Unusual coronary artery disease presentation: take the time to bury the hatchet and the stent, a case report
Julien Rosencher, Cindy Marques, Ghilas Raouhal, Patrice Cacoub

TL;DR
A rare case of coronary artery disease caused by inflammation was correctly diagnosed using advanced imaging, avoiding unnecessary procedures.
Contribution
Demonstrates the diagnostic value of multimodal imaging in identifying inflammatory causes of atypical coronary artery disease.
Findings
Multimodal imaging confirmed large vessel vasculitis as the cause of atypical CAD in a 74-year-old patient.
Treatment with anti-inflammatory drugs resolved symptoms and reversed arterial thickening without revascularization.
FDG-PET and CCTA were critical in diagnosing coronary arteritis missed by conventional angiography.
Abstract
Coronary artery disease (CAD) secondary to coronary arteritis (CA) is a rare and challenging condition to diagnose, often resulting in poor clinical outcomes. Conventional coronary angiography lacks the sensitivity to identify inflammatory causes, leading to underdiagnosis and inappropriate treatment. Advanced imaging techniques, particularly cardiac computed tomography angiography (CCTA), appear to be invaluable tools to correctly identifying CA as the underlying cause of atypical CAD. We describe the case of a 74 year old patient without traditional risk factor who presented with chest pain, a positive clinical and electrical stress test. Given the highly atypical form of CAD on CCTA characterized by a diffuse, circumferential thickening of coronary arteries, an inflammatory cause was suspected. Large vessel vasculitis was confirmed by fluorodeoxyglucose-positron emission tomography…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
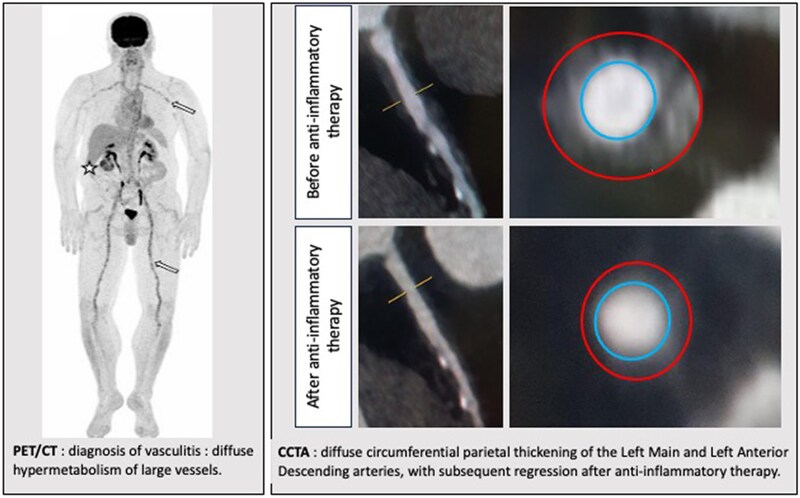 Figure 1
Figure 1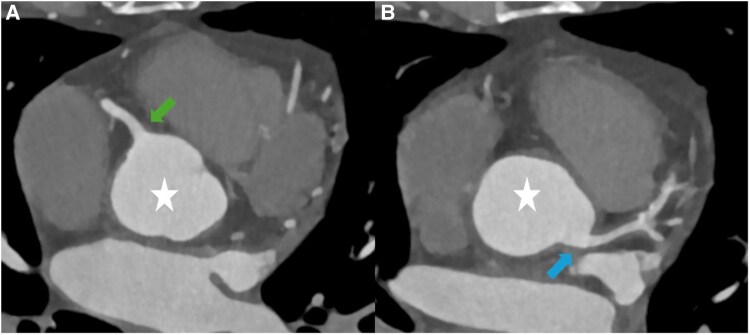 Figure 1
Figure 1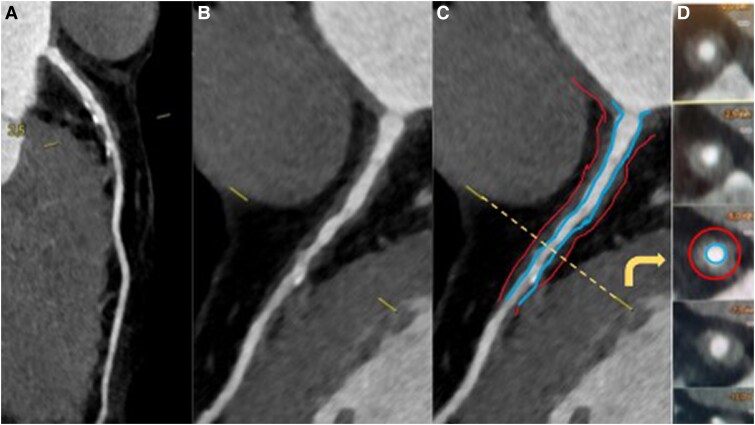 Figure 2
Figure 2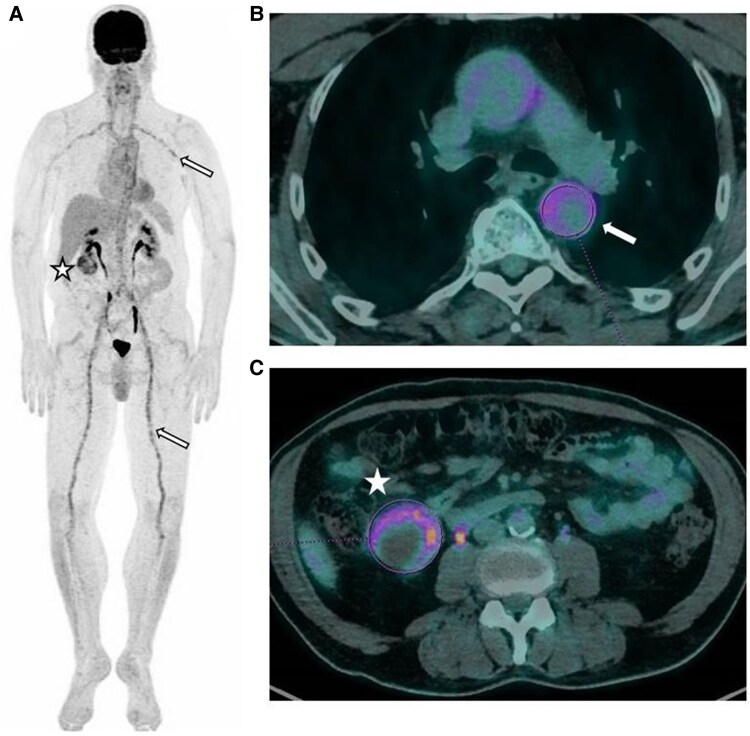 Figure 3
Figure 3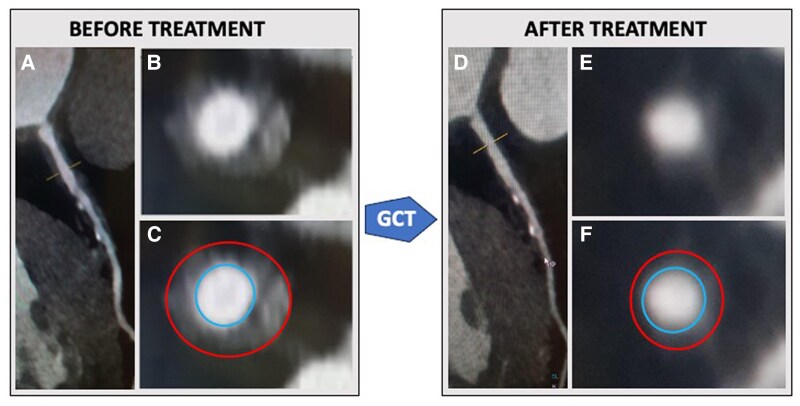 Figure 4
Figure 4| Disease | Description | Common imaging features | Differentiating features |
|---|---|---|---|
| Atherosclerotic CAD | Progressive narrowing of coronary arteries due to lipid and plaque deposition | Eccentric stenosis, calcifications, and plaque formation on angiography or CCTA | Presence of traditional risk factors (diabetes and hypertension), absence of systemic inflammation |
