Partial sacrectomy with en bloc tumor resection without instrumentation. What level is safe?
Jan Štulík, Michaela Rybárová, Pavel Hladík, Robert Lischke, Zdeněk Klézl, Radek Kaiser, Ondřej Naňka

TL;DR
This paper investigates the safety of performing partial sacrectomy without surgical instrumentation, finding that it can be stable in most patients, especially those with lower activity levels.
Contribution
The study demonstrates that non-instrumented high en bloc sacrectomy can provide sufficient stability for proton therapy in selected cases.
Findings
Non-instrumented high en bloc sacrectomy can retain the cranial sacrum and allow for proton therapy.
Instrumentation is mainly needed for younger, more active patients.
Lower bone mineral density does not always require instrumentation for stability.
Abstract
En bloc sacrectomy is an extensive surgical procedure which is often the only option which provides cure. Our experience shows that, in selected cases, instrumentation is not necessary even in case of a high en bloc sacrectomy retaining the cranial part of the sacrum in situ. This creates suitable conditions for subsequent proton therapy. What level of resection is safe without reconstruction? Between 2014 and 2023 we performed a total of 29 sacral resections for various etiologies. Patients following reconstruction of the lumbosacral region by internal fixator (3) and patient after hemicorporectomy (1) were excluded from the study. The study group comprised 25 patients, 15 men and 10 women with a mean age of 45.1 years (range, 1.7–72.2 years). The most frequent indication for surgery was chordoma (8), followed by MPNST (4), yolk sac tumor (2) and undifferentiated sarcoma (2). Stress…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
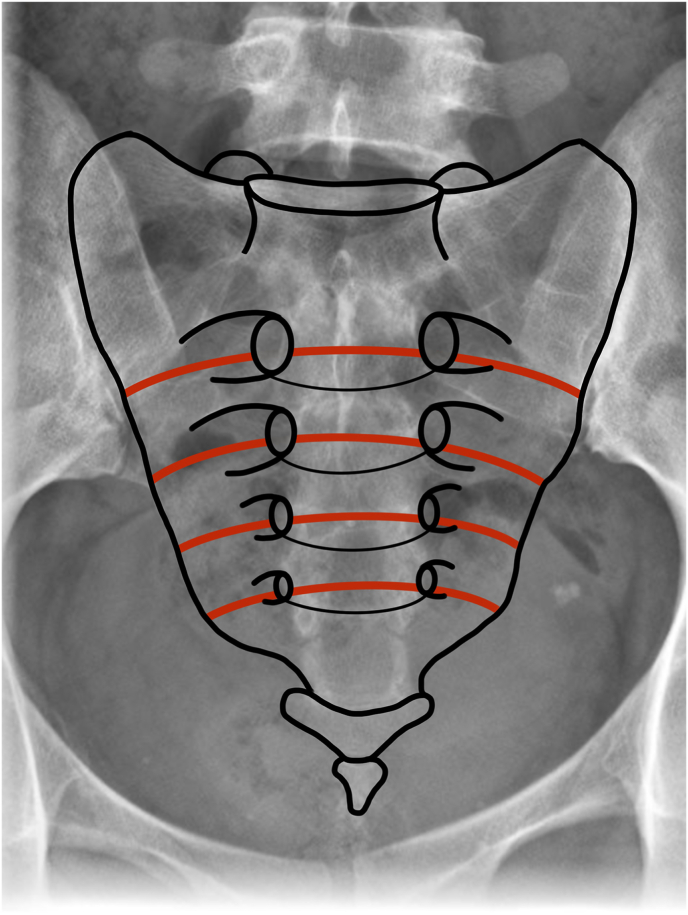 Figure 1
Figure 1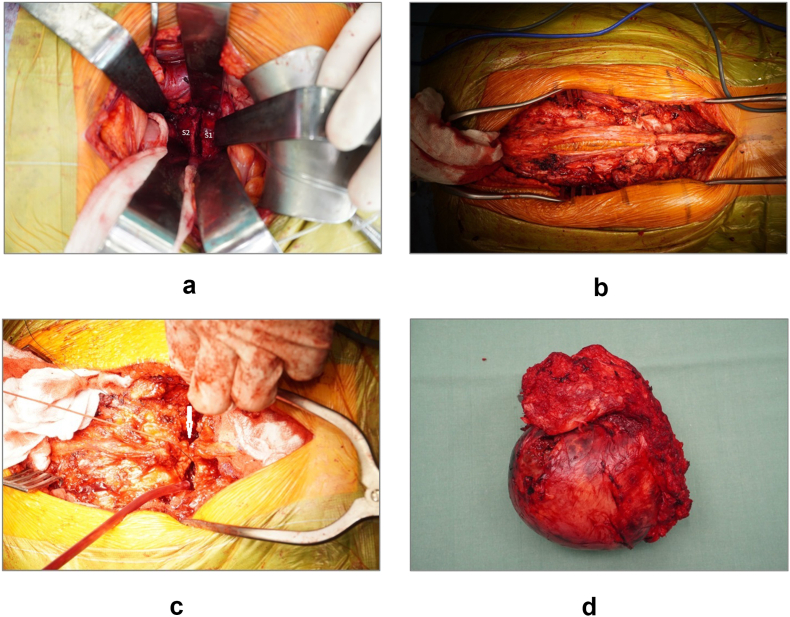 Figure 2
Figure 2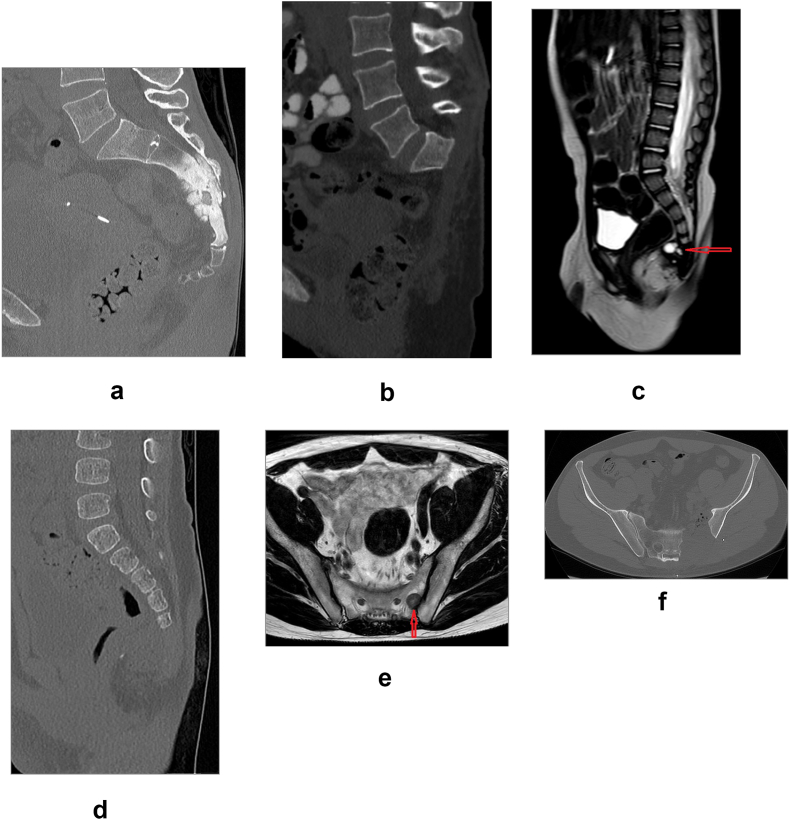 Figure 3
Figure 3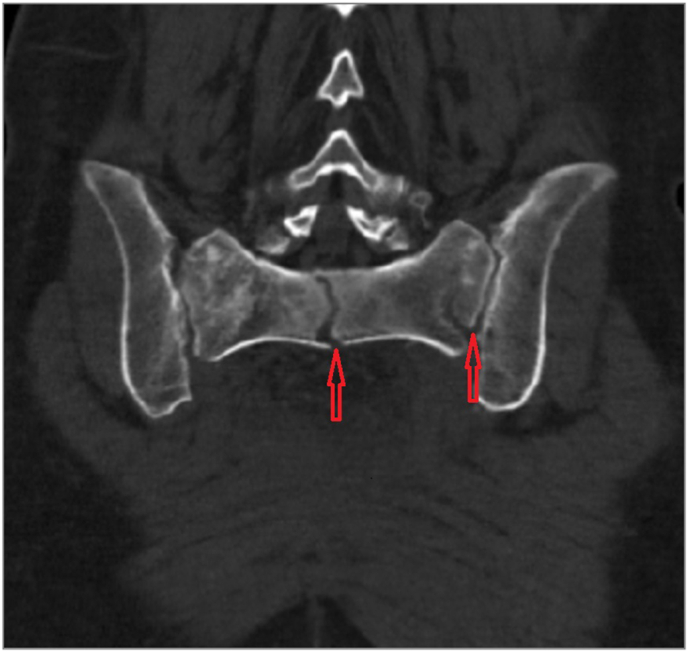 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsManagement of metastatic bone disease · Bone Tumor Diagnosis and Treatments · Spine and Intervertebral Disc Pathology
Authors’ contributions
Jan Štulík and Zdeněk Klézl contributed to the study conception and design. Michaela Rybárová; collected radiographic and clinical data. All authors contributed to the analysis and interpretation of acquired data. Jan Štulík obtained administrative and technical support necessary for successful completion of the project. Jan Štulík and Michaela Rybárová; were responsible for drafting of the first version of the manuscript. Finally, all authors read, reviewed and approved the final version of the manuscript.
