoma, and synovial sarcoma were included in the differential diagnosis, but the findings were not typical for any of these diseases. Subsequently, at a pathology consultation, the tumor was found to be negative for MUC4 and SSX (C-term), while FISH analysis detected rearrangements for both EWSR1 and CREM genes (Fig. 3). Based on these findings, the tumor was diagnosed as an epithelioid mesenchymal tumor with EWSR1::CREM gene fusion.
EWSR1::CREM fusion was identified using FISH. The tumor showed EWSR1 (A) and CREM (B) rearrangements. The isolated orange signals indicate gene rearrangements.CREM, cAMP-responsive element modulator; EWSR1, Ewing sarcoma breakpoint region 1; FISH, fluorescence in situ hybridization
DISCUSSION
EWSR1::CREM fusion is one of the fusions between EWSR1 or FUS and the CREB family of genes that have been reported in various tumor entities since approximately 2017.^5)^ Types of tumors with these fusions include angiomatoid fibrous histiocytoma (AFH), soft tissue and gastrointestinal clear cell sarcoma (CCS), primary pulmonary myxoid sarcoma, hyalinizing clear cell carcinoma of the salivary gland, and malignant mesotheliomas.^1)^ EWSR1, along with FUS, belongs to the FET family of RNA-binding proteins.^6)^ EWSR1 is involved in the crucial regulation of proper centromere function and inheritance in interphase cells.^7)^ Meanwhile, CREM, together with ATF1 and CREB1, belongs to the group of transcription factors called CREB family transcription factors.^1,2)^ Among these transcription factors, CREM is a newly recognized member in human tumors, and the phenotypic spectrum associated with CREM fusion is still being clarified.^2)^
Most gastric tumors with EWSR1/FUS::CREB fusions have been reported to be CCSLGT, also known as gastrointestinal neuroectodermal tumors (GNETs). The tumor in our patient had histological findings distinct from GNETs but was similar to 3 previously reported tumors,^1,8,9)^ which are summarized in Table 1. The 4 patients, including the present case, ranged in age from 25 to 64 years and consisted of 3 men and 1 woman. Although interpreted as mesenchymal tumors, cytokeratin or EMA positivity was observed in 3 of the cases, including our patient. In case 3, which showed a mixture of epithelial and mesenchymal components in gastritis cystica profunda, the disease course was benign, while the other 2 patients experienced metastasis and recurrence. Among these 2 cases, liver metastasis occurred 1 year after diagnosis in the first case, although the patient was subsequently lost to follow-up. The second case underwent resection of the initial gastric lesion and a recurrent lesion, followed by treatment with imatinib, sunitinib, and radiation therapy for the recurrence.
In a broader context, similar epithelioid mesenchymal tumors with keratin expression and EWSR1/FUS::CREB fusion have been reported in the abdominal cavity outside the stomach, with many of these tumors showing malignant behavior, including recurrence, metastasis, and resistance to chemotherapy.^1,8)^ Considering these previous tumor reports, we believe that our case should be carefully followed up for potential malignancy. There are still very few reports of gastric epithelioid mesenchymal tumors with EWSR1/FUS::CREB fusion that do not fit the criteria for GNETs, and the collection of additional cases is needed to better understand their epidemiology, symptoms, prognosis, and treatment.
CONCLUSION
We experienced a case of gastric epithelioid mesenchymal tumor with EWSR1::CREM fusion genes that did not fit the diagnostic criteria of established tumor entities. Since a malignant course has been previously reported in the literature for similar tumors, careful follow-up is required for these cases.
ACKNOWLEDGMENTS
The authors thank FORTE Science Communications (https://www.forte-science.co.jp/) for English language editing.
DECLARATIONS
Funding
This study received no specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Authors’contributions
NY drafted the manuscript.
All other authors critically reviewed the manuscript.
NY, HY, and KU performed operations.
KU performed endoscopy and was responsible for preoperative diagnosis.
TY and AY carried out pathological diagnosis.
All authors approved the final manuscript and agreed to take responsibility for all aspects of the study.
Availability of data and materials
Data presented in this case report are available from the corresponding author upon reasonable request.
Ethics approval and consent to participate
This work does not require ethical considerations or approval.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
Competing interests
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Argani P Harvey I Nielsen GP EWSR 1/FUS-CREB fusions define a distinctive malignant epithelioid neoplasm with predilection for mesothelial-lined cavities. Mod Pathol 2020; 33: 2233–43.32770123 10.1038/s 41379-020-0646-5PMC 7584759 · doi ↗ · pubmed ↗
- 2Yoshida A Wakai S Ryo E Expanding the phenotypic spectrum of mesenchymal tumors harboring the EWSR 1-CREM fusion. Am J Surg Pathol 2019; 43: 1622–30.31305268 10.1097/PAS.0000000000001331 · doi ↗ · pubmed ↗
- 3Segawa K Sugita S Aoyama T Detection of specific gene rearrangements by fluorescence in situ hybridization in 16 cases of clear cell sarcoma of soft tissue and 6 cases of clear cell sarcoma-like gastrointestinal tumor. Diagn Pathol 2018; 13: 73.30219084 10.1186/s 13000-018-0752-6PMC 6138919 · doi ↗ · pubmed ↗
- 4Nunobe S Hiki N Gotoda T Successful application of laparoscopic and endoscopic cooperative surgery (LECS) for a lateral-spreading mucosal gastric cancer. Gastric Cancer 2012; 15: 338–42.22350555 10.1007/s 10120-012-0146-5 · doi ↗ · pubmed ↗
- 5Kao YC Sung YS Zhang L EWSR 1 fusions with CREB family transcription factors define a novel myxoid mesenchymal tumor with predilection for intracranial location. Am J Surg Pathol 2017; 41: 482–90.28009602 10.1097/PAS.0000000000000788 PMC 5350023 · doi ↗ · pubmed ↗
- 6Flucke U van Noesel MM Siozopoulou V EWSR 1—the most common rearranged gene in soft tissue lesions, which also occurs in different bone lesions: an updated review. Diagnostics (Basel) 2021; 11: 1093.34203801 10.3390/diagnostics 11061093 PMC 8232650 · doi ↗ · pubmed ↗
- 7Kitagawa R Niikura Y Becker A EWSR 1 maintains centromere identity. Cell Rep 2023; 42: 112568.37243594 10.1016/j.celrep.2023.112568 PMC 10758295 · doi ↗ · pubmed ↗
- 8Shibayama T Shimoi T Mori T Cytokeratin-positive malignant tumor in the abdomen with EWSR 1/FUS-CREB fusion: a clinicopathologic study of 8 cases. Am J Surg Pathol 2022; 46: 134–46.34049318 10.1097/PAS.0000000000001742 · doi ↗ · pubmed ↗