| Takayasu arteritis | Large vessel vasculitis affecting the aorta and its branches, often seen in young females | Long, smooth stenosis or occlusion, arterial wall thickening (>2 mm) on CT or MRI, circumferential wall thickening with FDG-PET hypermetabolism | Often involves aortic arch vessels; systemic symptoms such as fever, malaise, and claudication; functional and morphological sequalae of previous flares |
| Giant cell arteritis (GCA) | Large vessel vasculitis commonly affecting older individuals | Circumferential wall thickening with FDG-PET hypermetabolism in the aorta and major branches | Associated with temporal artery tenderness, elevated C-reactive protein; possible association with polymyalgia rheumatica; histological diagnosis on temporal artery biopsy |
| IgG4-related disease | Multi-systemic fibro-inflammatory disease | Diffuse arterial wall thickening, delayed enhancement on contrast-enhanced imaging | Elevated IgG4 levels, specific lymph node or visceral involvement; characteristic histopathology on biopsy |
| Ankylosing spondylitis | Chronic inflammatory disease affecting the axial skeleton | Aortic root and ascending aorta thickening, valvular involvement on CT/MRI | Predominant musculoskeletal symptoms; sacroiliitis on imaging, HLA-B27 positivity |
| Atrophic polychondritis | Rare systemic autoimmune disease affecting the cartilages of the ears, nose, and respiratory tree | Aortic insufficiencies complicating dilatation of the aortic root, aneurysmal developments in the ascending thoracic aorta | Predominant cartilage involvement |
| Behçet's disease | Multi-systemic inflammatory disorder causing vasculitis of all vessel sizes | Aneurysms, occlusions, and stenoses of large vessels on angiography | Oral/genital ulcers, uveitis, positive pathergy test, HLA B51 positivity |
| ANCA-associated vasculitis | Small vessel vasculitis associated with anti-neutrophil cytoplasmic antibodies (ANCA) | Inflammation of small vessels, sometimes with microaneurysms, rarely affecting large vessels | Positive ANCA (p-ANCA or c-ANCA), common renal, ear nose and throat, pulmonary, or peripheral nerve involvement |
| Cogan’s syndrome | Rare autoimmune disease involving eyes and inner ears, with possible large vessel vasculitis | Aortic wall thickening and aneurysms, FDG-PET hypermetabolism | Associated with corneal and cochleovestibular damage |
| Erdheim-Chester disease | Rare non-Langerhans histiocytosis affecting multiple systems, including large vessels | Peri-aortic ‘coated aorta’ sign, FDG uptake in soft tissue surrounding vessels | Bilateral sclerotic bone lesions, CD68-positive histiocytes, BRAF mutation in many cases |
