Ruptured abdominal aortic aneurysm and aortocaval fistula: a highly lethal find
Walter Mario Ángel Jaramillo, Marby Sharyne Forero Gaviria, Romario Chanci Drago, Natalia Guzmán Arango, Natalia Barrera Cuesta, Andrés Gilberto Giraldo Echeverri, Verónica Lucía Malabet Mejía, Walter Mario Ángel Jaramillo, Marby Sharyne Forero Gaviria, Romario Chanci Drago

TL;DR
This paper reports a rare and life-threatening case of a ruptured abdominal aortic aneurysm with an aortocaval fistula and highlights the challenges in treating this condition.
Contribution
The paper presents a clinical case emphasizing the rarity and high risk of aortocaval fistulas due to ruptured aneurysms.
Findings
Aortocaval fistula is a rare but highly lethal complication of abdominal aortic aneurysms.
Emergency surgical intervention is critical for managing this condition, though it remains associated with high morbidity and mortality.
Clinical manifestations vary depending on the progression of the disease.
Abstract
Within the spectrum of abdominal aortic aneurysm, various complications can arise, including the development of an arteriovenous fistula connecting this major vessel to the infrarenal inferior vena cava. This report presents the case of a 70-year-old man with sudden, intense abdominal pain and syncope, found intraoperatively to have an aortocaval fistula due to a ruptured abdominal aortic aneurysm. The patient underwent emergency care, including fistula closure and placement of a Dacron aortobifemoral graft. Aortocaval fistula is a rare complication of aortic aneurysmal disease, with clinical manifestations varying depending on disease progression, leading to high morbidity and mortality both before and after surgical or interventional treatment. Dentro del espectro de aneurisma de aorta abdominal, se presentan diversas complicaciones asociadas a esta patología, entre ellas el…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
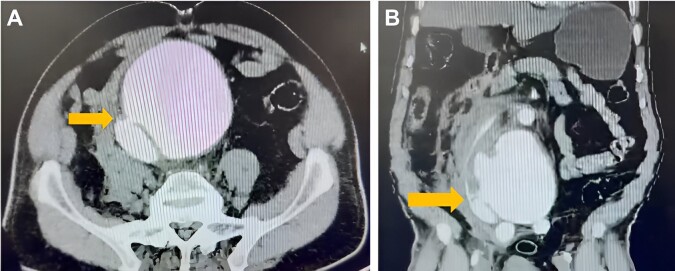 Figure 1
Figure 1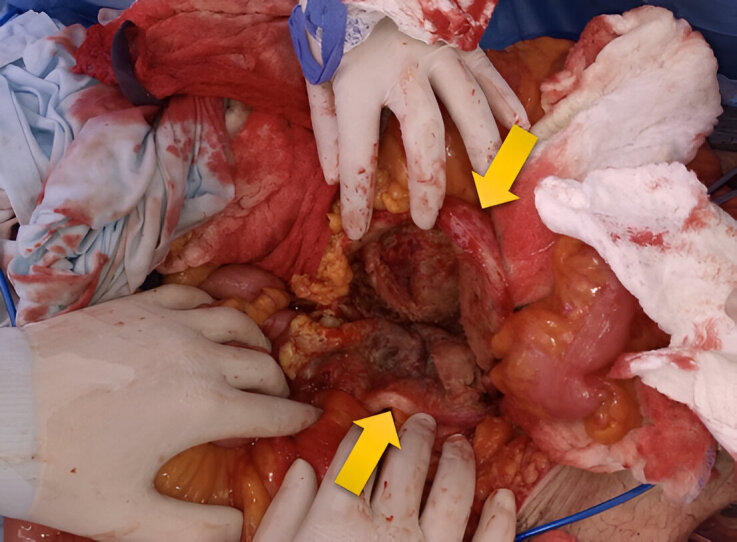 Figure 2
Figure 2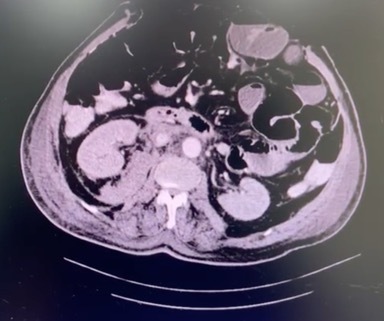 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic aneurysm repair treatments · Vascular Procedures and Complications · Cardiac, Anesthesia and Surgical Outcomes
INTRODUCTION
The aortocaval fistula (ACF) is an abdominal aortic aneurysm (AAA) complication. This condition is associated with a mortality rate ranging from 22% to 51% and is classified as primary in 80% of cases and secondary in 20%. Among primary cases, 5% to 10% originate from mycotic aneurysms or occur due to Ehlers-Danlos or Marfan syndrome.^1^ In these cases, aortic aneurysms can erode the inferior vena cava (IVC) or iliac veins, leading to an ACF.^2^ The most common ACF location is in the distal abdominal aorta, just above the iliac vein confluence. Most ACFs are asymptomatic, and their clinical presentation depends on the disease’s progression time and whether they are associated with the rupture of a preexisting abdominal aneurysm. When there is no aneurysmal rupture, clinical manifestations include a hyperdynamic hemodynamic state (tachycardia, low diastolic pressure, and cardiac dilation). Additionally, about 80% of patients experience abdominal and/or lumbosacral pain. During physical examination, most present a palpable mass, an audible continuous murmur, and a shiver.^3^ In advanced stages of ACF, the shunting of high-resistance arterial blood into the low-resistance venous system leads to congestive heart failure, commonly with venous hypertension. Additionally, it can affect the digestive and urinary systems, as well as the lower limbs, potentially causing lower gastrointestinal bleeding, hematuria, and lower limb edema.^4^ When aneurysmal rupture occurs, the clinical presentation is consistent with acute abdomen in a patient with hemodynamic instability.^5^