Introduction
1
Sacral tumors present one of the most challenging pathologies in spinal surgery. Primary sacral tumors are rare, diagnosed mostly at an advanced stage, with a large extraosseous component. The intricate anatomy of the pre-sacral space and the neural structures inside sacrum complicate surgical treatment (Fourney et al., 2005; Guo et al., 2013; Hsieh et al., 2009; Hugate et al., 2006). En bloc sacrectomy is often the only option for patients to be cured (Feghali et al., 2021; Fourney et al., 2005). Extensive resections pose a problem of biomechanical instability of the pelvic ring and transmission of forces from the body to the lower extremities. Functional impairment after resection of neural structures significantly affects the postoperative condition. Achieving continuity between the spine and the pelvic ring and prevention of instability is the goal of reconstruction techniques, often with the use of internal fixators, mesh cages, 3D printed anatomical implants, or their combination (Morales-Codina and Martín-Benlloch, 2022; Murakami et al., 2002; Wei et al., 2019; Yu et al., 2010). In contrast, instrumentation may not be necessary in cases of a high en bloc partial sacrectomy retaining the cranial part of the sacrum in situ, in order to create suitable field for subsequent proton therapy. However, the question is whether the retained part of the sacrum can provide adequate stability in the future. The aim of the study was to evaluate the pelvic ring stability after partial en bloc resection of the sacrum and determine a safe level of resection not requiring instrumentation.
Methods
5
Patients
5.1
Between 2014 and 2023 we performed a total of 29 sacral resections for various pathologies. Patients following reconstruction of the lumbosacral region by internal fixator (3) and patients after hemicorporectomy (1) were excluded from the study. Only patients with en bloc partial sacral resection without instrumentation were included. The study protocol was approved by the ethical committee of our hospital. All patients provided written consent to be enrolled in the study and allowed publication of data. All patients were evaluated in terms of surgical parameters, oncological parameters, clinical and functional results, radiological results including bone quality, and complications of surgical and oncological treatment. The study group comprised 25 patients, 15 men and 10 women with a mean age of 45.1 years (range, 1.7–72.2 years). The most frequent indication for surgery was chordoma in 8 cases, followed by malignant peripheral nerve sheath tumor – MPNST (4), yolk sac tumor (2) and undifferentiated sarcoma (2). The main clinical symptoms included coccygodynia radiating into the buttocks and lower extremities, radiculopathy similar as in lumbar disc herniation, urinating or defecating difficulties, or non-specific sensation of pressure in the region of the small pelvis.
Preoperative protocol
5.2
All patients underwent complete preoperative testing, including radiographic, CT, MRI and angiographic examinations. Preoperatively, open biopsy was performed in 22 patients and fine-needle aspiration biopsy in 3 cases (11 patients underwent the procedure at our department and 14 patients at another institution). We did not perform preoperative embolization of the regional blood vessels. Radiological examination revealed a tumor involving S2-S5 in 14 cases, S3-S5 in 3 cases, S4-S5 in 2 cases, and unilateral involvement of S1-S2 in 6 cases. Tumor extent was evaluated according to the Enneking (Enneking et al., 1980), Weinstein-Boriani-Biagini (Boriani et al., 1997) and Fourney classifications (Fourney et al., 2005) (Table 1). Four patients received preoperative neoadjuvant chemotherapy/radiotherapy, including one patient treated at our department and three patients referred from other departments where they underwent neoadjuvant chemotherapy/radiotherapy and operation). Patients with chordoma received postoperative proton beam therapy and those with osteosarcoma adjuvant chemotherapy.Table 1**–** Summary of diagnostic, pre– and postoperative clinical data stratified by type of resection.Table 1. PtSexAgeDiagnosisEnnekingaWBBbFourneycResection levelSacrificed rootsResection marginFUP (m)Recurrence and/or meta (m)Final disease status1F51,7osteosarcomaIIBA-C/12-9midline IVS1-2 (high)S1+ (S2-5)wide117NED2F14,8MPNSTIIBA-E/1-12midline IIIS1-2 (high)S1+ (S2-5)marginal11local (9)DOD3M36,6MPNSTIIBA-C/2-8midline IIIS1-2 (high)S1+ (S2-5)wide100NED4M40,2MPNSTIBA-C/1-3midline IIIS1-2 (high)S1+ (S2-5)marginal6lung (4)DOD5F42,0HG sarcomaIIBA-E/1-12midline IIIS1-2 (high)S1+ (S2-5)marginal3widespread (1)DOD6M40,9chordomaIIBA-E/1-12midline IIIS1-2 (high)S1+ (S2-5)wide18lung (15)DOD7F63,0MF histiocytomaIIBA-C/12-5midline IVS1-2 (high)S1+ (S2-5)wide27local (24)DOD8M48,0chordomaIIBA-E/1-12midline IIIS1-2 (high)S1+ (S2-5)wide54lung (50)DOD9F59,3MPNSTIIBA-C/1-12midline IIIS1-2 (high)S1+ (S2-5)wide57NED10M72,2ccRCCIIBA-C/7-1midline IIIS1-2 (high)S1+ (S2-5)wide17widespread (14)DOD11F32,0chordomaIIBA-E/1-12midline IVS1-2 (high)S1+ (S2-5)wide39lung (30)DOD12F49,7chordomaIIAB-C/3-10midline IIIS1-2 (high)S1+ (S2-5)wide51local (33)AWD13F66,4chordomaIIBA-E/1-12midline IVS1-2 (high)S1+ (S2-5)wide21AWD14M51,5chordomaIIBA-E/1-12midline IVS1-2 (high)S1+ (S2-5)wide12AWDAverage:47,738,115M64,2chordomaIIBA-E/1-12midline IIS2-3 (middle)S2+ (S3-5)wide35local (20)AWD16M3,1yolk sacIIBA-C/2-8midline IIS2-3 (middle)S2+ (S3-5)wide9widespread (6)DOD17F71,8adenocarcinomaIBA-C/5-11midline IIS3-4 (middle)S3+ (S4-5)wide33widespread (26)DOD18M1,7yolk sacIBA-B/8-11midline IS4-5 (low)S3+ (S5)wide6NED19M57,1chordomaIIBA-C/2-6midline IS4-5 (low)S3+ (S5)wide15NEDAverage:39,619,620M37,7benign cystIIBA-C/7-1eccentric Cleft unilateralleft S3-5wide101NED21M71,8HCCIBA-C/2-5eccentric Bright unilateralright S1-2wide18widespread (14)DOD22M48,3leiomyosarcomaIBB-C/10eccentric Bleft unilateralleft S2-3wide50widespread (45)DOD23M17,6UD sarcomaIBB-C/9-11eccentric Cleft unilateralleft S2-3wide45local (33)DOD24F26,8chondrosarcomaIBA-C/2-4eccentric Bright unilateral0wide27NED25M13,0osteoid osteomaIIB/2-3eccentric Aright unilateral0wide6NEDAverage:43,042,2*Abbreviations:*AWD = alive with disease, ccRCC = clear cell renal cell carcinoma, DOD = dead of disease, HCC = hepatocellular carcinoma, HG = high grade, MF = malignant.fibrous, MPNST = malignant peripheral neural sheath tumor, NED = no evidence of disease, UD = undifferentiated, WBB = Weinstein-Boriani-Biagini.aEnneking et al., 1980bWeinstein-Boriani-Biagini 1976cFourney et al., 2005
Surgical technique
5.3
Patients in need of high-level resection (S1-S2) underwent terminal sigmoideostomy three weeks prior to the actual sacrectomy for stool derivation and maintenance of hygiene in the anal area. The operative procedure consisted of one stage anteroposterior approach or one stage posterior approach. In the first stage, the patient was in supine position, a lower midline laparotomy was performed first, for transperitoneal approach exposing internal iliac arteries on both sides, which were ligated, same as internal iliac veins. Subsequently, osteotomy was performed in the respective level, most often S1-S2 interval at the level between S1 foramen or more caudally (Fig. 1). In the next step, a silastic sheet was inserted, the peritoneum sutured, and the surgical wound closed in layers without drain. The patient was then turned to prone position. The posterior approach consisted of incision in the midline at the L4-L5 level, caudally as far as the beginning of the gluteal cleft, where it was turned to the left or right above the buttocks, depending on tumor localization. In case of open biopsy or a previous procedure, the biopsy channel/the original scar including the skin was left on the resected part. Paraspinal, parasacral and gluteal muscles were released to visualize the posterior surface of the sacrum and the coccyx, both sacroiliac joints and iliac crests. The spinal canal was accessed at the respective level according to the type of resection (most often at the L5-S1 level), the dural sac with roots were ligated (usually S2 and caudally). Subsequently, osteotomy was performed in the middle part of the sacrum depending on tumor localization (usually between S1 foramina) and widened into the anterior osteotomy. We took particular care to ensure a safe osteotomy of the lateral part of the sacrum toward the sacroiliac joint. We never use a high-speed burr during en bloc tumor resection to eliminate the risk of tissue micro-dissemination and prefer using various types of osteotomes instead. Next, osteotomy was performed of both iliac crests and sacroiliac joints were released. The surrounding ligaments and nerve roots were cut and the resected part with the tumor was removed en bloc (Fig. 2). The silastic sheet was then extracted, and paravertebral muscles were reconstructed. Neither muscle flap nor skin transfer was used. Fascia, subcutaneous tissue and skin were closed in layers and subfascial suction drain was inserted. Stabilization by an internal fixator was not used in the study group, in order to create optimal conditions for proton beam therapy. For examplesof different levels of resection see Fig. 3.Fig. 1. Schematic drawing of respective levels of performed osteotomies, most often S1-S2 interval at the level between S1 foramen or more caudally.Fig. 1. Fig. 2Peroperative photographs of a one stage anteroposterior approach. Anterior osteotomy at the level between S1 foramen (a), the biopsy channel/the original scar including the skin was left on the resected part (b), the dural sac with roots ligated (c, white arrow), the surrounding ligaments and nerve roots were cut and the resected part with the tumor was removed en bloc (d).Fig. 2. Fig. 3Examples of different levels of resection. CT reconstructions in sagittal plane of high level resection (S1-S2) for osteosarcoma in 51 + 7 female patient pre- (a) and postoperatively (b). 1 + 4 male patient with yolk sac tumor (red arrow) preoperative MRI T2-weighed sagittal image (c) and CT reconstruction in sagittal plane after low level resection (S4-S5) (d). 48 + 3 male patient with leiomyosarcoma metastasis (red arrow) in T2-weighed axial cut of MRI (e) after unilateral resection in axial cut of CT reconstruction (f).Fig. 3
