Unexpected effects of treating insulin-resistant obese women with high-dose D-chiro-inositol: opening Pandora’s box
Sabrina Basciani, Maurizio Nordio, Maria Letizia Spizzichini, Lucio Gnessi

TL;DR
A study found that a Mediterranean diet improved insulin resistance in obese women, but adding high-dose D-chiro-inositol caused unexpected hormonal issues like increased testosterone and menstrual irregularities.
Contribution
The study reveals the unexpected hormonal side effects of high-dose D-chiro-inositol supplementation in insulin-resistant women.
Findings
Both groups showed improved insulin sensitivity and reduced weight and BMI after 4 months.
The DCI group experienced hyperandrogenism and menstrual irregularities, with increased testosterone and LH levels.
The Mediterranean diet alone provided metabolic benefits without the hormonal side effects seen with DCI.
Abstract
The combination of lifestyle changes and nutraceuticals, such as inositols, can reduce excess weight, leading to a reduction in insulin resistance and a normalization of the metabolic profile. As such, this study investigated the metabolic and hormonal changes observed in women who were overweight/obese with insulin resistance undergoing a hypocaloric Mediterranean diet combined with high-dose D-chiro-inositol (DCI) treatment. In total, 48 insulin-resistant women between 25 and 40 years old, with a body mass index (BMI) between 26 and 32 were divided into two groups: both groups followed a hypocaloric Mediterranean diet for 4 months, and patients in the treated group also underwent treatment with 2400 mg/day of DCI for the same period. We evaluated the homeostasis model assessment (HOMA) index, body weight, BMI, blood glucose, fasting insulin, lipid profile [cholesterol, low-density…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
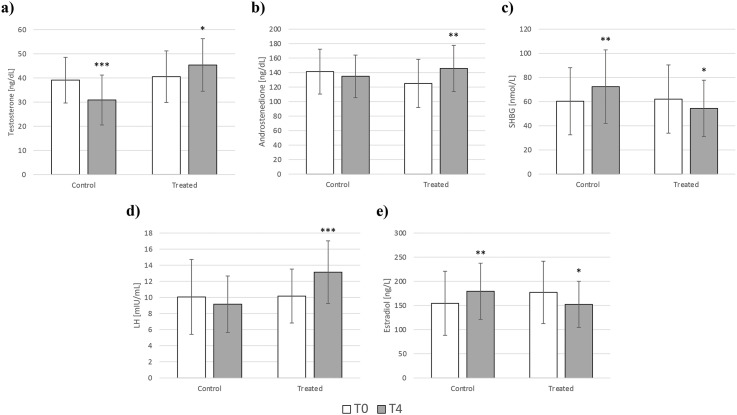 Figure 1
Figure 1| Control group | Treated group | |
|---|---|---|
| Age (years) | 33.5(28.5 – 36.75) | 34.5(29.25 – 37.75) |
| Height (cm) | 159(158 – 161) | 160.5(159 – 164) |
| Body weight (kg) | 70.95(68.68 – 72.55) | 77.10*(71.15 – 80.15) |
| BMI | 28.20(27.35 – 28.68) | 29.55(27.38 – 31.10) |
| HOMA index | 4.65(4.13 – 5.68) | 4.60(3.30 – 5.33) |
| Menstrual length (days) | 34(28 – 35.8) | 28(28 – 29.8) |
| Control group | Treated group | |||
|---|---|---|---|---|
| T0 | T4 | T0 | T4 | |
| HOMA index | 4.65(4.13 – 5.68) | 3.35***(2.93 – 4.33) | 4.60 (3.30 – 5.33) | 3.25***(2.90 – 4.28) |
| Blood glucose (mg/dL) | 111.00(107.25 – 117.00) | 101.00***(98.00 – 110.75) | 106.00(100.00 – 112.00) | 102.50*(96.00 – 106.75) |
| Fasting insulin (mcU/dL) | 17.40(15.58 – 19.50) | 13.45***(11.88 – 16.38) | 17.25(13.83 – 19.73) | 13.00***(11.03 – 16.90) |
| Control group | Treated group | |||
|---|---|---|---|---|
| T0 | T4 | T0 | T4 | |
| Body weight (kg) | 70.95(68.68 – 72.55) | 67.00***(64.58– 71.30) | 77.10(71.15 – 80.15) | 73.40***(68.80 – 77.40) |
| BMI | 28.20(27.35 – 28.68) | 26.40***(25.83 – 27.68) | 29.55(27.38 – 31.10) | 28.20***(26.63 – 29.73) |
| Control group | Treated group | |||
|---|---|---|---|---|