The ideal diagnosis should be confirmed by imaging, with contrast-enhanced abdominal computed tomography (CT) being the method of choice. Radiological findings include aneurysmal dilation of the abdominal aorta, arteriovenous shunt with contrast flow from the aorta to the IVC, and, in some cases, mural thrombus with obstructive effect at the fistula level.^6^
Current treatment strategies include open surgical repair, endovascular repair, or both.^7^ ACF endovascular repair has been increasingly described in the literature, with a variety of techniques and devices available, which are implanted within the abdominal aorta and/or the IVC.^8,9^ Open surgical repair has been the most frequently described treatment and, to date, continues to be considered the treatment of choice. Case complexity and the expertise of the healthcare center professionals are directly related to treatment strategy for this condition.^10^
This case report was approved by the ethics committee of the institution (Pablo Tobón Uribe Hospital).
PART I – CLINICAL SITUATION
The patient was a 70-year-old man, who presented a sudden onset of generalized and intense abdominal pain radiating to the lumbar region, with a syncope episode. He had a history of heavy smoking and no other comorbidities and was admitted to a nearby hospital in poor general condition, diaphoretic, and hypoperfused. During physical examination, marked abdominal distension, a pulsatile mass, and diminished femoral pulses were noted. Arterial blood gases revealed metabolic acidosis and severe hyperlactatemia. An emergency contrast-enhanced abdominal CT scan (Figure 1) was performed, and that was initially interpreted as an abdominal aortic dissection associated with a contained hematoma. Due to this finding, pharmacological control of blood pressure and heart rate were initiated, and the patient was immediately transferred to a higher-level hospital with available vascular surgery.
Abdominal computed tomography scan of the patient prior to surgical intervention: (A) axial cut showing the aortocaval arteriovenous fistula (yellow arrow); (B) coronal cut showing the aortocaval arteriovenous fistula (yellow arrow).
After clinical evaluation and image review by vascular surgery and radiology, a diagnosis of infrarenal AAA rupture was determined.
Given the diagnosis, the surgical alternatives were questioned: open repair or endovascular technique? However, due to the patient’s rapid clinical deterioration and the lack of immediate availability of trained personnel for endovascular management of the ruptured AAA, an emergency laparotomy was the procedure of choice.
PART II – WHAT WAS DONE
The patient underwent open surgery and, during the procedure, a ruptured infrarenal AAA, approximately 12 cm in diameter, was found. Proximal and distal vascular control was performed, followed by opening the aneurysmal sac (Figure 2). At this point, a 2 cm ACF was also identified, requiring proximal and distal control of the IVC. The ACF was then closed by suturing the venous wall defect with continuous polypropylene sutures. Finally, aortic reconstruction was performed with a Dacron aortofemoral graft.
Opening of the aortic aneurysm following vascular control; aortic wall (yellow arrows).