Postoperative protocol
5.4
Depending on the type of neurological lesion, patients were then placed to the spinal or rehabilitation unit to practice new defecation and urination stereotypes and gait. Postoperatively, patients were mobilized with the support of crutches or a high walking frame and recommended to use them for 3 months. Postoperatively, radiographs and CT scans were performed to check the extent of resection. Biopsy was assessed for quality of margins of the resection. Regular follow-ups were performed at 6 weeks, 12 weeks, 6 months, 9 months, 12 months and then as needed, however, minimally once in 6 months, included radiographic examination; CT and MRI examination at 6 months and 12 months. After one year, follow-ups were scheduled according to the need and development of the oncological condition.
Results
3
The study group of 25 patients was divided into 3 groups: 1. high level (S1+), 2. low level (S2+ to S4+) and 3. unilateral (S1-S5). The mean follow-up was 33.3 months (range 3–117 months). The basic demographic characteristics are summarized in Table 1.
Surgical results
3.1
The first group (anterior + posterior procedure) comprised 14 patients, the mean overall operative time was 334.7 min (range 240–540min); the mean overall blood loss was 2850 ml (range 5–5400 ml) and the mean postoperative length of stay (LOS) was 37.3 days (range 8–64 days). The second group (posterior approach only with one patient having combined approach) included 5 patients, the mean operative time was 169 min (range 15–270min); the mean blood loss was 411 ml (range, 5–1100 ml) and the mean postoperative LOS was 39.4 days (range, 10–84 days). The third group (posterior procedure only) included 6 patients; the mean operative time was 165 min (range 50–360min); the mean blood loss was 1664 ml (range 50–8000 ml). The mean postoperative LOS was 15.6 days (range 6–46 days). For further details see Table 2.Table 2**–** Summary of surgical and radiological data stratified by type of resection.Table 2. PtSexAgeDiagnosisBone resection levelSurgical time A/P (min)Blood loss A/P (ml)X-ray time A/P (s)Surgical stagesLOS (d)S1 BMDa (HU)stress fr. Denispostop. complications1F51,7osteosarcomaS1-2 (high)120/200200/13002/18A + P13236zone 1 + 32F14,8MPNSTS1-2 (high)150/240100/10002/10A + P39260336,6MPNSTS1-2 (high)100/360/50300/3100/1004/10/0A + P + A162554M40,2MPNSTS1-2 (high)110/300100/18004/34A + P8243wound revision5F42,0HG sarcomaS1-2 (high)120/390200/24002/7A + P312336M40,9chordomaS1-2 (high)140/400300/32003/21A + P38207zone 3wound revision7F63,0MF histiocytomaS1-2 (high)90/210200/16003/9A + P573028M48,0chordomaS1-2 (high)150/390300/42001/5A + P162909F59,3MPNSTS1-2 (high)210/150300/20002/10A + P42186zone 310M72,2ccRCCS1-2 (high)210/200400/50001/10A + P64183zone 111F32,0chordomaS1-2 (high)120/330200/20003/2A + P60249zone 3wound revision12F49,7chordomaS1-2 (high)90/18050/16004/20A + P63354wound revision13F66,4chordomaS1-2 (high)90/150300/6001/2A + P2818714M51,5chordomaS1-2 (high)100/265200/45004/12A + P47313wound necrosisAverage:47,7128,6/243,2/50226/2450/1002,6/12,1/037,3249,915M64,2chordomaS2-3 (middle)90/180100/100010/2A + P84236ileus16M3,1yolk sacS2-3 (middle)18015010P2135217F71,8adenocarcinomaS3-4 (middle)1805005P3214418M1,7yolk sacS4-5 (low)1556P5024419M57,1chordomaS4-5 (low)20030010P10260A verage:39,690/151100/39110/6,639,4247,220M37,7benign cystleft unilateral754002P735221M71,8HCCright unilateral360800011P2519322M48,3leiomyosarcomaleft unilateral200100030P829723M17,6UD sarcomaleft unilateral200 + 1201300/5026/2P + P46/830224F26,8chondrosarcomaright unilateral15080032P627225M13,0osteoid osteomaright unilateral501008P9176Average:43,0165166415.915,6265,3Abbreviations:A = anterior approach, BMD = bone mineral density, LOS = length of stay, HU** = Hounsfield unit, P = posterior approach.^2^Denis et al., 1980aSchrieber et al., 2014
Oncological results
3.2
In the first group, a wide surgical margin was confirmed in 11 patients, marginal in 3 patients and there was no contaminated margin. In the second group, wide resection was found in all patients. In the third group, wide surgical margin was found in 4 patients, marginal in 2 patients, again, no contaminated margin was found. Local recurrence was later found in 6 cases. Patient survival times are included in Table 1, Kaplan-Meyer estimate of patient survival is shown in graph 1.
