The effect of neuromuscular training on an edentulous patient with unstable mandibular position and uncoordinated mandibular movements: a clinical report
Hong Zhang, Shuying Hu, Yue Li, Xiaojing Yang, Mei Rui, Xiaoping Luo

TL;DR
This clinical report shows that neuromuscular training with therapeutic dentures can improve jaw position and movement in edentulous patients, leading to better denture outcomes.
Contribution
The study demonstrates that neuromuscular training using therapeutic dentures can stabilize jaw position and coordination in edentulous patients.
Findings
Neuromuscular training improved the patient's unstable mandibular position.
Masticatory exercises enhanced mandibular movement coordination.
Definitive dentures achieved satisfactory results after neuromuscular training.
Abstract
The edentulous patients with unstable mandibular position (MP) and uncoordinated mandibular movement (MM) usually complain the poor therapeutic effect when conventional complete dentures (CCDs) are delivered. This case report aims to observe whether neuromuscular training (NT) using therapeutic complete dentures (TCDs) can improve the MP and MM, thereby promoting the effect of the definitive dentures. NT was conducted using TCDs for an edentulous patient with unstable MP and uncoordinated MM. After a period of masticatory exercises, the patient’s MP and MM improved. Finally, the definitive dentures were delivered, achieving satisfactory results. NT with TCDs can improve unstable MP and uncoordinated MM, leading to successful rehabilitation in edentulous patient.