Indocyanine green fluorescence imaging for accurate detection of an intramural coronary artery during robotic coronary artery bypass grafting
Zain Khalpey, Ujjawal Kumar, Zacharya Khalpey, Tyler Phillips, Feras Khaliel

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
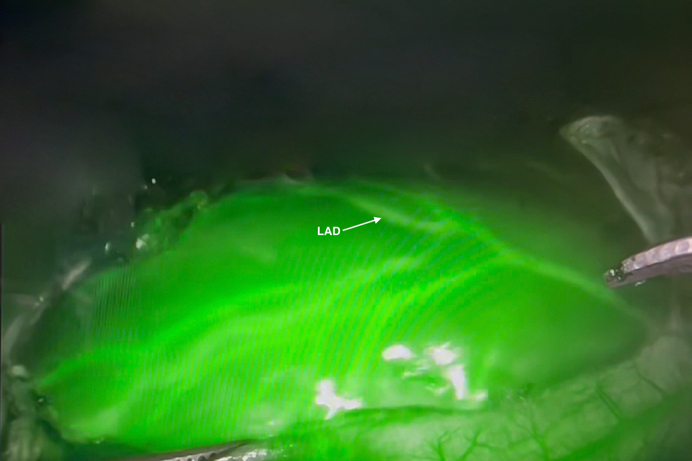 Figure 1
Figure 1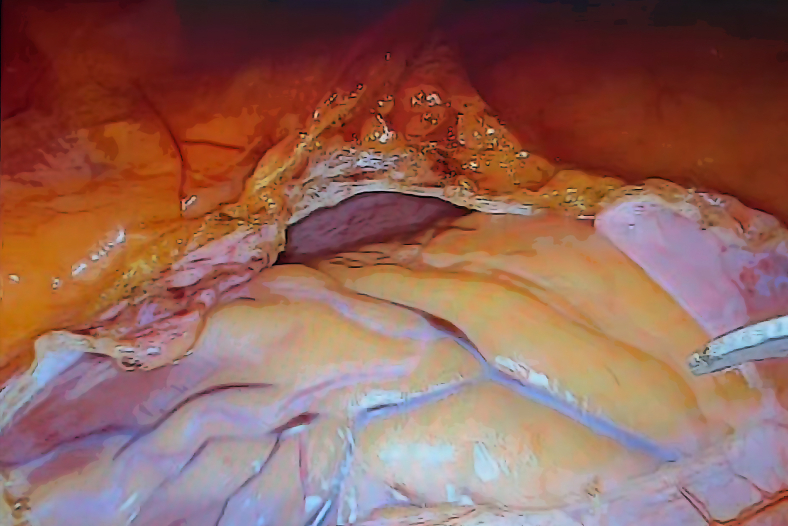 Figure 2
Figure 2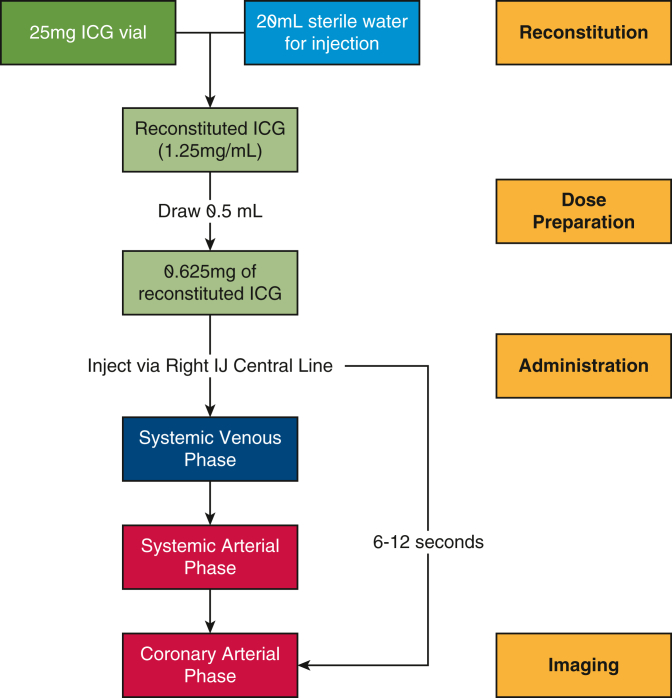 Figure 3
Figure 3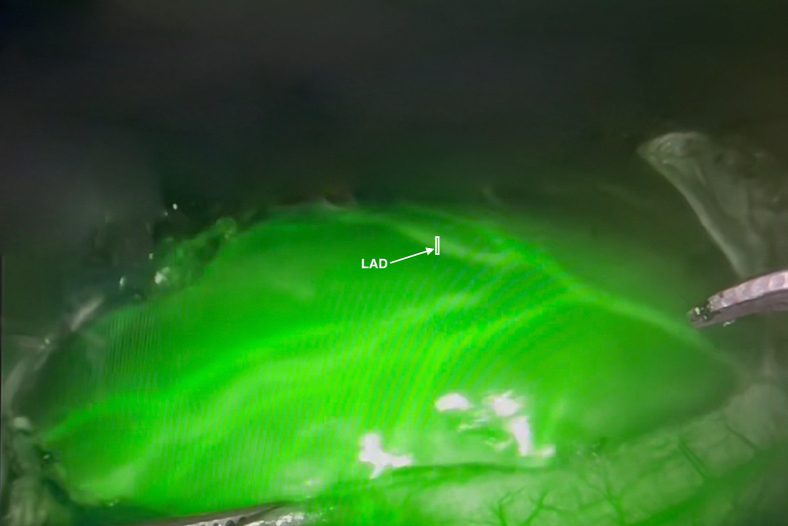 Figure 4
Figure 4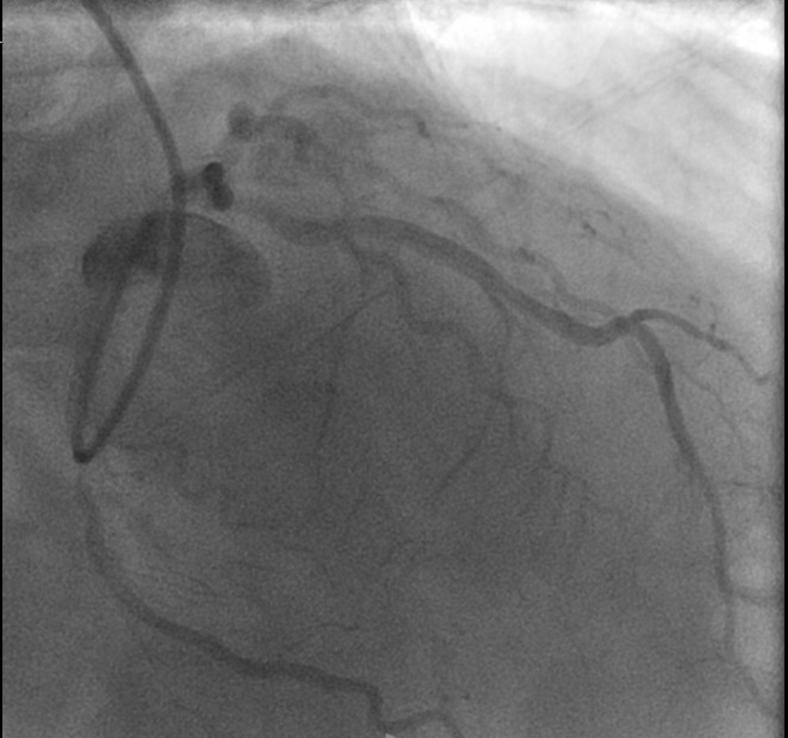 Figure 5
Figure 5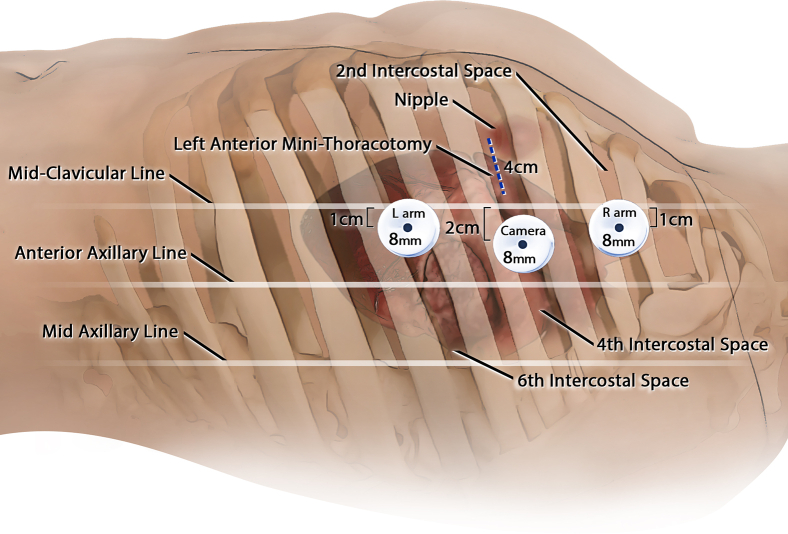 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac and Coronary Surgery Techniques · Coronary Artery Anomalies · Aortic Disease and Treatment Approaches
Successful intraoperative visualization of the LAD using ICG and Firefly mode. Central MessageIntraoperative fluorescence imaging using indocyanine green enabled precise visualization of an intramural left anterior descending coronary artery during robotic MIDCAB, facilitating successful coronary revascularization.