Clinical and functional outcome
3.3
We preferred to perform terminal sigmoideostomy in patients who underwent high resection (S1-S2) and in older patients with middle or low resection (S3+), which proved useful in practicing self-care after the operation and improved the standard of hygiene within the surgical wound site. All patients were placed in the spinal unit after stabilization to practice gait and self-care associated with sphincter dysfunction (fecal/urinary incontinence, or necessity of manual evacuation of stool and clean intermittent self-catheterization for the management of urinary retention). A total of 21 patients were able to walk early with crutches or in a high walking frame and gradually without any support. In the first group, plantar flexion of the foot was preserved in all patients. Five patients sustained a stress fracture of the sacral stump which, however, was clinically asymptomatic; the most serious complication was neuropathic pain. The patient's mobility was virtually unrestricted. Stability of the lumbo-sacroiliac complex was not impaired.
Radiological results
3.4
In the first group, we identified 5 fractures of the residual part of the sacrum (three in Denis zone III, one in Denis zone I and one in Denis zones I + III), see Fig. 4. The mean HU (Hounsfield unit) value of S1 body in patients with fractures was 212.2 (range, 183–249) and in patients without a fracture 263.9 (range, 187–354). In all of the cases, the values corresponded with the normal bone mineral density (Schreiber et al., 2014). In younger patients, trabecular remodeling of the residual sacrum and sclerotization of the SI joint occurred within 3 months, in elderly patients the remodeling process was slower. Bone quality in patients after a high S1+ sacrectomy was usually slightly lower in patients with a fracture of the sacral stump (S1) as compared those without a fracture (Table 2). The age of the patients did not seem to play a role – the youngest of the patients with a fracture was 32 and the oldest 72.2 years old; the youngest of the patients without a fracture was 14.8 and the oldest 71.8 years old.Fig. 455 + 7 female patient 4 years after high level resection (S1-S2) for osteosarcoma with fractures (red arrows) of the residual part of the sacrum (Denis zones I + III), CT reconstruction in a coronal plane.Fig. 4
Complications
3.5
Intraoperatively, we encountered one case of extensive bleeding from post-radiation altered veins during the anterior approach, which was addressed by ligation in cooperation with a vascular surgeon. No other intraoperative complications were observed. Early postoperative complications included wound healing problems in 6 patients, 5 required surgical revision and 1 patient underwent surgical revision of the abdominal cavity for postoperative ileus. (Table 2). In addition to the above-mentioned fractures, late complications included 2 cases of wound dehiscence after the proton beam therapy (70Gy). The therapy was in both cases difficult and protracted, the soft tissue defect failed to heal, and the patients lived with chronic fistula.
Discussion
4
Resection of sacral tumors is utilizing extensive and complex operative techniques and is associated with longer operative times, higher blood loss, surgical wound healing issues and, in general, with a higher number of various complications (Varga and Lazary, 2010). The main issues in this respect include the choice of an adequate surgical approach, assessment of stability of the lumbo-sacroiliac complex, filling the space after sacral resection, postoperative wound care and managing of functional disorders following resection of neural structures (Feghali et al., 2021; Fourney et al., 2005; Varga and Lazary, 2010).
