Malignant Hypertension Mimicking Pulmonary-Renal Syndrome
Shannon M Lee, Aida F Martinez, Nathan Yee

TL;DR
A patient with symptoms resembling a rare lung-kidney syndrome was actually suffering from severe high blood pressure, highlighting the need to consider this condition in similar cases.
Contribution
This case report highlights malignant hypertension as a rare mimic of pulmonary-renal syndrome.
Findings
The patient presented with symptoms suggesting pulmonary-renal syndrome but was ultimately diagnosed with malignant hypertension.
Malignant hypertension can cause lung and kidney damage, mimicking the signs of pulmonary-renal syndrome.
Early recognition of malignant hypertension is crucial to avoid unnecessary immunosuppressive treatment.
Abstract
Pulmonary renal syndrome (PRS) is a rare clinical syndrome characterized by pulmonary hemorrhage and rapidly progressing glomerulonephritis. It is commonly due to a rheumatologic etiology, including antineutrophil cytoplasm antibodies vasculitis or antiglomerular basement membrane disease. Given the rapid progression, patients are often empirically treated when there is high clinical suspicion for PRS. Few case reports have shown malignant hypertension (HTN) as a mimicker of PRS. We present a case of a patient with dyspnea, hemoptysis, and hematuria where there was high suspicion for PRS, and immunosuppression was initiated, but in the end, the etiology was malignant HTN. Malignant HTN can lead to multiple end-organ damage, including the lungs and kidneys; thus, it is important to consider malignant HTN in the differential. Overall, we report a case of malignant HTN mimicking PRS.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
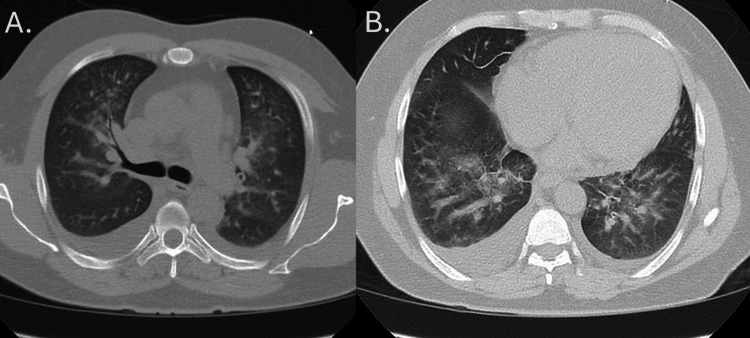 Figure 1
Figure 1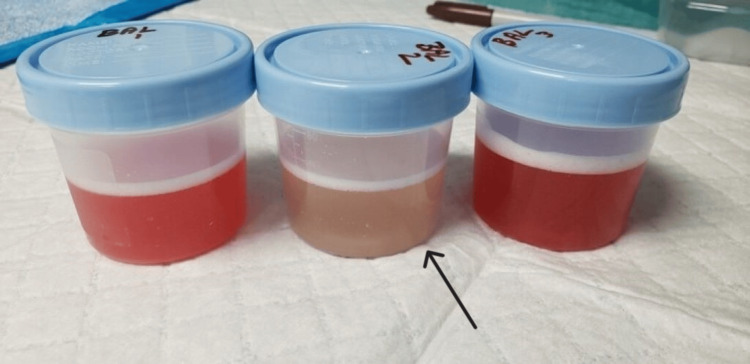 Figure 2
Figure 2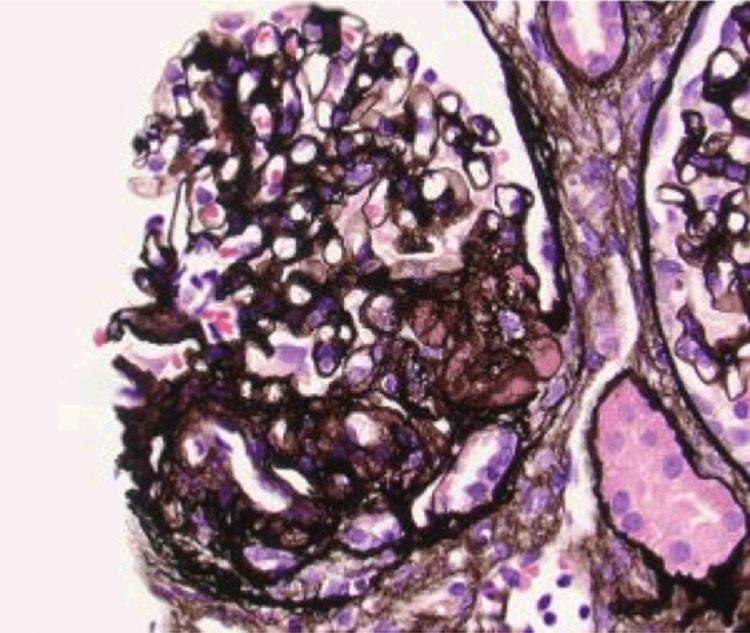 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoagulation, Bradykinin, Polyphosphates, and Angioedema · Pulmonary Hypertension Research and Treatments · Amyloidosis: Diagnosis, Treatment, Outcomes
Introduction