| Rheumatoid arthritis (RA) | Chronic inflammatory disease primarily affecting joints | Aortic wall thickening, coronary vasculitis on imaging in advanced disease | Predominant joint involvement, positive rheumatoid factor (RF), and anti-cyclic citrullinated peptides |
| Sarcoidosis | Granulomatous inflammatory disease affecting multiple organs | FDG-PET shows patchy vascular hypermetabolism, lymphadenopathy | Pulmonary or visceral involvement, elevation of angiotensin converting enzyme, non-caseating granulomas on biopsy |
| Polyarteritis Nodosa (PAN) | Necrotizing vasculitis of medium-sized arteries | Microaneurysms and segmental stenoses of ascending thoracic aorta on CT or MR angiography | Systemic symptoms (e.g. abdominal pain and neuropathy), association with hepatitis B |
| Kawasaki disease | Vasculitis seen in children, involving coronary arteries | Coronary aneurysms or ectasia, occasionally with thrombosis | Predominantly occurs in children; fever, rash, and conjunctivitis |
| Systemic lupus erythematosus (SLE) | Chronic autoimmune disease affecting multiple organs | Vasculitis-related stenoses or thrombosis on angiography | Systemic features (e.g. rash and joints). positive ANA, anti-dsDNA, anti-Sm, and complement consumption |
| Infectious arteritis | Arteritis caused by bacterial or fungal infections | Focal arterial wall thickening, possible abscess formation, or aneurysms | Positive blood cultures or serology, response to antibiotics/antifungal therapy |
| Tuberculosis | Chronic mycobacterial infectious that can cause aortitis in its advanced stages | Aortic wall thickening, pseudoaneurysms, and calcifications | Pulmonary or lymph node involvement, history of contagion, positive tuberculin skin test/interferon gamma release assay, granulomas with caseation on biopsy |
| Syphilis | Chronic infection, potentially causing tertiary syphilitic arteritis | Irregular vessel wall thickening with aneurysmal dilation on imaging | Positive serologic veneral disease research laboratory/treponema pallidum hemagglutination assay (VDRL/TPHA), history of untreated syphilis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Imaging and Diagnostics · Vasculitis and related conditions · Kawasaki Disease and Coronary Complications
Introduction