Fourney et al. (2005) categorized sacral resections into two basic groups: midline tumors and eccentric lesions. The midline group includes low, middle and high resection, total sacrectomy and hemicorporectomy. The resection level was specified according to the nerve root sacrifice. Low resection is associated with sacrificing S4 and lower nerve roots, middle resection is at the level of S3 nerve roots and in high resection at least one S2 nerve root and both S1 roots. Total sacrectomy requires sacrifice of both S1 roots. In the case of hemicorporectomy (translumbar amputation), neural structures are ligated at the L4-L5 or L3-L4 level (Štulík et al., 2020). The lateral group includes resection of the sacroiliac joint and hemisacrectomy. Total en bloc sacrectomy and high sacrectomy are traditionally performed via the anteroposterior combined approach, the middle and low resections via the posterior approach and the lateral resections from the lateral approach (Fourney et al., 2005; Varga et al., 2014; Zhang et al., 2003). Clarke et al. (2012) recommend the use of the posterior-only approach for all sacral tumors that do not extend beyond the lumbosacral junction or invade the small pelvic organs. Zang et al. (Zhang et al., 2009) published 10 posterior-only total en bloc resections of the sacrum and consider this technique to be a suitable and safe procedure for all sacral tumors. Sherman et al. (2012) described acceptable morbidity after the posterior-only approach for sacral tumor en bloc resection and identified obesity and operative time of more than 10 h as risk factors. McLoughlin et al. (2008) reported on total en bloc sacrectomy from posterior-only approach with sacral elevation to facilitate vascular control. By contrast, Roldan et al. (2014) described a low en bloc resection of the sacrum together with a rectal tumor from the anterior-only approach. We prefer combined anteroposterior surgical approaches for total and high en bloc sacrectomies, a posterior-only approach for middle and low, as well as lateral resections, and a combined posteroanterior approach for hemicorporectomy.
En bloc resection with a margin of healthy tissue is an essential criterion of a successful operative treatment of malignant sacral tumors. Bederman, Castiglione, Feghali, Fourney, Guo, Sciubba, Varga, Wei et al. (Bederman et al., 2014; Castiglione et al., 2020; Feghali et al., 2021; Fourney et al., 2005; Guo et al., 2013; Sciubba et al., 2009; Varga et al., 2014; Wei et al., 2019) published a robot-assisted resection within the anterior procedure in combination with a standard open posterior procedure. Farshad et al. (2021) described 3D printed osteotomy guide for a precise execution of low sacral resection.
Stability of the lumbo-sacroiliac complex is decisive for indication of an instrumented reconstruction. Instrumentation is not indicated in low resections with an intact sacroiliac joint (Bederman et al., 2014; Fourney et al., 2005; Štulík et al., 2020). On the contrary, in case of total sacral resection most authors favor iliolumbar stabilization allowing early rehabilitation (Fourney et al., 2005; Hugate et al., 2006; Morales-Codina and Martín-Benlloch, 2022; Murakami et al., 2002; Varga and Lazary, 2010). Bederman et al. (2014) distinguish between three types of reconstruction techniques: spinopelvic fixation (SPF), posterior pelvic ring fixation (PPRF) and anterior spinal column fixation (ASCF) and recommend their use in combination. Another group of authors avoid any instrumentation due to the risk of infection, loosening, prolonging of operative time etc. (Roldan et al., 2014; Wei et al., 2019). Wuisman et al. (2000) reported on 5 patients after total sacrectomy without instrumentation, where a caudal shift of the lumbar spine occurred, and a mass of scar tissue developed between the spine and the pelvis which provided a certain degree of stability with a satisfactory functional result after more than 8 weeks. In high resections between S1-S2, stability of the sacroiliac joints depends on the extent of resection. The complex is considered stable with preservation of at least 50 % of the surface of sacroiliac joints. This represents preservation of at least half of the S1 segment and stabilization is not necessary (Fourney et al., 2005; Hugate et al., 2006; Varga and Lazary, 2010; Zhu et al., 2012). Hugate et al. (2006) published a biomechanical study on incidence of S1 fractures following a high sacral resection on cadaveric material. With sacrectomy performed caudal to the S1 neural foramina, the average resection of the sacroiliac joints was 16 %, with sacrectomy performed cephalad to the S1 neural foramina it was 25 %. In lower resections, axial load caused Denis zone II fractures, in higher resections more often Denis zone III fractures, but bilateral. The authors recommend reconstruction and fixation in higher resections performed cephalad to the S1 neural foramina. Bergh et al. (2000), however, reported 33 % of stress fractures in their 18 patients after high sacral resections (S1-S2 and higher). A clinically long-term negative effect of the fracture was observed only in one patient. In our cohort of 14 patients after a high en bloc sacral resection (S1-S2) without fixation, we recorded 5 (35.7 %) fractures localized solely in Denis zone I or III (Denis et al., 1988). Clinically more severe complications were not observed.
Filling the space after total or high sacral resection and the subsequent wound suture with a high risk of wound healing problems are one of the main issues of operative treatment. Most authors prefer soft tissue reconstruction to avoid rectal prolapse and wound healing complications. The most frequently performed transfer technique uses vertical rectus abdominis musculocutaneous (VRAM) flap via the anterior approach or gluteus maximus adipomuscular (GM) flap from the posterior approach (Fourney et al., 2005; Varga et al., 2014) Kim et al. (2015) recommend VRAM flap technique for complex anteroposterior surgical approaches and GM flap technique for posterior approaches. 3D printed sacral endoprosthesis with or without a supplementing lumbopelvic fixation is an up-to-date option meeting both the above-mentioned requirements, i.e., stability of the complex and filling of the defect (Morales-Codina and Martín-Benlloch, 2022; Wei et al., 2019). Wei et al. (2019) published a cohort of 10 patients with a 3D printed sacral implant and report results in terms of stability of the complex and implant failure comparable to those provided by a combined technique of fixation. They recorded significantly better results only in comparison with posterior reconstruction and fixation. Morales-Codina and Martín-Benlloch (2022) evaluated various types of iliolumbar fixation alone or in combination with a 3D printed implant in their biomechanical study. With the use of a 3D printed implant, they found a marked decrease in stress values related to instrumentation and bone structures and assumed a reduced risk of instrumentation failure. Huang et al. (2019) also pointed out biomechanical benefits of a 3D printed implant and favor its use.