The patient left surgery with an open abdomen and was transferred to the intensive care unit to continue the resuscitation process. During the hospital stay, he progressed well, with a dynamic abdominal wall closure. As a postoperative complication, he developed a urinary tract infection, for which an antibiotic was administered. Recovery was successful, and no complications related to the surgical technique were observed. Postoperatively, a contrast-enhanced abdominal CT scan was performed to evaluate differential diagnoses due to postoperative ileus. No complications related to the surgery were reported, and no ACF was identified (Figure 3).
Abdominal computed tomography scan of the patient after surgical intervention, with absence of the aortocaval fistula.
DISCUSSION
ACFs are rare complications of AAAs, with high morbidity and mortality rates, significantly affecting multiple body systems. Early diagnosis, treatment, and correction of these fistulas pose a significant challenge.
The classic surgical treatment for ACF focuses on vascular control of the aneurysm, followed by direct closure of the arteriovenous communication from the aneurysmal sac.^11^ Treatment options include open surgery and endovascular treatment,^12,13^ which are elected based on clinical presentation, comorbidities, surgical anatomy, and patient stability in the operating room.
Open surgery remains widely used, with a high success rate, low reintervention rates, and no significant increase in postoperative mortality compared to endovascular treatment. However, it is associated with longer hospital stays and higher morbidity.^7,14^ Conversely, endovascular treatment offers an attractive therapeutic alternative to open surgery, presenting satisfactory results, such as less blood loss.^15^ However, the number of patients treated via the latest approach remains low, and long-term follow-up data are insufficient. Additionally, it presents complications such as endograft thrombosis, endoleaks, among others.^15,16^
However, endovascular repair is the preferred method for treating ACF,^17^ as it presents lower postoperative complication rates compared to open surgery.^18^ When available, endovascular repair is the method of choice,^19^ especially in multimorbid patients with favorable anatomy. Conversely, to avoid follow-up and reinterventions often required by endovascular treatment, open surgery is preferred in young, healthy patients or those with unfavorable anatomy.^20^
CONCLUSION
ACF is a very rare complication among patients with AAA. Its clinical presentation varies depending on the presence or absence of aneurysmal rupture and the disease's progression.
Proper pre-surgical imaging and interpretation are essential to avoid incorrect diagnoses and, most importantly, to provide the best treatment strategy for the patient.^16^ Although endovascular treatment is preferred today, open surgery remains a viable option.^20^
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dakis K Nana P Kouvelos G et al Treatment of aortocaval fistula secondary to abdominal aortic aneurysm: a systematic review Ann Vasc Surg 20239020421710.1016/j.avsg.2022.11.00836496094 · doi ↗ · pubmed ↗
- 2Syme J Case of spontaneous varicose aneurism Edinb Med Surg J 18313610810410530329946 PMC 5760152 · pubmed ↗
- 3Zúñiga G Ramón Rodríguez J Cáceres P Fístula aortocava como complicación de aneurisma aórtico abdominal Rev Chil Cir 201163662362610.4067/S 0718-40262011000600013 · doi ↗
- 4Akwei S Altaf N Tennant W Mac Sweeney S Braithwaite B Emergency endovascular repair of aortocaval fistula: a single center experience Vasc Endovascular Surg 201145544244610.1177/153857441140708721571773 · doi ↗ · pubmed ↗
- 5Moore WS Lawrence PF Oderich GS Fístula aortocava: cirugía vascular y endovascular.New York Elsevier 2019
- 6Dakis K Nana P Kouvelos G et al Treatment of aortocaval fistula secondary to abdominal aortic aneurysm: a systematic review Ann Vasc Surg 20239020421710.1016/j.avsg.2022.11.00836496094 · doi ↗ · pubmed ↗
- 7Umscheid T Stelter WJ Endovascular treatment of an aortic aneurysm ruptured into the inferior vena cava J Endovasc Ther 200071313510.1177/15266028000070010510772746 · doi ↗ · pubmed ↗
- 8Silveira PG Cunha JRF Lima GBB Franklin RN Bortoluzzi CT Galego GN Endovascular treatment of ruptured abdominal aortic aneurysm with aortocaval fistula based on aortic and inferior vena cava stent-graft placement Ann Vasc Surg 20142881933.e 110.1016/j.avsg.2014.06.07325017775 · doi ↗ · pubmed ↗