Coronary artery disease (CAD) secondary to coronary arteritis (CA) is a rare condition, making diagnosis challenging and often leading to poor outcomes. While certain clinical features may suggest underlying vasculitis, conventional coronary angiography lacks specific diagnostic features, which frequently results in underdiagnosis and inadequate treatment. In this case, we present a patient with an atypical presentation of CAD, where coronary computed tomography angiography (CCTA) was essential in identifying an inflammatory cause.
Summary figure
The arterial circumferential thickening is depicted as the area between the red (artery outer wall) and the blue (artery lumen) lines.
Case presentation
A 74-year-old Caucasian patient was admitted for CCTA after experiencing Class II angina according to the Canadian Cardiovascular Society classification for 2 months. The electrocardiogram showed no T waves and ST-segment abnormalities, and the echocardiography results were normal. A positive exercise stress test revealed a down-sloping ST-segment depression concomitant with chest pain. He had no significant past medical history and no cardiovascular risk factors.
Cardiac computed tomography angiography revealed a highly atypical form of CAD, characterized by a diffuse, circumferential thickening with low attenuation of the ascending aorta (Figure 1), the proximal left main coronary artery (LMCA), and Left Anterior Descending (LAD) artery (Figure 2). This arterial thickening resulted in a 50%–70% stenosis of the mid-LAD artery. Given this atypical presentation in a patient without traditional cardiovascular risk factors, an inflammatory cause was suspected. Therefore, we decided to postpone coronary revascularization and referred the patient to a specialized internal medicine unit for further evaluation.
Computed tomography angiography of the ascending aorta and coronary ostia. Cross-sectional views (A and B) showing circumferential thickening of the ascending aorta (white star) extended to left main coronary artery and right coronary artery ostia (arrows) without significant stenosis.
Coronary computed tomography angiography patterns of arteritis. Diffuse and circumferential thickening with low attenuation was observed from the left main ostium to the mid-left anterior descending artery. In the schematic representation, the circumferential thickening is depicted as the area between the red (artery outer wall) and the blue (artery lumen) lines. (A–C) Curved multiplanar reconstruction images obtained by cardiac computed tomography angiography. (D) Cross-sectional coronary image at the level of the yellow line.