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2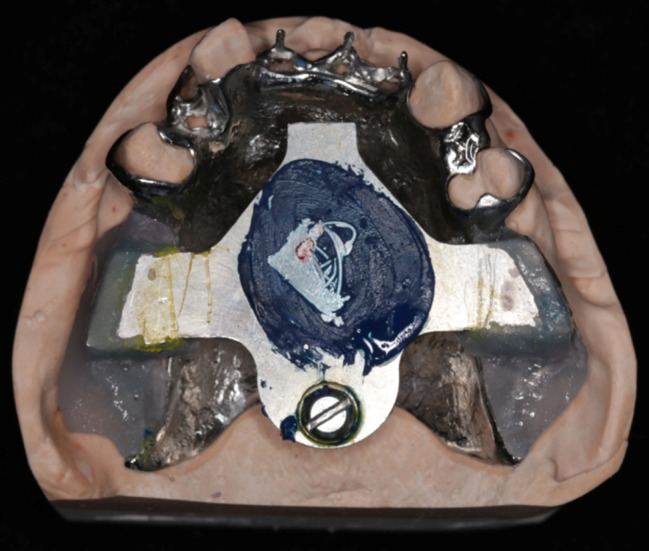 Figure 3
Figure 3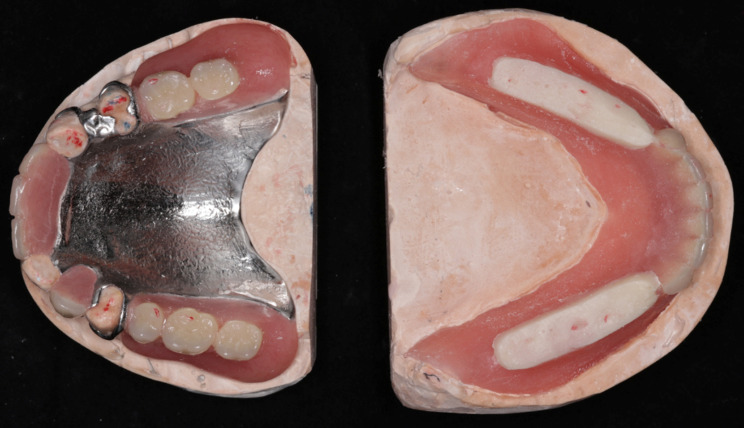 Figure 4
Figure 4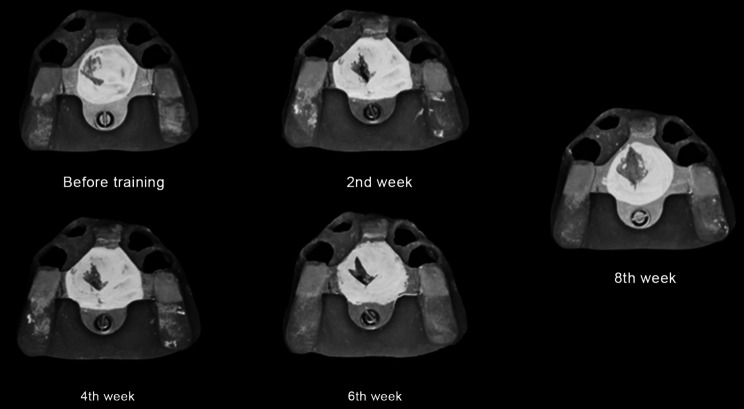 Figure 5
Figure 5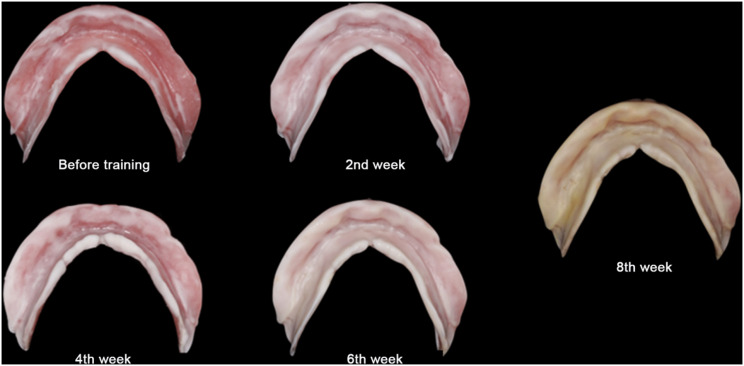 Figure 6
Figure 6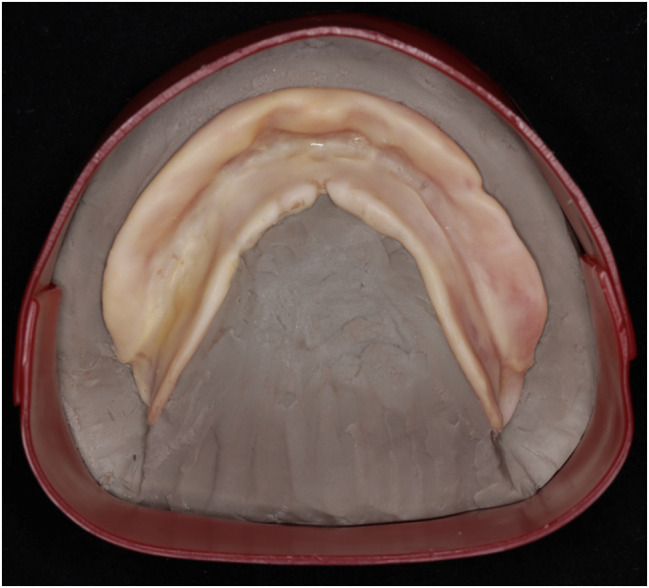 Figure 7
Figure 7 Figure 8
Figure 8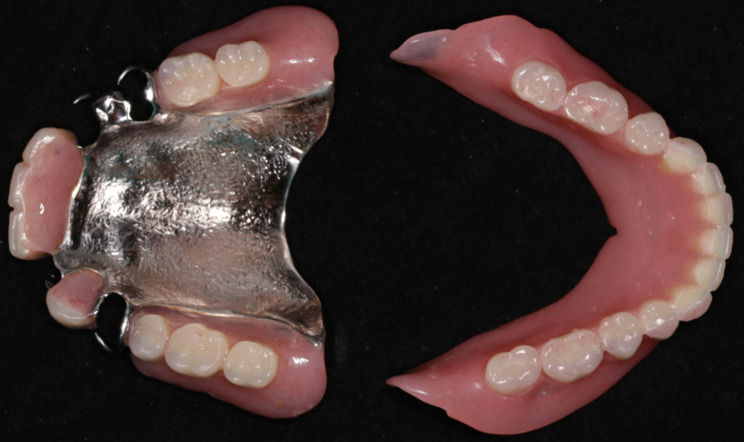 Figure 9
Figure 9- —‘3456’ Cultivation Program For Junior Talents of Nanjing Stomatological School, Affiliated Hospital of Medical School, Research Institute of Stomatology, Nanjing University
- —Jiangsu Seniors Health research Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTemporomandibular Joint Disorders · Botulinum Toxin and Related Neurological Disorders · Stroke Rehabilitation and Recovery
Background
Accurate mandibular position (MP) and coordinated mandibular movements (MM) are critical for functional rehabilitation in edentulous patients [1, 2]. However, unstable MP and uncoordinated MM are increasingly common in edentulous patients, often caused by poor chewing habits and some systemic conditions such as cerebral palsy, Bell’s palsy, and Parkinson’s disease [3–5]. These conditions can lead to unstable occlusion, making chewing difficult and increasing occlusal interference [6].