Pulmonary renal syndrome (PRS) is characterized by pulmonary hemorrhage and rapidly progressing glomerulonephritis, often presenting with hemoptysis, acute kidney injury (AKI), and hematuria [1,2]. PRS is most often due to autoimmune conditions, including antineutrophil cytoplasm antibody (ANCA) vasculitis, antiglomerular basement membrane (GBM) disease, and systemic lupus erythematosus [1-3]. The main pathology behind PRS is inflammation and necrosis of the capillaries. In the lungs, destruction of the pulmonary capillaries leads to vessel wall breakdown and necrosis, which can present as hemoptysis. In the kidneys, there is often necrotizing glomerulonephritis, which often presents as hematuria [4]. Given that respiratory and renal compromise may occur rapidly, prompt recognition is vital. Definitive diagnosis of PRS consists of lung biopsy with findings of small vessel vasculitis or renal biopsy with the presence of glomerulonephritis. However, this sometimes may not be feasible in the setting of acute illness [5]. While not diagnostic, bronchoalveolar lavage (BAL) is often performed to confirm diffuse alveolar hemorrhage (DAH) [5]. When suspicion is high, immunosuppressive agents and plasma exchange are initially used, even in cases when the diagnosis is not yet confirmed, as there is a risk of rapid progression [1].
This article was previously presented as a rapid-fire case report presentation at the 2024 CHEST Annual Scientific Meeting on October 7, 2024.
Case presentation
A 36-year-old man with a history of hypertension (HTN) presented with two weeks of dyspnea, non-life-threatening intermittent hemoptysis, and hematuria. He had recently stopped his blood pressure medications, which included amlodipine, hydrochlorothiazide, and valsartan, a few months before admission after moving from Central America. He had a temperature of 37.3°C, heart rate of 118 bpm, respiratory rate of 25 breaths/minute, and blood pressure of 235/177 mmHg. Laboratory analysis revealed an elevated creatinine of 3.05 mg/dL and a urinalysis (UA) notable for a large amount of blood with 26-50 red blood cells (RBCs)/high-power fields and >600 mg/dL protein. The urine protein/creatinine ratio was 4.06. His blood pressure quickly improved after receiving IV labetalol in the emergency department. Given high concern for pulmonary-renal syndrome based on presentation, a broad autoimmune workup including ANCA, antimyeloperoxidase (MPO), antiproteinase-3 (PR3), and GBM was sent out. Computerized tomography of the chest demonstrated bilateral ground glass opacities and infiltrates (Figure 1).