Diagnostic assessment
The clinical examination was unremarkable, with no changes in the patient’s general condition and no fever, sweating, headache, jaw claudication, or reduced visual acuity. The laboratory workup revealed no signs of biological inflammation, with neither an elevation in C-reactive protein levels nor an increase in erythrocyte sedimentation rate. A comprehensive immunological and infectious evaluation, including tests for antinuclear antibodies, antineutrophil cytoplasmic antibodies (ANCA), serum immunoglobulin G4 (IgG4), HIV, and syphilis serologies, were normal. Cardiac magnetic resonance imaging (CMR) showed no myocardial inflammation or late enhancement, with an estimated left ventricular ejection fraction of 65%.
To investigate potential involvement of other organs, a fluorodeoxyglucose-positron emission tomography scan (FDG-PET) was performed, revealing signs of large vessel vasculitis with diffuse hypermetabolism of the aortic wall, as well as the supra-aortic, subclavian, coeliac, superior mesenteric, external iliac, femoral, and popliteal arteries suggestive of giant cell arteritis (GCA) (Figure 3A and B). The maximum standardized uptake value (SUVmax) ranged from 4.7 to 6.1. Fluorodeoxyglucose-positron emission tomography scan also detected a heterogeneous hypermetabolic mass in the right kidney, measuring ∼5.5 cm, with an SUVmax of 7.2 (Figure 3C). A temporal artery biopsy showed fibrous endarteritis with no evidence of GCA. Final diagnosis was classified as unlabelled arteritis, closely resembling GCA.
Large vessel arteritis diagnosis using positron emission tomography/computed tomography. Initial fluorodeoxyglucose-positron emission tomography scan maximum intensity projection (A) and fused positron emission tomography/computed tomography coronal views (B, C) revealed diffuse hypermetabolism of large vessels, consistent with vasculitis (arrows). Pathological fluorodeoxyglucose uptake was also observed in a heterogeneous right renal mass (star).
Interventions
The patient was medically treated with aspirin, a high dose of statin, and a beta-blocker. The primary focus was to treat the right kidney mass, considering the hypothesis of paraneoplastic aortitis due to renal cancer. After a complete workup, no metastases were detected. Subsequently, the patient underwent a partial nephrectomy. Pathological examination confirmed a papillary carcinoma with clear margins. Follow-up FDG-PET scans at 2- and 5-months post-surgery showed no improvement in the pan-aortitis. Consequently, glucocorticoids were introduced at a dose of 0.7 mg/kg/day, followed by prednisone 10 mg/day for 1 month, then gradually reduced by 1 mg/month until reaching 5 mg/day.
Follow-up
The chest pain disappeared quickly with corticosteroid therapy and 4 months after the start of treatment, an FDG-PET scan showed regression of the aortic hypermetabolism (Figure 4). Furthermore, a 1-year follow-up CCTA revealed a notable regression of the coronary thickening in the LMCA and proximal part of the LAD artery with maximum stenosis under 50%.
Regression of circumferential thickening of the left main and left anterior descending coronary arteries before (A–C) and after (D–F) glucocorticoids in cardiac computed tomography angiography. Unmarked (B, E) and marked (C, F) cross-sectional images of the left descending coronary artery corresponding to the yellow line level of the curved multiplanar reconstruction (A, D). In the marked images, the circumferential thickening is visualized between the red line (artery outerwall) and blue line (artery lumen). GCT, glucocorticoid.
