Pericardiectomy using an ultrasonic scalpel in patients with constrictive pericarditis
Takashi Yoshinaga, Jun Takaki, Kosuke Nakata, Takafumi Hirota, Hideaki Hidaka, Tatsuya Horibe, Ken Okamoto, Toshihiro Fukui

TL;DR
This paper reports on the successful use of an ultrasonic scalpel for radical pericardiectomy in patients with constrictive pericarditis.
Contribution
The study presents the first consecutive case series of radical pericardiectomy using an ultrasonic scalpel.
Findings
Radical pericardiectomy using an ultrasonic scalpel was performed successfully in 10 patients.
There were no operative deaths, and most patients improved to NYHA class I postoperatively.
Abstract
Pericardiectomy using an ultrasonic scalpel is the effective operative treatment of chronic pericarditis. However, no consecutive case series of radical pericardiectomy using an ultrasonic scalpel has been reported. We retrospectively reviewed the records of 10 patients who underwent a radical pericardiectomy with an ultrasonic scalpel between April 2015 and March 2024. Preoperative and postoperative variables were reviewed. The median age was 65 years, and 3 patients were female. Three patients had preoperative atrial fibrillation. Forty percent of patients were in NYHA class 3–4. Three patients underwent urgent operations. An ultrasonic scalpel was used for the dissection and resection of thickened parietal pericardium and visceral pericardium around the heart except in the area of the posterior left atrium in all patients. Three patients underwent the off-pump technique. Coronary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
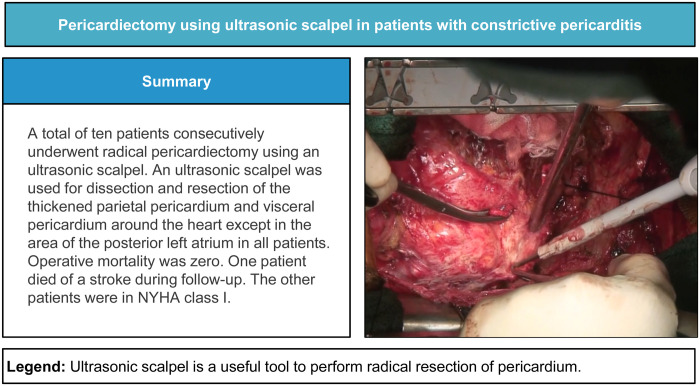 Figure 1
Figure 1| Variable | All patients ( |
|---|---|
| Age (years) | 65 [55.8–68.5] |
| Women | 3 (30%) |
| Body mass index | 21.9 ± 6.4 |
| Hypertension | 4 (40%) |
| Diabetes mellitus | 5 (50%) |
| Hyperlipidemia | 2 (20%) |
| Smoking history | 7 (70%) |
| Previous stroke | 1 (10%) |
| Peripheral vascular disease | 0 |
| Haemodialysis | 2 (20%) |
| Prior myocardial infarction | 0 |
| NYHA class 3–4 | 4 (40%) |
| Atrial fibrillation | 4 (40%) |
| Previous cardiac surgery | 0 |
| Variable | All patients ( |
|---|---|
| Concomitant procedures | 4 (40%) |
| Without cardiopulmonary bypass | 3 (30%) |
| Operation time (min) | 248 (211.5–391.8) |
| Cardiopulmonary bypass time (min) | 117 (107.5–137) |
| Operative deaths | 0 |
| Stroke | 0 |
| Use of haemodynamic support device | 0 |
| Respiratory failure | 0 |
| New haemodialysis | 1 (10%) |
| Mediastinitis | 1 (10%) |
| New atrial fibrillation | 1 (10%) |
| Bleeding requiring re-exploration | 0 |
| Postoperative ICU stay (day) | 3 [2–5] |
| Preoperative | Follow-up | ||
|---|---|---|---|
| Left ventricular diastolic dimension (mm) | 34.6 ± 7.3 | 41.6 ± 5.0 | 0.010 |
| Left ventricular systolic dimension (mm) | 22.9 ± 5.2 | 27.5 ± 3.6 | 0.013 |
| Left ventricular end-diastolic volume (ml) | 45.2 ± 17.2 | 65.2 ± 17.5 | 0.012 |
| Left ventricular end-systolic volume (ml) | 18.9 ± 7.6 | 25.9 ± 7.6 | 0.018 |
| Ejection fraction (%) | 58.2 ± 4.7 | 60.4 ± 6.1 | 0.714 |
| E/A ratio | 2.4 ± 1.6 | 1.2 ± 0.4 | 0.022 |
| Deceleration time (ms) | 132.7 ± 41.5 | 195.6 ± 67.1 | 0.028 |
| 8.5 ± 3.3 | 9.0 ± 3.2 | 0.566 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Myasthenia Gravis and Thymoma · Ultrasound in Clinical Applications
INTRODUCTION
Constrictive pericarditis is a chronic and progressive inflammatory disease of the pericardium that involves pericardial scarring and fibrous thickening of the pericardium [1]. Although rare, constrictive pericarditis is one of the long-standing causes of heart failure. Although most patients with pericarditis are managed medically with diuretics, pericardiectomy is the definitive treatment for patients with uncontrolled heart failure. However, the early postoperative mortality of pericardiectomy is high, ranging from 2% to 15% [2]. Adequate pericardial resection is critical to prevent persistent haemodynamic compromise and symptoms due to residual constrictive physiology [3]. Failure to free the inferior aspect of the ventricles and remove the diaphragmatic pericardium may result in residual constriction and recurrent symptoms [4].
