Eclipsed mitral regurgitation and the role of multimodality imaging: a case report
Stavros Kounas, Nektarios Pilatis, Eirini Solomou, Markos Koukos, Maria Aroni

TL;DR
A case report shows how advanced imaging techniques helped diagnose and treat a rare heart condition causing severe mitral regurgitation.
Contribution
Highlights the diagnostic value of multimodality imaging in identifying dynamic ischemia as a cause of eclipsed mitral regurgitation.
Findings
Multimodality imaging revealed ischemia-induced mitral regurgitation undetected by conventional tests.
Percutaneous coronary intervention resolved symptoms, confirming ischemia as the cause.
Stress imaging is crucial for diagnosing dynamic ischemia affecting valvular function.
Abstract
Eclipsed mitral regurgitation (MR) is a rare, reversible condition that leads to transient severe MR and acute heart failure in patients with preserved left ventricular (LV) ejection fraction. Its diagnosis is challenging due to its intermittent presentation, necessitating advanced imaging techniques to reveal the underlying pathology. We present a case of a 74-year-old female with recurrent severe MR associated with a non-obstructive lesion in the proximal left anterior descending (LAD) artery. Multimodality imaging played a pivotal role in diagnosing this condition, as conventional vasodilator stress tests failed to uncover the ischaemic mechanism. Exercise stress echocardiography and myocardial perfusion scintigraphy