Even when centric occlusion is established based on the apex point of gothic arch tracing (GAT) trajectory, these patients frequently complain of poor retention, bad stability, pain, and recurrent mucosal ulcers when using conventional complete dentures (CCDs) [7]. Furthermore, occlusal trauma due to unstable MP and uncoordinated MM is especially harmful in implant-supported complete dentures, leading to complications like fractured artificial teeth, cracked bridge frameworks, peri-implantitis, implant loosening, and, in more serious cases, temporomandibular joint dysfunction and orofacial pain [8].
Therapeutic complete dentures (TCDs) with flat occlusal tables in the mandibular denture allow unrestricted voluntary movements, promoting neuromuscular adaptation by reducing occlusal interference and enabling repetitive masticatory exercises to restore coordinated muscle function. These dentures have shown promise in improving treatment effect for edentulous patients with complex conditions. Previous reports have demonstrated the successful stabilization of complete dentures in patients with cerebral palsy, Bell’s palsy, and Parkinson’s disease using TCDs [3–5]. It has been suggested that when flat table treatment dentures are used, the oral mucosa provides sensory feedback regarding vertical stop and bite force, leading to increased activation of the masseter muscle [3]. However, detailed protocols for therapeutic procedures, including specific methods, duration, and efficacy, are not well documented, and the underlying mechanism of treatment remains unclear.
This clinical report presents a detailed protocol for neuromuscular training (NT) in an elderly edentulous male patient with an unstable MP and uncoordinated MM. The effectiveness of NT was systematically evaluated, and the final definitive dentures achieved satisfactory results. Through this case report, we aim to provide a reproducible and practical therapeutic approach for managing similar patients.
Case presentation
An 82-year-old male patient presented at Nanjing Stomatological Hospital, Affiliated Hospital of Medical School, Institute of Stomatology, Nanjing University (Nanjing, China), complaining of tooth loss and recovery his chewing ability. He reported a decade-long history of unsuccessful attempts to use removable partial dentures (RPDs) due to their ineffectiveness and pain during mastication, which led him to rely solely on his right premolars for chewing. However, three months ago, he lost his right mandibular premolars, rendering him unable to chew any food, significantly affecting his nutritional intake and overall quality of life. The patient was in good general health, with no history of severe systemic diseases (e.g., hypertension, diabetes, or cardiovascular disorders), psychiatric conditions, or neurological deficits (e.g., Parkinson’s disease or stroke). He also reported no pain in the temporomandibular joints and denied smoking, alcohol consumption, or any parafunctional habits. Clinical examination revealed four natural teeth without obvious mobility in the maxillary arch and edentulous mandibular arch. The mandibular residual ridge was well-rounded (Atwood Type I), and the oral mucosa was well-keratinized. A treatment plan proposing an implant-supported overdenture for the mandible and a RPD for the maxilla was presented. However, the patient opted for a removable prosthesis for both arches, avoiding surgery.