Discussion
Cardiac manifestations of systemic vasculitis are rarely seen in clinical practice, and coronary involvement is much less common than myocardial or pericardial involvement. Differentiating CA from atherosclerotic coronary disease is challenging, as the clinical presentation can be similar and manifests as typical angina, acute myocardial infarction, ventricular arrhythmias, or cardiac failure.^1^ Although uncommon, CA is associated with poor prognostic outcomes. In a large cohort of 1647 sudden cardiac death cases referred for pathological heart assessment, only 50 patients (3.0%) had non-atherosclerotic coronary pathology, with CA found in 6 (12%) of these cases.^2^
This case emphasizes the growing role of CCTA as a first-line tool in the diagnostic workup of CAD, allowing in our case for the identification of inflammatory patterns.^3^ The diagnosis of CA was suspected by analogy with aortitis, characterized by regular, circumferential wall thickening of more than 2 mm without calcified or non-calcified plaques.^4,5^ Additionally, a lack of traditional cardiovascular risk factors raised suspicion for an alternative aetiology, further supporting the diagnosis of CA. Despite the presence of symptomatic obstructive CAD, we decided not to perform coronary angiography and instead prioritized biological and non-invasive imaging techniques to better evaluate the potential underlying inflammatory process. Of note, although coronary angiography could have been the first-line investigation, it likely would not have provided a definitive diagnosis as it cannot visualize the circumferential thickening characteristic of inflammatory vascular diseases. In case of atypical presentation, the use of endovascular imaging such as intravascular ultrasound (IVUS) is now recommended to provide additional detail, including identification circumferential thickening with low attenuation.^4^
The role of multimodal non-invasive imaging in the diagnosis pathway of CA is increasingly recognized.^1^ In this case, the findings of diffuse coronary wall thickening on CCTA associated with artery wall hypermetabolism on FDG-PET were crucial in distinguishing inflammatory arteritis from atherosclerotic CAD. Although FDG-PET may not always differentiate vasculitis from atherosclerotic disease, it has become a pivotal diagnostic tool for systemic vasculitis, offering high positive and negative predictive values, and is also useful for evaluating treatment effects.^1,6^ Although not performed in this case, CMR can also detect inflammatory processes in both vascular walls and the myocardium.^1^ In similar scenarios, when faced with clinical atypia such as absence of vascular risk factors or unusual anatomical features like circumferential coronary involvement, aortic wall thickening, additional clinical, biological, and metabolic imaging investigations should be considered to avoid overlooking a non-atherosclerotic CA requiring timely and specific management.
The patient described in this case was a 74-year-old Caucasian male presenting with diffuse aortitis, notably involving the coronary arteries, without the evidence of stenoses or aneurysmal dilatation, and in a paraneoplastic context. Several causes of CA have been described, with the most common being Kawasaki disease, Takayasu arteritis, Polyarteritis Nodosa, and GCA.^1^ The description and imaging features of the several diseases that might present similarly are provided in Table 1 for a comprehensive comparative framework. This table summarizes the key characteristics, imaging patterns, and distinguishing features commonly included in the differential diagnosis of CA. In the present case, several factors, including the patient’s gender, age, ethnicity, and the recent onset of aortitis without structural changes, argue against a diagnosis of Takayasu arteritis, which typically affects younger females with typical ostial coronary artery involvement.^7,8^ Similar cases of IgG4-related disease have been described, with diagnosis established by CCTA in most of the cases.^4^ However, IgG4-related disease was also ruled out based on normal serum IgG4 levels and the absence of other clinical manifestations suggestive of this condition, such as lymphadenopathy, or pancreatic, pulmonary, orbitary and neurological involvement. A diagnosis of GCA could not be confirmed as the patient did not present cranio-cephalic symptoms (headaches, scalp tenderness, and jaw claudication), and the temporal artery biopsy showed no histological evidence of GCA. Consequently, the diagnosis was classified as unlabelled arteritis, closely resembling GCA, given the absence of resolution after cancer treatment and the excellent response to corticosteroid therapy.
Management of CA is complex and depends on its aetiology. In our patient, the accurate diagnosis prevented unnecessary revascularization procedures, which could have been associated with poor prognosis, higher risks of restenosis, or graft failure in an inflamed vascular bed.^8,9^ Early imaging guided diagnosis and the control of active inflammation seem to be crucial for improving clinical outcomes. Indeed, treatment with glucocorticoids led to significant improvement in both metabolic and coronary stenosis. At 12 months of follow-up, the patient no longer presented with chest pain or dyspnoea. Revascularization was not performed, as the patient showed regression of coronary thickening and inflammation on imaging, with no clinical manifestations of ischaemia. Moreover, if the diagnosis had not been established using both imaging modalities, the renal cancer could have progressed, preventing an upfront curative surgical intervention, and the aortitis could have advanced, leading to structural changes (aneurysmal dilations and stenosis) with functional sequelae.