| T0 | T4 | T0 | T4 | |
| Cholesterol (mg/dL) | 203.5(196 – 257.8) | 187.5*(176.25 – 212.75) | 214.5(188.75 – 243.5) | 187.5*(174.25 – 200.75) |
| LDL (mg/dL) | 143(116 – 160.25) | 117.5*(102 – 138.75) | 138.5(98.25 – 164.75) | 119*(92.5 – 142.5) |
| HDL (mg/dL) | 50.5(42 – 57) | 56.5*(49.5 – 63.5) | 48.5(43.25 – 57.75) | 53*(46.75 – 59.75) |
| Triglycerides (mg/dL) | 125.5(114.5 – 175.75) | 115.5*(99.25 – 128.25) | 139.5(106.5 – 76.25) | 120*(99.25 – 132) |
| Control group | Treated group | |||
|---|---|---|---|---|
| T0 | T4 | T0 | T4 | |
| Testosterone (ng/dL) | 40.5(33.25 – 46) | 28***(23.5 – 35.5) | 42(32.75 – 48) | 47.5*(39.5 – 49.75) |
| Androstenedione (ng/dL) | 144.5(108.75 – 165.75) | 131(112.5 – 150.25) | 119(96.5 – 155.5) | 148.5**(118 – 173.75) |
| SHBG (nmol/L) | 58.5(34.75 – 83.25) | 74**(45.75 – 97.5) | 54.5(39.5 – 78.5) | 49*(37.5 – 65.75) |
| FAI | 2.43(1.70 – 3.44) | 1.56**(0.97 – 2.23) | 2.90(1.64 – 4.02) | 3.06***(2.48 – 4.37) |
| LH (mIU/mL) | 9.4(6.08 – 13.77) | 8.65(6.43 – 11.53) | 10(7.55 – 12.58) | 12.95***(10.98 – 15.68) |
| Estradiol (ng/dL) | 151.5(95.5 – 202) | 189.5**(139 – 211.75) | 179(121.75 – 213.5) | 156*(124.75 – 175.75) |
| FSH (mIU/mL) | 8.1(4.92 – 11.4) | 8.05(5.98 – 11.4) | 7.3(5.1 – 9.5) | 8.15(6.1 – 11) |
| DHEAS (µg/dL) | 127(88.5 – 191.5) | 133.5(91.5 – 185.2) | 112.5(93 – 171.5) | 130(103.8 – 181.8) |
| Menstrual length (days) | 34(28 – 35.75) | 28.5*(28 – 32.8) | 28(28 – 29.8) | 32***(30 – 34) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiet and metabolism studies · Diet, Metabolism, and Disease · Liver Disease Diagnosis and Treatment
Introduction
Insulin resistance (IR) is a dysmetabolic condition resulting in a reduced response to insulin from peripheral target tissues. Therefore, tissues require higher concentrations of insulin to achieve a physiological response, leading to compensatory hyperinsulinemia, which is the typical diagnostic hallmark of IR (1).
The direct metabolic consequences of IR include hyperglycemia and obesity, which may lead to inflammation, hypertension, endothelial dysfunction, cardiovascular diseases, metabolic syndrome, non-alcoholic steatosis, and type 2 diabetes mellitus (2–5).
Aside from genetic susceptibility, IR and obesity typically stem from an unhealthy lifestyle, examples of which include a nutritional imbalance with weight gain and an excess buildup of adipose tissue, insufficient physical activity, increased sodium intake, and glucose toxicity and lipotoxicity from excessive circulating free fatty acids (6). In addition, several studies suggest the impairment of gut microbiota, as an environmental factor, may be related to the progression of IR, obesity, and metabolic disturbances (7, 8).
Therefore, lifestyle intervention is crucial for both the treatment and prevention of IR in at-risk patients, as compelling evidence has demonstrated that a moderate and well-tailored weight loss—by as little as 5%–10%—can lead to several health benefits, including a reduction of blood pressure and positive changes in insulin sensitivity and inflammatory biomarkers (9).