successfully demonstrated a small ischaemic region affecting the mitral valve apparatus, which triggered severe MR during physical exertion. This dynamic ischaemia,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
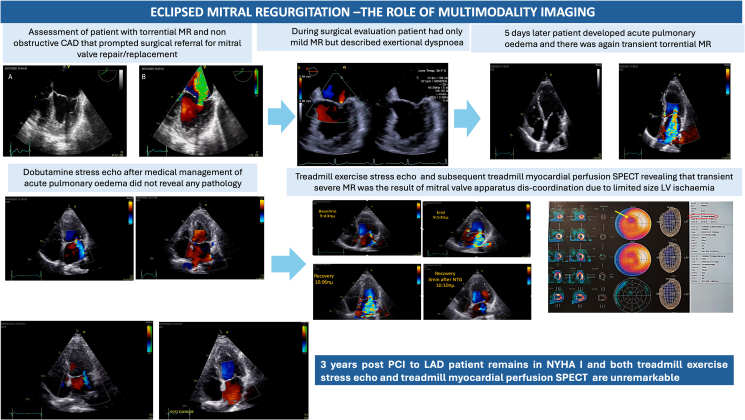 Figure 1
Figure 1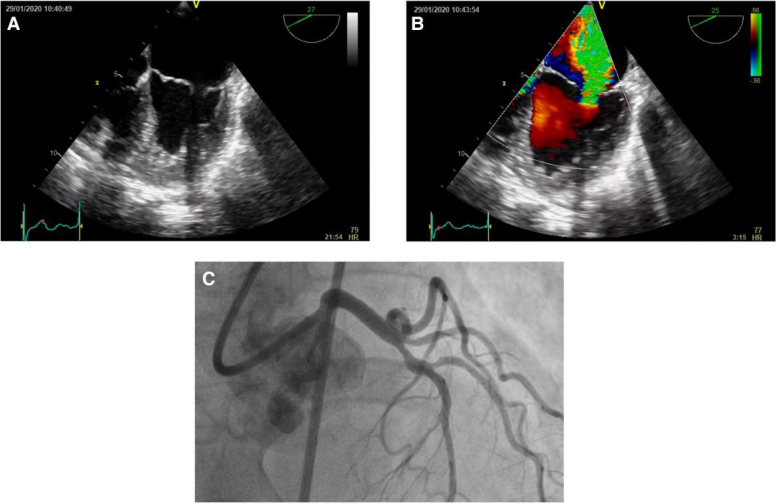 Figure 1
Figure 1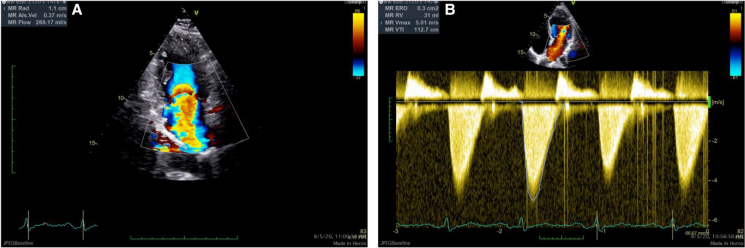 Figure 2
Figure 2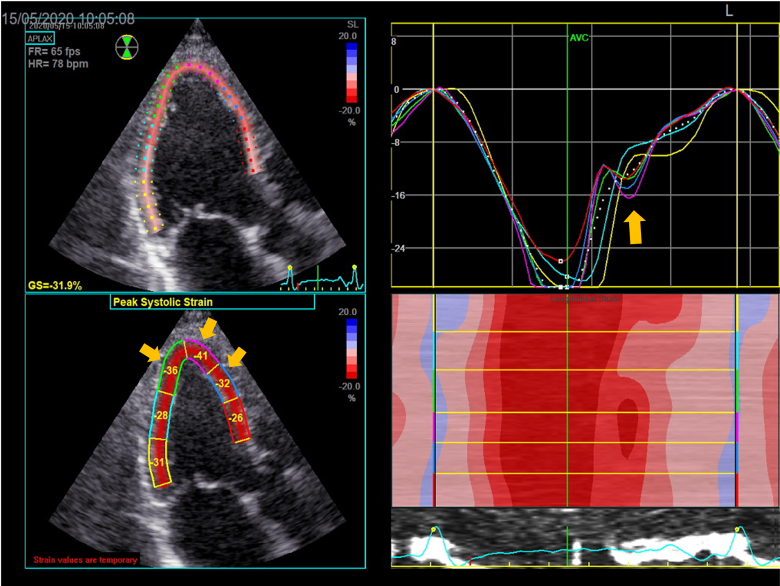 Figure 3
Figure 3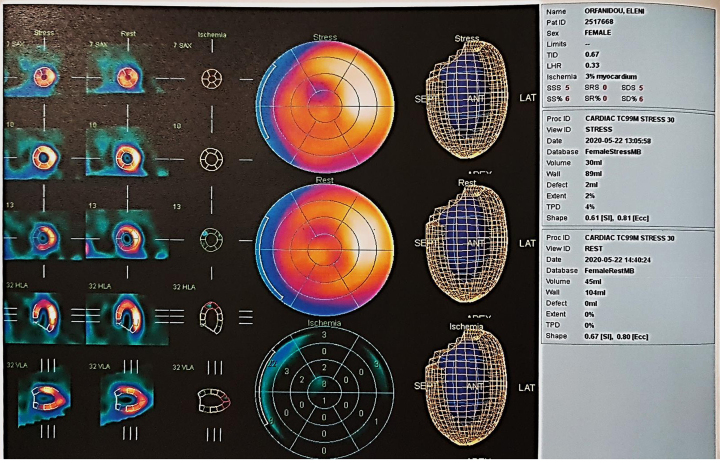 Figure 4
Figure 4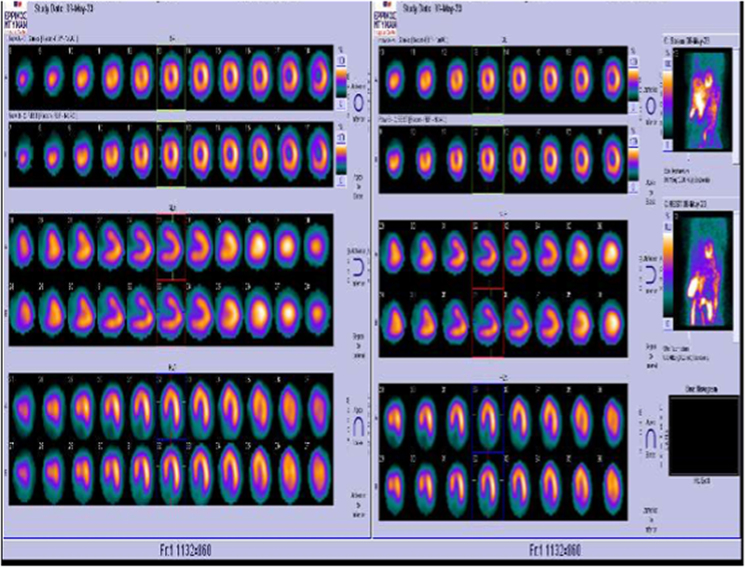 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Cardiac Structural Anomalies and Repair
Introduction
Eclipsed mitral regurgitation (eclipsed MR) is a rare condition characterized by completely reversible severe functional MR, leading to acute heart failure in patients with a normal left ventricular (LV) ejection fraction (EF). The term was first introduced by Avierinos et al. in 2008, who reported three patients with transient, massive functional MR in the absence of pre-existing LV dysfunction or significant coronary artery disease (CAD). The reversible nature of the condition makes it difficult to recognize, and its underlying causes are multifactorial. This is evidenced by the small number of case reports over the years, with patients being diagnosed and managed in different ways—from medical management to surgical valve replacement and transcatheter repair—depending on the underlying pathophysiology.