Intramural coronary arteries provide technical challenges during coronary artery bypass grafting (CABG). Found in approximately 42% of individuals1 these vessels can lead to myocardial ischemia, arrhythmias, and sudden cardiac death. Traditional angiography has significant limitations in precisely localizing intramural segments,2 resulting in prolonged dissection/operative times and increasing the risk of myocardial damage. We present near-infrared fluorescence (NIRF) imaging as a solution for intraoperative visualization of intramural vessels. Institutional review board approval requirement waived; written patient consent for publication was received.
Case Report
A 57-year-old man with a history of hyperlipidemia and prior orthopedic surgeries was evaluated. Preoperative cardiac catheterization (Figure 1) revealed 90% proximal left anterior descending artery (LAD) stenosis and 70% midvessel stenosis in the left circumflex artery (LCx), correlating with anterior and inferior wall ischemia on nuclear stress testing (left ventricular ejection fraction, 67%). An intramural course of the LAD was also noted. Because postoperative rehabilitation would be challenging (the patient has severely limited mobility), hybrid revascularization with robotic minimally invasive direct coronary artery bypass (MIDCAB) to the LAD and staged percutaneous coronary intervention to the LCx was planned.Figure 1. Preoperative angiography: proximal left anterior descending coronary artery and mid-left circumflex artery stenosis.
Incisions were made, ports were introduced, and the da Vinci Xi robotic system (Intuitive) was docked (Figure 2). The left internal thoracic artery was robotically harvested with a 1-cm intrathoracic fascial pedicle. Visualizing the LAD's course proved challenging (Figure E1). Indocyanine green (ICG) was prepared (Figure E2) and 0.5 mL of reconstituted ICG solution (1.25 mg/mL) was administered following pericardial opening. Fluorescence imaging (Firefly; Intuitive) in the arterial phase delineated the LAD's path (Figure E3), and a mammary clip was placed on the overlying epicardial fat as a marker allowing the anastomosis to be completed in the typical MIDCAB technique. Native flow was temporarily occluded with silastic tapes and the flow was measured using Medistim (Medistim), showing excellent graft function (pulsatility index, 2.1; flow, 12 mL/min). Intercostal nerves 3 through 5 were ablated for postoperative pain management using a cryoprobe (cryoICE; AtriCure). Echocardiography demonstrated preserved ejection fraction with negligible valvular insufficiency.Figure 2. Setup for robot-assisted minimally invasive direct coronary artery bypass.