In this context, the hypocaloric regimen defined as the Mediterranean diet can improve IR in obese individuals when compared to other dietary approaches, especially in terms of insulin levels, homeostasis model assessment index for IR (HOMA-IR), and inflammation (10–12).
When lifestyle modifications alone are not sufficient to achieve clinically relevant weight loss and metabolic recovery, supplementation with natural compounds may be of great help, accelerating the recovery process and avoiding, or at least postponing, pharmacological interventions and/or surgical approaches.
Among natural molecules with insulin-sensitizing properties, inositols have proven effective in normalizing IR and hyperinsulinemia in dysmetabolic patients, mainly in overweight and obese women, or in women with polycystic ovary syndrome (PCOS) (13–17). D-chiro-inositol (DCI)—the second-most represented isomer of the inositol family—regulates insulin secretion, the mitochondrial respiratory chain, and glycogen storage. The first evidence of the importance of DCI in these processes derives from the observation of a higher DCI content in the body areas deputed to glycogen storage, mainly adipose cells, muscles, and the liver (18). As such, physicians use this molecule to treat insulin dysfunctions in a panel of conditions characterized by metabolic abnormalities (18). Moreover, some studies have suggested that a deficiency of DCI and its high urinary clearance correlate with IR and hyperinsulinemia, leading to the onset of diabetes and metabolic disorders, as observed in patients with PCOS (17, 19–22). There is plenty of clinical evidence on the effectiveness of DCI as an insulin sensitizer, and as a relevant molecule in the field of endocrinology and nutrition (16, 19, 22, 23).
On these premises, the present study aims to evaluate metabolic changes experienced by insulin-resistant overweight/obese women on a hypocaloric Mediterranean diet supplemented with DCI for a period of 4 months.
Materials and methods
Study design and participants
This was an open-label, controlled, interventional study carried out from June to October 2022 at the Section of Medical Pathophysiology, Food Science, and Endocrinology, Department of Experimental Medicine, Sapienza University of Rome. This study was registered on ClinicalTrials.Gov (Identifier: NCT05348941; Approval number: CE6422; Board name: Kemeso) and followed the Good Clinical Practice guidelines and the Declaration of Helsinki. Accordingly, all patients provided written informed consent.
In total, 48 Italian women aged between 25 and 40 years, with a body mass index (BMI) of between 26 and 32 and a diagnosis of IR (HOMA index ≥2.5), were enrolled in our department.
Exclusion criteria included (i) treatment with drugs or supplements that interfere with the mechanism of action of insulin and (ii) pregnancy and breastfeeding.
The sample size was calculated according to previous literature, which demonstrated a decrease in the HOMA index from 5.05 ± 1.51 at baseline to 3.05 ± 0.85 after a 3-month treatment with DCI (23). Setting a power of 90% and a chance of type-1 error equal to 0.05 and considering an adherence rate equal to approximately 50% (24), we obtained a sample size equal to 24 patients per arm, resulting in 48 patients in total.
The 48 enrolled women were divided into two groups based on availability and consent. The treated group (n= 24) received 2400 mg/day of DCI orally in addition to a hypocaloric Mediterranean diet, consisting of fruit, vegetables, olive oil, legumes, cereals, and fish, providing a fixed percentage of carbohydrates, fats (mainly monounsaturated), and proteins (55%, 25%, and 20%, respectively). The patients in the control group (n= 24) followed the same hypocaloric Mediterranean diet in the absence of supplementation. All patients were monitored for 4 months, with the possibility of a second follow-up after 2 more months of treatment.
Measurement
The aim of this study was to evaluate the effects of a 4-month oral supplementation with a high dose of DCI (2400 mg/day) in association with a hypocaloric Mediterranean diet on IR.
DCI dosage was chosen according to the prior work by Nestler (25, 26).
The HOMA index was the primary outcome, while body weight, BMI, blood glucose levels, fasting insulin, lipid profile [cholesterol, low density lipoprotein (LDL), high density lipoprotein (HDL), and triglycerides], and hormonal profile [total testosterone, androstenedione, dehydroepiandrosterone sulfate (DHEAS), sex hormone-binding globulin (SHBG), estradiol, follicle-stimulating hormone (FSH), luteinizing hormone (LH), and menstrual length] represented secondary outcomes. Blood samples from all patients were collected by venipuncture during the follicular phase at baseline and after 4 months of diet and diet + DCI treatment.