Conclusion
The diagnosis and management of CA remain challenging, particularly in differentiating it from atherosclerotic CAD. An atypical presentation of symptomatic obstructive CAD, such as diffuse circumferential coronary thickening and low-attenuation patterns on CCTA, should prompt careful evaluation before proceeding with coronary angiography or revascularization. Integrating PET-FDG findings of active inflammation with clinical and laboratory investigations enables timely diagnosis and targeted treatment. Early recognition and inflammation control are crucial for optimizing clinical outcomes and avoiding unnecessary or potentially harmful revascularization procedures.
Lead author biography
Julien Rosencher is working in the catheterization laboratories and in the cardiovascular imaging laboratories at the Groupe Hospitalier Privé Ambroise Paré—Hartmann, France. Dr Rosencher has a strong interest in clinical education with mentorship in both laboratories. He is also involved in the French Liberal Cardiologist Association (CNCF).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Khanna S, Garikapati K, Goh DSL, Cho K, Lo P, Bhojaraja MV, et al Coronary artery vasculitis: a review of current literature. BMC Cardiovasc Disord 2021;21:7.33407141 10.1186/s 12872-020-01813-6PMC 7788693 · doi ↗ · pubmed ↗
- 2Hill SF, Sheppard MN. Non-atherosclerotic coronary artery disease associated with sudden cardiac death. Heart 2010;96:1119–1125.20511306 10.1136/hrt.2009.185157 · doi ↗ · pubmed ↗
- 3Houssany-Pissot S, Rosencher J, Allouch P, Bensouda C, Pillière R, Cacoub L, et al Screening coronary artery disease with computed tomography angiogram should limit normal invasive coronary angiogram, regardless of pretest probability. Am Heart J 2020;223:113–119.32087878 10.1016/j.ahj.2019.12.023 · doi ↗ · pubmed ↗
- 4Hata S, Ota S, Ino Y, Miyamoto M, Okumoto Y, Kimura K, et al Serial imaging follow-up for immunoglobulin G 4-related coronary arteritis with acute coronary syndrome. JACC Case Rep 2024;29:102561.39484316 10.1016/j.jaccas.2024.102561 PMC 11522725 · doi ↗ · pubmed ↗
- 5Saadoun D, Vautier M, Cacoub P. Medium- and large-vessel vasculitis. Circulation 2021;143:267–282.33464968 10.1161/CIRCULATIONAHA.120.046657 · doi ↗ · pubmed ↗
- 6Bleeker-Rovers CP, Bredie SJH, van der Meer JWM, Corstens FHM, Oyen WJG. F-18-fluorodeoxyglucose positron emission tomography in diagnosis and follow-up of patients with different types of vasculitis. Neth J Med 2003;61:323–329.14708910 · pubmed ↗
- 7Soto ME, Meléndez-Ramírez G, Kimura-Hayama E, Meave-Gonzalez A, Achenbach S, Herrera MC, et al Coronary CT angiography in Takayasu arteritis. JACC Cardiovasc Imaging 2011;4:958–966.21920333 10.1016/j.jcmg.2011.04.019 · doi ↗ · pubmed ↗
- 8Moutzoukis G, Mahrholdt H, Seitz A. Cardiac manifestation of giant cell arteritis as a rare cause of severe coronary triple vessel disease. J Cardiovasc Comput Tomogr 2023;17:e 5–e 6.36192327 10.1016/j.jcct.2022.09.001 · doi ↗ · pubmed ↗