We present a compelling case of dynamic MR caused by less than 10% ischaemia in a region of the left ventricle due to a non-obstructive lesion in the left anterior descending (LAD) artery, affecting the mitral valve (MV) apparatus. While functional imaging with vasodilatory stress tests failed to reveal the underlying pathology, the use of multimodality imaging, specifically exercise-based tests, successfully identified the subtle ischaemia responsible for the mechanical dysfunction of the MV. This case underscores the importance of multimodality imaging when conventional methods fail to uncover the cause of severe intermittent regurgitation.
Summary figure
**
Case presentation
We revisit the recent medical history of a 74-year-old female patient with a background of primary sclerosing cholangitis, paroxysmal atrial fibrillation, and a history of nephrolithiasis. One year before presenting at our centre, she was admitted to another hospital with a urinary tract infection complicated by acute respiratory failure of unclear aetiology, necessitating intubation. She had a short stay in the intensive care unit and was extubated within 24 h. After discharge, she experienced repeated episodes of transient dyspnoea and chest discomfort, with a concomitant drop in oxygen saturation (SO_2_ < 90%) on pulse oximetry.
A few months later, she was re-admitted to the same hospital due to chest pain and acute pulmonary oedema. Diagnostic workup revealed an unremarkable 12-lead electrocardiogram (ECG) and negative biomarkers for myocardial injury (hs-troponin). However, a transthoracic echocardiogram (TTE) revealed severe functional MR, later confirmed by transoesophageal echocardiogram (TOE) (Figure 1A and B). During that time, the patient was in normal sinus rhythm and her blood pressure remained within normal range. A coronary angiogram showed intermediate proximal LAD stenosis (Figure 1C), which was deemed non-obstructive after fractional flow reserve (FFR) assessment (FFR = 0.86). Consequently, the patient was referred for surgical treatment of MV disease, with the option of a left internal mammary artery graft to the LAD. The patient had received recommendations for MV replacement from two different cardiothoracic centres before seeking a third consultation at our centre.
Initial transoesophageal echo and diagnostic coronary angiogram revealing severe mitral valve regurgitation. (A) 0–30 degrees four-chamber view in end-systole revealing coaptation gap of mitral valve leaflets. (B) Same image with colour revealing severe mitral regurgitation. (C) Diagnostic coronary angiogram right anterior oblique cranial view demonstrating 60–70% disease on proximal left anterior descending artery and 70% on ramus intermedius branch (small vessel).
Pre-operative evaluation was performed at our Heart Valve Center, including a new TTE/TOE, per our practice protocol, to assess the valve anatomy and the mechanism of regurgitation. To our surprise, the assessment revealed only mild MV regurgitation (see Supplementary material online, Videos S1–S5). As a result, an exercise echocardiogram was ordered to evaluate a possible dynamic component. However, 5 days later, the patient presented with symptoms and signs of evolving pulmonary oedema during her scheduled appointment. The new TTE at that time showed massive MV regurgitation with triangular regurgitant jet in continuous wave Doppler (Figure 2), with systolic mitral leaflet restriction, causing a lack of coaptation (see Supplementary material online, Videos S6 and S7), as well as severely elevated systolic pulmonary artery pressure, demonstrated in comparison with her initial assessment (see Supplementary material online, Figure S1). The patient’s chest X-ray is shown in Supplementary material online, Figure S2. It is worth noting that no fluctuations in blood pressure were observed between assessments and that she was always in sinus rhythm and the exact vital signs are documented in the figure legends of each assessment. The patient was admitted for heart failure treatment with intravenous (IV) diuretics.
Recurrence of severe mitral regurgitation with validated quantification in transthoracic echocardiogram. (A) Pisa mitral regurgitation 1.1 cm indicating severe regurgitation. (B) Effective regurgitant orifice area and regurgitant volume measured with continuity method. Note that the triangular shaped envelope of mitral regurgitation indicates acute severe mitral regurgitation and that the effective regurgitant orifice area and regurgitant volume could be underestimated since the continuity equation assumes a more uniform flow.