After the blood samples were centrifuged at 1,000 × gravitational units (g) for 10 minutes to separate the serum, the serum was stored at − 20°C until assayed.
All the analyses were performed using commercial kits, at Policlinico Umberto I hospital (Rome, Italy). Insulin and glucose levels were assessed using a DPC Immulite 2000 analyzer (Euro/DPC, Llanberis, UK). Cholesterol was measured using an enzymatic cholesterol oxidase/peroxidase method (Beckman Coulter Diagnostics, Brea, CA, USA), and triglycerides were measured using an enzymatic assay (Beckman Coulter Diagnostics, Brea, CA, USA); HDL-cholesterol and LDL-cholesterol tests were performed (Beckman Coulter Diagnostics, Brea, CA, USA). Total testosterone and SHBG were measured using an ECLIA (Electrochemiluminescence immunoassay) kit (Roche Diagnostics, Mannheim, Germany); estradiol was measured using a competitive immunoassay (Access Immunoassay System, Estradiol, Beckman Coulter, Brea, CA, USA). DHEAS was measured using an enzymatic assay (Roche Diagnostics, Mannheim, Germany). Androstenedione was measured using an RIA kit (Beckman Coulter Diagnostics, Brea, CA, USA). FSH and LH were measured using ELISA kits. Free androgen index (FAI) was calculated as [(total testosterone/SHBG) x 100].
Statistical analysis
Data were analyzed via Mann–Whitney U tests (2018 GraphPad Software 8.0.1, La Jolla, CA, USA); values are provided as median (25^th^ percentile – 75^th^ percentile). We considered a p-value of <0.05 to be statistically significant.
Results
General characteristics
All 48 patients completed the study. Baseline parameters and anthropometric measures were not significantly different between the control and treatment groups, as shown in Table 1.
HOMA index, blood glucose levels, fasting insulin
After 4 months, both groups demonstrated a significant improvement in the HOMA index, blood glucose levels, and fasting insulin levels.
In detail, the HOMA index in the treated group significantly decreased from 4.6 (3.3 – 5.33) to 3.25 (2.9 – 4.28), while in the control group, a significant reduction was also observed from 4.65 (4.13 – 5.65) to 3.35 (2.93 – 4.33).
The same pattern was recorded for both blood glucose and fasting insulin, as shown in Table 2. When analyzing the variations from baseline to 4 months between the two groups, no significant differences were found in the HOMA index or in blood glucose and fasting insulin levels.
Body weight and BMI
The 4-month treatment significantly decreased body weight and BMI in both groups, as shown in Table 3. Likewise, after the study period there was no significant difference between the study group and the control.
Lipid profile
The 4-month treatment significantly ameliorated the lipid pattern in both groups, as shown in Table 4. In particular, we observed a significant reduction in cholesterol, LDL, and triglycerides and a significant increase in HDL levels. After the study period, there was no significant difference between the study group and the control.
Hormonal profile
As the normalization of metabolic profile is often associated with an improvement in hormonal patterns and menstrual regularity, we also evaluated total testosterone, androstenedione, DHEAS, SHBG, FAI, estradiol, FSH, LH, and menstrual length as secondary outcomes.
Total testosterone significantly decreased in the control group, while the opposite was observed in the study group. Indeed, the treated group experienced a significant increase in testosterone levels with respect to the baseline value (Figure 1a). Androstenedione remained unchanged in the control group but was also significantly increased in the treated group (Figure 1b).
*Changes in testosterone (a), androstenedione (b), SHBG (c), LH (d), and estradiol (e) in the control (diet alone) and treated (diet + DCI) groups at baseline (T0) and after 4 months (T4). Values are expressed as median (25th percentile – 75th percentile). *p<0.05 vs T0; **p<0.01 vs T0; **p<0.001 vs T0. SHBG, sex hormone-binding globulin; LH, luteinizing hormone.
SHBG was inversely affected when comparing the changes that occurred in the two groups. Indeed, the amount of SHBG significantly increased in the control group, while its levels significantly decreased in the group supplemented with high-dose DCI (Figure 1c).