There have been only a few case reports on the feasibility of using an ultrasonic scalpel to dissect thickened pericardium in patients with constrictive pericarditis [5, 6]. Uchida et al. [5] reported that using an ultrasonic scalpel made it relatively easy to find the correct plane to avoid injuring the coronary arteries even though the pericardium was strongly adherent to the myocardium. We have used an ultrasonic scalpel for the treatment of constrictive pericarditis to achieve complete resection of thickened pericardium. In this study, we evaluate the effectiveness of using an ultrasonic scalpel for constrictive pericarditis.
PATIENTS AND METHODS
We studied 10 consecutive patients who underwent ultrasonic scalpel pericardiectomy for the treatment of constrictive pericarditis at the Kumamoto University Hospital. Patients who underwent concomitant procedures were included in this study. The study was approved by the research ethics committee at Kumamoto University (Approval No. 3070). The institutional review board approved this retrospective study and waived the requirement for written consent.
Our strategy for pericardiectomy was to achieve complete resection of the thickened pericardium with or without cardiopulmonary bypass. Cardiopulmonary bypass was necessary for cardiac decompression and circulatory support, especially in those patients whose lateral and infero-posterior pericardium was extremely thickened and calcified. Cardiopulmonary bypass was also required for concomitant procedures such as valve replacement.
A median sternotomy was performed in all patients. Our operative strategy and methods are similar to those described by Hemmati et al. [3]. The pericardial incision was started in the midline (Video 1). First, an electric cautery was used to create a dissection between the pericardium and epicardium. Once the correct dissection plane could be observed, dissection was performed with an ultrasonic scalpel. Our intention was to dissect the plane between the pleura and the pericardium; however, the pleural cavity is usually opened on both sides because the adhesion between the pleura and the pericardium is tight. Resection of the anterior and lateral sides of the pericardium was performed until the phrenic nerves were seen. The diaphragmatic pericardium was dissected from the inferior surface of the left and right ventricles using a heart positioner normally used for off-pump coronary artery bypass grafting. The diaphragmatic pericardium was resected from the underlying muscular and fibrous portions of the diaphragm. We resected the diaphragmatic pericardium until the inferior pulmonary veins could be seen. The right and left sides of the diaphragmatic pericardium were also resected until the phrenic nerves were visible. The fibrous tissues around the superior and inferior vena cava were also resected.
Next, we removed as much as possible of the thickened epicardium that was affected by the inflammation of the pericardium. An ultrasonic scalpel is particularly useful for epicardial resection because it causes less bleeding and does not induce ventricular arrythmias. We do not perform the “waffle procedure [7]” unless the epicardial adhesion is dense and the epicardium is difficult to remove completely. Concomitant procedures were performed after completion of the pericardiectomy.
All patients underwent echocardiography 2–3 days before the operation and 7–12 months after the operation [median 12 months (10.5–12.0)].
All statistical analyses were performed with the StatView 5.0 software package (SAS Institute Inc., Cary, NC, USA). Continuous variables are presented as the median and interquartile range or the mean ± standard deviation. Continuous variables were compared using paired t-tests. Differences were considered significant at P < 0.05.
RESULTS
We performed ultrasonic scalpel pericardiectomy in 10 patients between April 2015 and March 2024. Pericardial resection was completed in all cases. The preoperative characteristics of the patients are listed in Table 1. None of the patients had had previous cardiac operations. Three patients urgently underwent operations because they had acute heart failure with catecholamines.
Operative and postoperative data are shown in Table 2. Concomitant procedures were performed in 4 patients, including coronary artery bypass grafting in 4 patients, aortic valve replacement in 1 patient, and tricuspid valve repair in 1 patient. Cardiopulmonary bypass was used in 7 patients. Of those, 3 patients did not undergo any procedures other than pericardiectomy. There were no operative deaths. In addition, no patients experienced major postoperative complications such as stroke, bleeding requiring re-exploration, low output syndrome, perioperative myocardial infarction or respiratory failure. However, 1 patient required haemodialysis and 1 patient had mediastinitis.
Pre- and postoperative echocardiographic data are shown in Table 3. Both diastolic and systolic dimensions of the left ventricle were significantly improved. Similarly, both end-diastolic and end-systolic left ventricular volumes were significantly improved. However, the left ventricular ejection fraction did not change. Most of the parameters of left ventricular diastolic function were significantly improved after the operation.