CT of the chest with bilateral ground glass opacities and infiltrates seen at two locations: at the level of the pulmonary arch (A) and below the pulmonary arch (B)CT: computed tomography
During his hospitalization, the patient's blood pressure management was escalated to include carvedilol and nifedipine. Rheumatology and nephrology were consulted, and due to high concern for rheumatologic etiology, pulse-dose steroids and immunosuppressive therapy were initiated. In addition, the pulmonology team evaluated the patient, and a bronchoscopy with BAL was performed in the right middle lobe, lingula, and left lower lobe. BAL fluid was bloody, but serial aliquots of BAL fluid did not consistently show an increasingly hemorrhagic return consistent with bland pulmonary hemorrhage rather than DAH (Figure 2). In addition, while hemoptysis was documented before the bronchoscopy with BAL, no hemoptysis was documented after. Infectious workups, including BAL studies, later returned negative results. Before discharge, autoimmune workup, including ANCA, MPO, PR3, and GBM, returned negative, leading to the discontinuation of pulse-dose steroids and immunosuppressive therapy. The patient was discharged with antihypertensive medications and steroid taper, as well as a plan for a renal biopsy.
BAL results showing bloody return (right and left). Subsequent aliquot (middle) does not consistently show hemorrhagic returnBAL: bronchoalveolar lavage
Two weeks after discharge, he underwent a renal biopsy, which showed thrombotic microangiopathy (TMA) with secondary focal and segmental glomerulosclerosis and acute tubular injury (Figure 3). Findings were consistent with acute injury from malignant HTN in the setting of chronic uncontrolled HTN. There was no evidence of glomerulonephritis or vasculitis. Ultimately, malignant HTN was the etiology of his hemoptysis and hematuria with AKI. Four months after discharge, he was adherent to his antihypertensive regimen and normotensive with some improvement in renal function to serum Cr 2.69 mg/dL and resolution of hematuria given trace protein seen on UA.
Renal biopsy results with JMS stain to highlight the segmental glomerulosclerosisJMS: Jones methenamine silver
Discussion
PRS consists of the combination of DAH and rapidly progressive glomerulonephritis. PRS is most commonly due to autoimmune conditions: 70% of cases are due to ANCA vasculitis, and 20% are due to anti-GBM disease [2]. The remaining 10% of cases are attributed to rheumatoid arthritis, mixed connective tissue disease, and poststreptococcal glomerulonephritis [2]. The pathological process for PRS differs based on the condition, but it is commonly due to small vessel inflammation in the pulmonary capillaries and the glomerulus. In the lungs, the inflammation in the capillaries leads to neutrophil influx, which disrupts the integrity of the capillaries, allowing for RBCs to flood into the alveoli [2]. This presents as DAH. The renal pathology consists of fibrinoid deposition and crescentic inflammation, ultimately causing glomerulonephritis, which often presents as hematuria [6].
Malignant HTN is defined as elevated blood pressure with target end-organ damage, including the brain, eyes, and kidneys. This may present as acute encephalopathy, retinopathy, kidney injury, and/or hematuria [7,8]. Increased blood pressure results in mechanical stress and widespread endothelial dysfunction, leading to capillary leakage and hyperperfusion with disruption of pressure regulation in the arterioles and development of TMAs [8,9]. Unfortunately, the diagnosis of malignant HTN is often missed and only established once there is end-organ damage [10]. The absence of treatment can lead to poor prognosis, so identification and blood pressure management are key. Malignant HTN can have substantial long-standing effects if not treated.
Malignant HTN can affect multiple organ systems, including the pulmonary and renal systems. Malignant HTN causes increased permeability of the endothelium, which can lead to fibrin deposits, smooth muscle necrosis, and vascular injuries at the capillary level [9]. In the pulmonary system, HTN acts through small vessel and capillary inflammation, leading to fibrinoid necrosis. On renal histology, there can be ischemic retraction of the glomeruli as well as small artery lesions like concentric medial smooth muscle hypertrophy, also known as onion skinning [9]. Due to damage of the capillaries, RBCs cross the capillary membrane and enter the alveoli [1,2,11]. On BAL, there is often some blood; however, this contrasts with PRS, where there is DAH, which presents with progressively bloody aspirates from the BAL [2]. In the kidneys, HTN presents as fibrinoid necrosis of the afferent arterioles and proliferative endarteritis of the arteries, narrowing the arterial lumen and causing ischemia [1]. This contrasts with PRS, where kidney biopsy presents as glomerulonephritis. Unfortunately, 63% of patients who present with malignant HTN already have renal impairment [1]. In patients with end-organ damage in the renal system, renal recovery is often poor at five years, with a risk of dialysis dependence despite adequate blood pressure control [6,10]. Overall, early identification of high blood pressure and management with lifestyle changes and oral hypertensives is critical in preventing downstream end-organ effects.