Consequently, the FAI significantly decreased in the control group from 2.43 (1.70 – 3.44) to 1.56 (0.97 – 2.23) (p<0.01) while it significantly increased in the patients who received the supplementation, from 2.90 (1.64 – 4.02) to 3.06 (2.48 – 4.37) (p<0.01).
LH levels exhibited a contrary pattern to SHBG, increasing in the treated group with no change in the control group (Figure 1d).
Estradiol levels appeared to be higher after 4 months in the control group, increasing from 151.5 ng/L (95.5 – 202) to 189.5 ng/L (139 – 211.8) (p<0.01). In contrast, DCI supplementation contributed to a significant decrease in estradiol levels, from 179 ng/L (121.8 – 213.5) to 156 ng/L (124.8 – 175.8) (p<0.05) (Figure 1e). In both groups, no significant changes were observed for DHEAS and FSH. All the hormonal changes are shown in Table 5.
Menstrual length
In agreement with the hormonal parameters, the menstrual cycle was also greatly affected by high-dose DCI. While the menstrual length in the control group was significantly improved from 34 (28 – 35.8) to 28.5 (28 – 32.8) days, patients who received DCI supplementation experienced a significant increase in menstrual length, from 28 (28 – 29.8) to 32 (30 – 34) days.
Due to these circumstances, namely the significant increase in androgen levels and the extension of menstrual cycle, the authors decided that the study needed to be discontinued for patient safety concerns. Thereby, a second follow-up after 2 further months of treatment, as previously scheduled, was no longer considered.
Discussion
Obesity is a chronic condition that is associated with several metabolic and non-metabolic comorbidities, impacting life quality and expectancy and increasing public health costs worldwide (27–30). Among the drivers of excess weight and related complications, IR stands out as a primary contributing factor (31–33). Indeed, IR and prediabetes are on the increase worldwide, with alarming predictions for the next 15–20 years (34). Clearly, these data underscore the pressing need for lifestyle adjustments to tackle weight gain and associated disorders.
The recommended first-line approach for weight loss relies on adequate physical activity and healthy eating habits (35). In this context, the Mediterranean diet is associated with several benefits in terms of reducing IR, and lowering the risk of developing diabetes, metabolic syndrome, and cardiovascular diseases (36, 37).
Furthermore, nutraceutical interventions are currently employed on a large-scale basis as potential treatments for weight management and insulin sensitivity improvement (38, 39).
Consequently, inositols have attracted much attention, as several studies have confirmed their effectiveness in improving IR and excess weight-associated complications in patients with PCOS, metabolic syndrome, and diabetes (40).
Aside from increasing insulin sensitivity, inositols, and notably DCI, have been proven to be able to correct the imbalance between energy intake and energy output (41), leading to a reduction in oxidative stress (42), inflammation (43), and BMI (16, 44).
As such, this study intended to examine the benefits, in terms of metabolic and hormonal rebalance, of supplementing insulin-resistant overweight/obese women with DCI in combination with a hypocaloric Mediterranean diet.
In agreement with the results of the Nestler research group (25, 26), we opted for a treatment with high-dose DCI (45), as prior data has demonstrated that DCI improves metabolic and reproductive function in certain patients.
Our findings highlight once more that DCI supplementation causes a significant improvement in insulin sensitivity, delineated by a reduction in the HOMA index, along with a decrease in blood glucose and fasting insulin levels across both groups. Moreover, although the BMI was already significantly different at T0, the patients demonstrated significant body weight and BMI reductions in both the diet and DCI-supplemented groups. In contrast, our study, for the first time, questions the usefulness of high doses of this inositol to correct metabolic disturbances and the associated gynecological issues in a population different from healthy volunteers.
In detail, the administration of high-dose DCI resulted in alarming effects on hormonal profiles and menstrual cycle fluctuations. The control group exhibited a decline in total testosterone and androstenedione, likely due to the lowering of insulin levels and insulin-dependent production of ovarian androgens. In contrast, the treatment group experienced a noteworthy increase in the abovementioned androgens. Naturally, the FAI was also increased by treatment with high-dose DCI, whereas it was reduced in the diet-only group in agreement with the evidence in the literature (46). The increase in the FAI signifies that the women treated with high-dose DCI may have progressed toward a more hyperandrogenic phenotype, and this likely accounts for the menstrual irregularities observed in the treated group.