During admission, after stabilizing the patient, we assessed the coronary flow reserve of the LAD using IV adenosine, which revealed normal findings (see Supplementary material online, Figure S3). We proceeded with a dobutamine stress echocardiogram to check for myocardial ischaemia, which returned negative results, showing no regional wall motion abnormalities at peak stress (>85% of the age-predicted heart rate) (See Supplementary material online, Videos S8–S13). We then followed through with the initial plan for treadmill exercise echocardiography. Pre-exercise TTE showed mild MR (Video 1). The patient managed 4 min of exercise on the treadmill (modified Bruce protocol) before stopping due to dyspnoea and angina. Electrocardiogram recordings at the time were unremarkable (see Supplementary material online, Figure S4). Subsequent TTE revealed torrential MR with minimal improvement after 5 min of recovery (Video 2; see Supplementary material online, Video S14). Despite a blood pressure reading of 110/70 mmHg, sublingual nitroglycerine was administered, leading to an immediate resolution of MR and her symptoms (Video 3). Left ventricular speckle-tracking longitudinal strain analysis showed normal rest and peak EF and global longitudinal strain values, but regional strain curve analysis revealed reversible post-systolic shortening of the mid-apical antero-septal segments, indicating subtle ischaemia over the distal LAD region (Figure 3). To support these findings, a myocardial perfusion single-photon emission computed tomography (SPECT) using a modified Bruce treadmill protocol was performed. The test was again prematurely terminated due to symptoms, but scintigraphy images revealed a 3% area of LV ischaemia in the apical anterior wall (Figure 4).
Left ventricular longitudinal strain at baseline and at peak exercise. Mid-apical antero-septal post-systolic shortening at peak stress compared to baseline is demonstrated with arrows. Strain curves normalized after the administration of sublingual nitrates.
Single-photon emission computed tomography with exercise on treadmill. Three per cent area of ischaemia on the apical anterior wall.
After a short period of treatment with vasodilatory agents (nitrates and diltiazem), during which symptoms remained unchanged, the patient underwent percutaneous coronary intervention (PCI) to the proximal LAD (see Supplementary material online, Videos S15 and S16). Since then, she has remained asymptomatic, in New York Heart Association (NYHA) Class I. Three years after PCI, follow-up exercise echocardiography and exercise SPECT testing showed normal findings (Supplementary material, Videos S17 and S18; Supplementary material online, Figure S5; Figure 5).
Single-photon emission computed tomography with exercise on treadmill post-revascularization.
Discussion
Eclipsed MR is a rare and often under-recognized clinical phenomenon that can lead to recurrent episodes of acute pulmonary oedema in patients with preserved LV EF.^1,2^
This case exemplifies how small, localized areas of myocardial ischaemia can severely disrupt the coordination of the MV apparatus, leading to intermittent MR.^2,3^ The ischaemic insult in such patients may not be widespread, making it difficult to detect using traditional imaging techniques like vasodilatory stress testing or dobutamine echocardiography. As was seen in this case, these methods often miss the nuanced pathophysiology due to their non-physiologic nature. Our findings indicate that transient severe MR can arise due to mechanical discoordination of the MV apparatus caused by subtle ischaemia of the mid-apical anteroseptal segments, preventing proper leaflet coaptation. This was also supported by the reversible post-systolic shortening observed during strain imaging.
The role of coronary vasospasm in exacerbating ischaemia is another critical point highlighted by this case. This phenomenon could explain why certain non-invasive tests failed to replicate the pathophysiological state that produced the severe MR. Vasospasm may not always be induced during routine testing, especially when using pharmacological agents that mimic, but do not fully reproduce, physiological stress.^4^ This insight suggests that vasospasm should be more routinely considered in cases where patients present with symptoms that do not correlate with typical ischaemic findings.
In the context of eclipsed MR, distinguishing between various causes of transient MR is crucial for accurate diagnosis and management. Eclipsed MR is characterized by severe, yet reversible, MR that occurs under specific physiological stress, such as exercise, and resolves at rest, making it challenging to diagnose with conventional methods. Differential diagnosis should consider several key causes of transient MR, including ischaemic MR, functional MR due to LV dysfunction, pappilary muscle dysfunction, and transient increases in left atrial pressure, which may all present with episodic MR. This differentiation is essential, as it directs treatment strategies—whether addressing ischaemic mechanisms, improving haemodynamics, or intervening surgically—towards the underlying cause of transient MR, thereby preventing mismanagement or unnecessary valve interventions.