Complications after sacral resections are relatively frequent. In addition to the above-mentioned fractures, they include particularly wound healing problems or local recurrencies associated with non-radical procedures. Reynolds et al. recommend soft tissue reconstruction is performed after total sacrectomy allowing tension-free closure, and dead space elimination, thus reducing wound dehiscence and return to theater (Reynolds et al., 2016).
Potential functional impairment of the patient after en bloc sacral resection is an important part of the consenting process. Zoccali et al. (2016) focused in their review on neurological deficits, i.e., residual motor function and gait, sensitivity, bladder, bowel, and sexual function. In total sacrectomies, all functions are compromised to a certain degree, residual motor function depends on sparing L5 and S1 nerve roots. Essential for bladder and bowel function is preservation of at least one L3 nerve root. Unilateral resection is usually associated with a better clinical result. Fourney et al. (2005) report more severe impairment of sexual function in older patients.
Conclusion
5
Partial sacrectomy with en bloc tumor resection is an extensive surgical procedure which is often the only option which provides cure. Our experience shows that, in selected cases, instrumentation is not necessary even in case of a high en bloc partial sacrectomy (S1-S2 level) retaining the cranial part of the sacrum in situ. This creates suitable conditions for subsequent proton beam therapy. Stress fractures of the sacral stump occur in elderly patients with lower bone mineral density, or in younger patients with a higher bone mineral density who are more active when resuming their daily routine after the operation. Instrumentation is, in our view, primarily indicated in younger and more active patients, whereas in a majority of patients, even with lower bone mineral density, non-instrumented procedure results in sufficient stability with all levels of resection.
Funding
This study was supported by Ministry of Health of Czech Republic - conceptual development of research organization, Motol University Hospital, Prague, Czech Republic (grant number: 00064203).
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bederman S.S.Shah K.N.Hassan J.M.Hoang B.H.Kiester P.D.Bhatia N.N.Surgical techniques for spinopelvic reconstruction following total sacrectomy: a systematic review Eur. Spine J.232201430531910.1007/s 00586-013-3075-z 24150036 PMC 3906440 · doi ↗ · pubmed ↗
- 2Bergh P.Kindblom L.G.Gunterberg B.Remotti F.Ryd W.Meis-Kindblom J.M.Prognostic factors in chordoma of the sacrum and mobile spine: a study of 39 patients Cancer 88920002122213410.1002/(sici)1097-0142(20000501)88:9<2122::aid-cncr 19>3.0.co;2-110813725 · doi ↗ · pubmed ↗
- 3Boriani S.Weinstein J.N.Biagini R.Primary bone tumors of the spine. Terminology and surgical staging Spine 22919971036104410.1097/00007632-199705010-000209152458 · doi ↗ · pubmed ↗
- 4Castiglione M.Conti C.Frondizi D.Cottini E.Cochetti G.Ciampini A.Cellini V.Mearini E.A combined one-staged robot-assisted sacral chordoma resection World Neurosurg 141202021021410.1016/j.wneu.2020.06.05632553601 · doi ↗ · pubmed ↗
- 5Clarke M.J.Dasenbrock H.Bydon A.Sciubba D.M.Mc Girt M.J.Hsieh P.C.Yassari R.Gokaslan Z.L.Wolinsky J.P.Posterior-only approach for en bloc sacrectomy: clinical outcomes in 36 consecutive patients Neurosurgery 712201235736410.1227/NEU.0b 013e 31825 d 01d 4; discussion 36422569060 · doi ↗ · pubmed ↗
- 6Denis F.Davis S.Comfort T.Sacral fractures: an important problem. Retrospective analysis of 236 cases Clin. Orthop. Relat. Res.227198867813338224 · pubmed ↗
- 7Enneking W.F.Spanier S.S.Goodman M.A.A system for the surgical staging of musculoskeletal sarcoma Clin. Orthop. Relat. Res.15319801061207449206 · pubmed ↗
- 8Farshad M.Selman F.Burkhard M.D.Müller D.Spirig J.M.Partial sacrectomy with patient-specific osteotomy guides N Am. Spine Soc. J.8202110009010.1016/j.xnsj.2021.100090 PMC 882005635141654 · doi ↗ · pubmed ↗