Due to the above-reported metabolic and hormonal concerns in the treatment group, the trial was stopped due to ethical considerations.
We speculate that these results are attributable to the endocrine role of DCI, which participates in steroidogenesis, downmodulating the conversion of androgens to estrogens via the aromatase enzyme. Indeed, as initially demonstrated by Sacchi using in vitro experiments (47) and later confirmed in vivo by Bevilacqua (48), DCI inhibits aromatase gene expression, promoting androgen accumulation at the expense of estrogens. In this regard, the literature agrees that DCI administration should be avoided in hyperandrogenic women with PCOS, who may experience a worsening of their symptoms.
Furthermore, a recent study (49) encouraged a more careful evaluation of doses, timing, and patient features in the case of a treatment with DCI, in order to achieve the desired therapeutic effect without exacerbating pathological conditions, such as PCOS-related hyperandrogenism (18).
Our study is not intended to confirm or explain the molecular mechanism underlying the clinical effects of DCI. Therefore, it is imperative that further research unravels the intricate interplay between DCI, insulin sensitivity, and hormonal regulation. Moreover, the importance of long-term studies cannot be overstated, as they are crucial for evaluating the sustainability of therapeutical effects and their broader clinical implications.
Limitations
Among the limitations of this study, the primary one is the absence of a placebo in the control group, which may introduce potential bias; the relatively small sample size is the second.
Conclusions
Overall, this study emphasizes how proper nutritional habits positively impact insulin sensitivity and excess weight. Undoubtedly, the joint use of combinational approaches may contribute to metabolic recovery; however, our study does not indicate any additional benefits of high-dose D-chiro-inositol supplementation compared to diet alone.
Moreover, our results indicate that it is crucial for clinicians to be aware of all known mechanisms of action of food supplements, in addition to dose- and time-related effects. It is hoped that this study may guide clinicians towards the prescription of tailored therapeutical strategies that address the patients’ individual needs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Johnson JD. On the causal relationships between hyperinsulinaemia, insulin resistance, obesity and dysglycaemia in type 2 diabetes. Diabetologia. (2021) 64:2138–46. doi: 10.1007/s 00125-021-05505-4 34296322 · doi ↗ · pubmed ↗
- 2Deacon CF. Physiology and pharmacology of DPP-4 in glucose homeostasis and the treatment of type 2 diabetes. Front Endocrinol (Lausanne). (2019) 10:80. doi: 10.3389/fendo.2019.00080 30828317 PMC 6384237 · doi ↗ · pubmed ↗
- 3Ginsberg HN. Insulin resistance and cardiovascular disease. J Clin Invest. (2000) 106:453–8. doi: 10.1172/jci 10762 PMC 38025610953019 · doi ↗ · pubmed ↗
- 4Wild S Roglic G Green A Sicree R King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. (2004) 27:1047–53. doi: 10.2337/diacare.27.5.1047 15111519 · doi ↗ · pubmed ↗
- 5Li M Chi X Wang Y Setrerrahmane S Xie W Xu H. Trends in insulin resistance: insights into mechanisms and therapeutic strategy. Signal Transduct Target Ther. (2022) 7:216. doi: 10.1038/s 41392-022-01073-0 35794109 PMC 9259665 · doi ↗ · pubmed ↗
- 6Fahed M Abou Jaoudeh MG Merhi S Mosleh JMB Ghadieh R Al Hayek S. Evaluation of risk factors for insulin resistance: a cross sectional study among employees at a private university in Lebanon. BMC Endocr Disord. (2020) 20:85. doi: 10.1186/s 12902-020-00558-9 32522257 PMC 7288486 · doi ↗ · pubmed ↗
- 7Lippert K Kedenko L Antonielli L Kedenko I Gemeier C Leitner M. Gut microbiota dysbiosis associated with glucose metabolism disorders and the metabolic syndrome in older adults. Benef Microbes. (2017) 8:545–56. doi: 10.3920/bm 2016.0184 28701081 · doi ↗ · pubmed ↗
- 8Baothman OA Zamzami MA Taher I Abubaker J Abu-Farha M. The role of Gut Microbiota in the development of obesity and Diabetes. Lipids Health Dis. (2016) 15:108. doi: 10.1186/s 12944-016-0278-4 27317359 PMC 4912704 · doi ↗ · pubmed ↗