Exercise-based multimodality imaging proved to be the key diagnostic modality that successfully uncovered the ischaemia responsible for the patient’s recurrent pulmonary oedema and MR.^4^ The use of treadmill exercise stress testing, coupled with echocardiography and myocardial perfusion scintigraphy, allowed us to simulate the physiological conditions under which the patient’s symptoms manifested. These dynamic tests are able to highlight transient ischaemia, which might be missed during resting or pharmacologically induced stress tests.
Moreover, this case underscores the importance of personalized therapy based on individualized diagnostic findings. In the era of precision medicine, identifying the specific mechanisms behind a patient’s disease allows for more targeted interventions.^5^ The use of PCI to address the proximal LAD lesion resulted in complete symptom resolution, which further emphasizes the need for tailored treatment strategies in such complex cases. Not all patients with functional MR require valve replacement or repair; rather, identifying and treating the underlying aetiology can lead to excellent clinical outcomes, as seen in this patient who remained asymptomatic for 3 years post-PCI.^4^
This case raises the possibility that eclipsed MR may be more prevalent than currently recognized. The intermittent nature of the condition and the reliance on non-physiological testing likely contribute to its underdiagnosis.^3,5^ Further research and awareness are needed to refine diagnostic criteria, develop more sensitive testing protocols, and explore whether specific subpopulations may be more susceptible to this condition. The potential role of coronary vasospasm in other forms of dynamic valvular dysfunction also warrants further investigation.
Limitations
This case report has a few limitations. Although coronary vasospasm was not confirmed through a reactivity test or the presence of ST-elevation on the ECG—both of which are typically associated with vasospasm-induced ischaemia—the transient nature of the ischaemia and MR, the discrepancy between exercise and pharmacological stress testing, the absence of significant coronary obstruction, and the rapid response to nitrates strongly suggest that coronary vasospasm was the underlying cause of the acute event.
Additionally, cardiac magnetic resonance imaging (CMRI) was not performed due to the clinical urgency and evolving symptoms, which necessitated prompt diagnosis and treatment using other multimodality imaging techniques. However, CMRI could have offered further insights, particularly in detecting microvascular dysfunction, potentially contributing to a more comprehensive understanding of the ischaemic events.
Conclusion
In conclusion, eclipsed MR represents an important and often overlooked contributor to acute heart failure in patients with preserved EF. This case highlights the utility of exercise-based multimodality imaging in uncovering the underlying ischaemia and emphasizes the importance of individualized treatment approaches. Future studies should aim to refine diagnostic strategies to better identify and manage this elusive but clinically significant condition.
Supplementary Material
ytaf075_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Avierinos JF, Thuny F, Tafanelli L, Renard S, Chalvignac V, Guedj E, et al Eclipsed mitral regurgitation: a new form of functional mitral regurgitation for an unusual cause of heart failure with normal ejection fraction. Cardiology 2008;110:29–34.17934266 10.1159/000109403 · doi ↗ · pubmed ↗
- 2Ichikawa K, Watanabe A, Ito H. Eclipsed mitral regurgitation successfully treated with a combination of surgical and pharmacological therapies: a case report. Eur Heart J Case Rep 2019;3:ytz 039.31449597 10.1093/ehjcr/ytz 039PMC 6601157 · doi ↗ · pubmed ↗
- 3Bourque C, Dijos M, Leroux L, Labrousse L, Metras A, Michaud M, et al Eclipsed functional mitral regurgitation destabilizing hypertrophic cardiomyopathy: an unusual case treated with Mitra Clip. CJC Open 2021;3:680–683.34027373 10.1016/j.cjco.2020.12.010PMC 8134909 · doi ↗ · pubmed ↗
- 4Milleron O, Bouleti C, Mazouz S, Brochet E, Rouzet F, Nataf P, et al Eclipsed mitral regurgitation: an unusual cause of acute heart failure. Eur Heart J Cardiovasc 2017;10:1163–1169.10.1093/ehjci/jew 192PMC 583745027625364 · doi ↗ · pubmed ↗
- 5Kelshiker MA, Seligman H, Howard JP, Rahman H, Foley M, Nowbar AN, et al Coronary flow reserve and cardiovascular outcomes: a systematic review and meta-analysis. Eur Heart J 2022;43:1582–1592.34849697 10.1093/eurheartj/ehab 775PMC 9020988 · doi ↗ · pubmed ↗