Postoperative recovery was uncomplicated; he was discharged from the intensive care unit on postoperative day 1 and from the hospital on postoperative day 3. At 2 weeks, he reported minimal discomfort managed with acetaminophen only and was walking 1 mile daily. Staged percutaneous coronary intervention to the left circumflex coronary artery completed revascularization 1 month postoperatively. The interventional cardiologist confirmed a patent graft to the LAD. At 9 months, the patient has had no further anginal episodes or electrocardiogram changes, with increasing exercise tolerance and no residual pain.
We present the successful application of robotic cardiac surgery in a patient with functional limitations that achieved complete revascularization while avoiding sternotomy. The use of ICG-guided NIRF imaging facilitated precise grafting and minimized operative time and the minimally invasive approach enabled rapid postoperative recovery.
Comment
Successful identification and bypass of intramural coronary arteries represents a significant technical challenge in coronary revascularization. This case demonstrates the novel application of ICG-guided NIRF imaging to localize an intramural LAD during robotic MIDCAB, preventing conversion to sternotomy. Although ICG-guided NIRF imaging is well established for evaluating anastomoses and graft flow in CABG surgery,3 its utility in delineating intramural coronary anatomy is novel. Further, the literature is sparse regarding its use for identifying the course of intramural coronary vessels.
NIRF coronary angiography with ICG has shown promise in providing real-time visualization of coronary arteries, bypass grafts, and myocardial perfusion during CABG surgery.4 Developments in imaging systems have allowed simultaneous capture of color and NIR images, improving visualization of both grafts and perfusion abnormalities.5 ICG-NIRF imaging allows real-time visualization of coronary anatomy, reduced need for extensive dissection to identify vessel course, and assessment of graft patency at completion. In minimally invasive approaches such as totally endoscopic coronary artery bypass, it could ensure the correct trajectory is maintained during LAD dissection. NIRF could aid robotic grafting to the right coronary artery, addressing the challenge of vessel localization in minimally invasive approaches. This aligns with broader trends toward minimally invasive cardiac surgery and increasing integration of advanced imaging technologies in surgical decision making.
Conflict of Interest Statement
The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hostiuc S.Negoi I.Rusu M.C.Hostiuc M.Myocardial bridging: a meta-analysis of prevalence J Forensic Sci 63420181176118510.1111/1556-4029.1366529044562 · doi ↗ · pubmed ↗
- 2Nykonenko A.Feuchtner G.Nykonenko O.Feasibility of CCTA for guidance of CABGJ Cardiovasc Comput Tomogr 153202128128410.1016/j.jcct.2020.09.00532981883 · doi ↗ · pubmed ↗
- 3Reuthebuch O.Häussler A.Genoni M.Novadaq SPY: intraoperative quality assessment in off-pump CABG Chest 1252200441842410.1378/chest.125.2.41814769718 · doi ↗ · pubmed ↗
- 4Detter C.Russ D.Iffland A.Near-infrared fluorescence coronary angiography: a new noninvasive technology for intraoperative graft patency control Heart Surg Forum 54200236436912538119 · pubmed ↗
- 5Handa T.Katare R.G.Sasaguri S.Sato T.Preliminary experience for the evaluation of the intraoperative graft patency with real color charge-coupled device camera system: an advanced device for simultaneous capturing of color and near-infrared images during CABG Interact Cardiovasc Thorac Surg 92200915015410.1510/icvts.2008.20141819423513 · doi ↗ · pubmed ↗