Routine procedures were initiated for both the maxillary and mandibular dentures. The maxillary master cast and mandibular preliminary cast were made, and the metallic framework for the maxillary RPD and the mandibular occlusion registration plate were fabricated (Fig. 1). Occlusion registration was recorded using check-bite method with wax rims. However, at the first try-in, the patient’s mandible exhibited a habitual forward and rightward shift during mouth closure (Fig. 2). To confirm the centric relationship, GAT (Gnathometer M, Ivoclar Vivadent AG), mounted on the maxillary metallic framework and the mandibular occlusion plate, was used. The patient was seated upright with proper head support, and instructed to perform protrusive, retrusive and lateral jaw movements. Then the rapid and continuous tapping movements were also instructed. GAT trajectory showed scattered tapping points far from the apex point, along with a noticeable deficiency in left MM paths (Fig. 3).
Fig. 1. The left side showed the maxillary master cast and the mandibular preliminary cast, while the right side displayed the maxillary metallic framework and the mandibular occlusion registration plate
Fig. 2. At the first try-in, the patient’s mandible exhibited a habitual forward and rightward shift during mouth closure
Fig. 3. Before NT, GAT trajectory showed scattered tapping points far from the apex point, along with a noticeable deficiency in left MM paths
Given the negative impact of the unstable MP and uncoordinated MM, NT with TCDs before the definitive dentures delivered was recommended. After a detailed explanation, the patient consented to the treatment protocol.
The horizontal jaw relationship was re-established at the apex point based on GAT trajectory, and the occlusal plane was transferred with a face bow. The maxillary RPD was fabricated following standard procedures. The mandibular posterior artificial teeth were instead of flat occlusal tables, paralleled to the occlusal plane. They were made of a mixture of auto-polymerizing acrylic resin and zinc oxide powder in a 1:1 ratio, allowing only the maxillary functional cusps to contact them, without any cusp-fossa interlocks (Fig. 4). The mucosal surface of the mandibular denture base was lined with tissue conditioner (TC) (Coe-Comfort, GC Ltd.).
Fig. 4. The point-flat contacts without cusp-fossa interlocks between the maxillary functional cusps and mandibular flat tables
After the delivery of the TCDs, the patient was instructed to perform NT through masticatory exercises at least three times a day—during breakfast, lunch, and dinner— with each session lasting a minimum of 30 min. The progression of food texture was carefully planned, transitioning gradually from soft to normal foods. Weeks 1–2: Soft foods such as noodles, porridge, steamed eggs, and tofu were recommended to minimize mucosal pressure and allow initial adaptation. Weeks 3–4: Semi-solid foods, including rice, fish, tomatoes, scrambled eggs, and ground meat, were introduced to gradually increase the masticatory load. Weeks 5–8: Solid foods, such as nuts, raw cucumber, braised pork, and stewed chicken, were incorporated to simulate natural chewing demands and further enhance neuromuscular coordination. Advancement to the next food texture level was permitted only if the patient reported no mucosal pain or ulceration after chewing, ensuring a comfortable and progressive adaptation process. Follow-up visits were scheduled every two weeks to adjust the occlusal contacts and TC layer. Initially, unbalanced indentations were observed on the mandibular flat tables, and these, along with any obvious cusp-fossa interlocks, were adjusted to balanced point-flat contacts. Any flushed areas on TC layer were ground down and relined with new TC. GAT trajectory was observed at each visit to monitor the changes of MP and MM.
At the eighth-week follow-up, GAT trajectory returned to a typical arrowhead shape (Fig. 5), with clear indentations on the mandibular flat tables and no flushed areas on TC layer (Fig. 6). At this time point, NT was deemed complete, and the definitive mandibular denture was fabricated. The relationship between the maxilla and mandible was recorded using silicone bite registration material (Virtual CADbite Registration, Ivoclar Vivadent AG), and TC layer was used as a dynamic functional impression (Fig. 7). The mandible final try-in denture was made and evaluated in the patient’s mouth (Fig. 8). Finally, the definitive mandibular complete denture was fabricated (Fig. 9).
Fig. 5GAT trajectories indicated an improvement in mandibular movement paths during NT
Fig. 6TC layers on the mucosa surface of the denture base became more uniform
Fig. 7. The ultimate TC layer served as the dynamic functional impression for the definitive mandibular dentures
Fig. 8. The final try-in dentures were in the mouth
Fig. 9. The definitive maxillary and mandibular dentures were delivered
The patient’s satisfaction regarding retention, stability, chewing ability and phonetics was evaluated using a Visual Analog Scale (VAS) method at each follow-up visit, and 1 day, 1 month, 6 months, and 1 year after the definitive dentures were delivered (see Table 1).