Only a handful of cases of malignant HTN mimicking PRS are documented in the literature. Park et al. [7] reported a patient with no history of HTN presenting with HTN, hemoptysis, and elevated creatinine levels, accompanied by microscopic hematuria and proteinuria. This patient was initially started on steroid therapy before a negative immunological workup. In addition, Yong and Power [1] report a patient with an almost decade-long history of uncontrolled HTN presenting with hemoptysis, headache, and epigastric pain; in this case, he was treated with steroids, cyclophosphamide, and plasma exchange before a negative immunological workup. While this combination of pulmonary and renal damage is often due to immunological conditions, it is important to consider malignant HTN in the diagnosis. This case illustrates how malignant HTN can lead to end-organ damage in the lungs and kidneys, mimicking a rare diagnosis like PRS.
Conclusions
This case highlights the importance of keeping malignant HTN in the differential diagnosis, especially when the patient presents with uncontrolled HTN. Recognition and management of malignant HTN is crucial in preventing further end-organ damage. Overall, this case illustrates how malignant HTN can lead to multiple end-organ damage to mimic a rare diagnosis like PRS. This is important because there are only a handful of cases of malignant HTN mimicking PRS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Malignant hypertension causing a pulmonary-renal syndrome Case Rep Nephrol Yong B Power DA 3273695201820183065203510.1155/2018/3273695 PMC 6311832 · doi ↗ · pubmed ↗
- 2Pulmonary renal syndrome: a clinical review Breathe (Sheff) Boyle N O'Callaghan M Ataya A Gupta N Keane MP Murphy DJ Mc Carthy C 2202081820223686594310.1183/20734735.0208-2022 PMC 9973488 · doi ↗ · pubmed ↗
- 3Malignant hypertension with a rare complication of pulmonary alveolar hemorrhage Am J Nephrol Hida K Wada J Odawara M Kunitomi M Hayakawa N Kashihara N Makino H 64672020001064487110.1159/000013558 · doi ↗ · pubmed ↗
- 4Pulmonary-renal syndromes: an update for respiratory physicians Respir Med Mc Cabe C Jones Q Nikolopoulou A Wathen C Luqmani R 1413142110520112168473210.1016/j.rmed.2011.05.012 · doi ↗ · pubmed ↗
- 5Pulmonary-renal syndrome. Merck Manuals The Merck Manuals 10 2023 Lee J Rahway, NJ Merck & Co.2023 https://www.merckmanuals.com/professional/pulmonary-disorders/diffuse-alveolar-hemorrhage-and-pulmonary-renal-syndrome/pulmonary-renal-syndrome
- 6Bench-to-bedside review: pulmonary-renal syndromes--an update for the intensivist Crit Care Papiris SA Manali ED Kalomenidis I Kapotsis GE Karakatsani A Roussos C 2131120071749329210.1186/cc 5778 PMC 2206392 · doi ↗ · pubmed ↗
- 7Malignant hypertension with an unusual presentation mimicking the immune mediated pulmonary renal syndrome Yonsei Med J Park HS Hong YA Chung BH 122412275320122307412710.3349/ymj.2012.53.6.1224 PMC 3481392 · doi ↗ · pubmed ↗
- 8Malignant hypertension and multiorgan damage: mechanisms to be elucidated and countermeasures Hypertens Res Saito T Hasebe N 1221234420213302898810.1038/s 41440-020-00555-4 · doi ↗ · pubmed ↗