DISCUSSION
Surgical resection represents a fundamental approach to the treatment of constrictive pericarditis. The primary objective of pericardiectomy is to achieve complete resection. The majority of surgeons perform a pericardial resection that extends to the phrenic nerve on both sides. Nevertheless, this step may lead to the persistence of left ventricular dysfunction. To achieve complete resection, it is essential to remove the pericardium from the diaphragm to the posterior aspect of the heart. We use cardiopulmonary bypass in patients whose haemodynamics are unstable during the resection of the posterior side of the heart. Furthermore, it is crucial to remove as much of the epicardium as possible. The procedure carries a significant risk of bleeding from the ventricular muscle and damage to the coronary arteries. In our institute, an ultrasonic scalpel has been used to resect the pericardium and epicardium. Uchida et al. [5] reported its usefulness in a case report and described that haemostasis was easily achieved by using an ultrasonic scalpel and that no major bleeding from the myocardium was observed. Similar to their report, none of our patients had massive bleeding caused by injury to the ventricular muscle or the coronary artery. Furthermore, it has been proposed that the use of an ultrasonic scalpel may help to avoid electrical stimulation of the muscles, which could otherwise lead to haemodynamic deterioration due to arrhythmia. In our experience, we did not observe any instances of ventricular arrhythmia caused by the use of an ultrasonic scalpel. Haemostasis was easily achieved by using an ultrasonic scalpel, and no major bleeding from the myocardium was observed. We did not observe major arrhythmia during the operation. No blood transfusions were required in 2 patients. Moreover, an ultrasonic scalpel can be used in patients with heavily calcified pericardium. It is very effective in dissecting the calcified pericardium from the epicardium. However, care should be taken not to apply too much pressure with an ultrasonic scalpel on the myocardium because of the potential risks of perforation.
In this study, the parameters of left ventricular diastolic function, as measured by echocardiography, exhibited a near-complete recovery to the normal range. Ghavidel et al. [8] suggested that left ventricular diastolic function returns to normal early after pericardiectomy in approximately 40% of patients, and late after pericardiectomy in almost 60%. In the present study, we adopted the follow-up echocardiographic data ranging from 6 to 12 months after the operation. We did this because early postoperative data are often influenced by postoperative conditions that have not sufficiently recovered.
The limitations of this clinical study are as follows: (i) the number of patients was small; (ii) we did not compare the current technique with another technique, (iii) we did not have long-term follow-up data; and (iv) we did not have data from patients undergoing other surgical methods for comparison.
CONCLUSIONS
In conclusion, radical resection of the pericardium is essential for patients with constrictive pericarditis. The utilization of an ultrasonic scalpel is safe and effective when performing a radical pericardiectomy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gillaspie EA, Stulak JM, Daly RC et al A 20-year experience with isolated pericardiectomy: analysis of indications and outcomes. J Thorac Cardiovasc Surg 2016;152:448–58.27210468 10.1016/j.jtcvs.2016.03.098 · doi ↗ · pubmed ↗
- 2Depboylu BC, Mootoosamy P, Vistarini N, Testuz A, El-Hamamsy I, Cikirikcioglu M. Surgical treatment of constrictive pericarditis. Tex Heart Inst J 2017;44:101–6.28461794 10.14503/THIJ-16-5772 PMC 5408622 · doi ↗ · pubmed ↗
- 3Hemmati P, Greason KL, Schaff HV. Contemporary techniques of pericardiectomy for pericardial disease. Cardiol Clin 2017;35:559–66.29025547 10.1016/j.ccl.2017.07.009 · doi ↗ · pubmed ↗
- 4Cho YH, Schaff HV, Dearani JA et al Completion pericardiectomy for recurrent constrictive pericarditis: importance of timing of recurrence on late clinical outcome of operation. Ann Thorac Surg 2012;93:1236–40.22386088 10.1016/j.athoracsur.2012.01.049 · doi ↗ · pubmed ↗
- 5Uchida T, Bando K, Minatoya K, Sasako Y, Kobayashi J, Kitamura S. Pericardiectomy for constrictive pericarditis using the harmonic scalpel. Ann Thorac Surg 2001;72:924–5.11565688 10.1016/s 0003-4975(00)02436-x · doi ↗ · pubmed ↗
- 6Di Luozzo G, Moussa F, Schor J, Traad E, Williams D, Carrillo R. Harmonic scalpel for pericardiectomy: novel approach to an old cardiac dilemma. Heart Surg Forum 2004;7:E 525–7.10.1532/HSF 98.2004109115799939 · doi ↗ · pubmed ↗
- 7Matsuura K, Mogi K, Takahara Y. Off-pump waffle procedure using an ultrasonic scalpel for constrictive pericarditis. Eur J Cardiothorac Surg 2015;47:e 220–2.25656404 10.1093/ejcts/ezu 554 · doi ↗ · pubmed ↗
- 8Ghavidel AA, Gholampour M, Kyavar M, Mirmeshdagh Y, Tabatabaie MB. Constrictive pericarditis treated by surgery. Tex Heart Inst J 2012;39:199–205.22740731 PMC 3384050 · pubmed ↗