Table 1. The VAS grades (0–10 scale) of the retention, stability, chewing ability and phoneticsTime pointsRetentionStabilityChewing abilityPhoneticsBefore training32142 weeks training53264 weeks training65586 weeks training888108 weeks training1098101 day after delivered1098101month after delivered1098106 months after delivered10109101 year after delivered10101010
Discussion and conclusions
In natural teeth, the signals of occlusal contacts are perceived by mechanoreceptors within the periodontium, which activate sensorimotor circuits and provide feedback to promote rhythmic jaw movements [9]. However, in edentulous patients, these signals are received by the mucosa beneath the denture base and the perioral muscles [10]. In this case, due to long-term tooth loss and ill-fitting dentures, the input signals from the oral mucosa and muscles are significantly reduced and inaccurate, leading to neuromuscular dysfunction. At the first try-in, the patient showed unstable MP and the patient’s mandible exhibited a habitual forward and rightward shift during mouth closure.
To resolve the poor chewing habit, normal neuromuscular function must be rebuild. Previous studies have demonstrated that repetitive motor training, such as tooth clenching [11], hold-and-split training for anterior teeth [12], and tongue movements [13, 14], can induce cortical plasticity of the jaw muscles, optimizing muscle function. In this case, we suspected that the mechanism of TCDs treatment is plasticity in the motor cortex of the masticatory muscles induced by repeated masticatory exercises. Only with restored neuromuscular function can dentures serve as effective tools for regaining optimal chewing function.
As an appliance of NT, TCDs are characterized by point-flat contacts between the functional cusps of the maxillary denture and the flat tables of the mandibular denture, allowing voluntary mandibular movements without restriction [4]. To maintain voluntary movement, regular occlusal adjustments are crucial at each follow-up visit. In this case, after a period of masticatory exercises, the indentations became more balanced, indicating improved MM.
GAT is a simple and effective technique for determining the centric relationship between maxilla and mandible (apex point) [15]. By analyzing the relationship between the muscular contact position (tap point) and the apex point, as well as the lateral mandibular movement paths, neuromuscular function can be inferred [16, 17]. In this case, after a period of NT, GAT showed an improved trajectory, finally approaching the typical arrowhead shape, indicating improvements in MP and MM. Instead of relying on clinician’s experience, the typical arrowhead shape serves as a clear indicator for terminating of TN. Therefore, using GAT to guide the therapeutic process is more precise and practical, making it a valuable approach to promote in future clinical practice.
TC is a viscous gel with viscoelastic properties [18] that can help restore inflamed oral mucosa beneath the denture base, record dynamic functional impressions, adjust occlusal force distribution, and alleviate pain [19–21]. In this case, changes in TC layer during treatment reflected the effects of NT, and its final uniformity indicated improvements in MP and MM. However, due to ethanol evaporation and the aging of plasticizers, TC layer gradually loses its viscoelastic properties, requiring reapplication every two weeks [22]. Ultimately, TC layer served as the dynamic functional impression for the definitive mandibular denture [23].
Although the satisfaction questionnaire is a subjective evaluation method, it is widely used in the bio-psycho-social model of medical care to assess treatment effect in edentulous patients [24]. In this case, the patient’s subjective evaluations aligned with the objective results from GAT trajectory and TC performance, confirming the effectiveness of NT with TCDs. Throughout NT period and after the delivery of the definitive dentures, the patient reported none of the pain he had experienced with traditional dentures.
While this case demonstrates the effectiveness of TCDs, further research is needed to clarify the effects of NT on the brain, masticatory muscles, and condylar position by transcranial magnetic stimulation (TMS), electromyography (EMG), or cone beam computed tomography (CBCT).
Neuromuscular training with therapeutic complete dentures can improve unstable mandibular positions and uncoordinated mandibular movements, leading to successful rehabilitation in edentulous patients.