Patent foramen ovale: life-saving, but breath-taking in fulminant pulmonary embolism
Kathrin Reuthner, Thomas Müller, Alexander Dietl

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
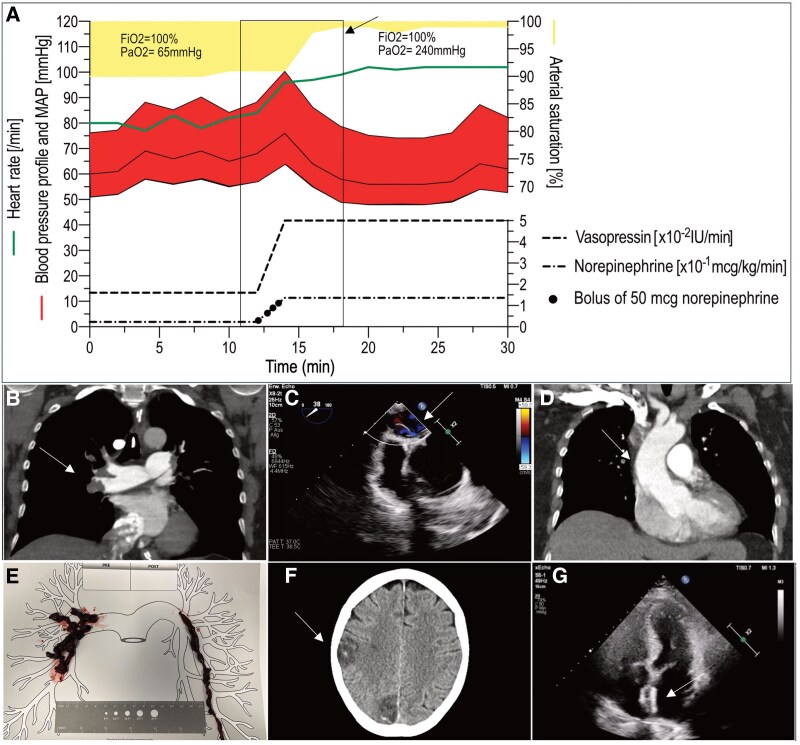 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Traumatic Brain Injury and Neurovascular Disturbances · Radiation Dose and Imaging
Two days after knee surgery, a 61-year-old female patient developed acute dyspnoea followed by hypoxaemic respiratory failure. The patient had no medical history. A week before, she had been able to cycle to work. A CT scan revealed bilateral central pulmonary artery emboli despite the administration of thromboprophylaxis (Panel B). In critical hypoxaemic failure despite non-invasive ventilation (NIV), bronchoscopic intubation was performed in upright position through the oronasal NIV mask. After the upper body was lowered, there was a sudden haemodynamic collapse accompanied by a significant improvement in oxygen saturation (Panel A). With persistent hypoxaemia, a right-to-left atrial shunt was suspected. In line, transthoracic echo revealed a jet on colour Doppler. Transoesophageal echocardiography provided further information on the morphology, showing a patent foramen ovale (PFO) (Panel C). The thin, rather mobile atrial septum was displaced to the left atrium resulting from high right atrial pressure. When pulmonary embolism initially increased pressures in pulmonary circulation, the right-to-left shunt most probably had prevented the right heart from acute failure. Lowering the upper body in the presence of a PFO as well as aortic elongation (Panel D) reduces the right-to-left shunt volume in orthodeoxia syndrome. In our case, reduced right-to-left shunt volume improved oxygenation but unmasked the fulminant obstructive shock. As progressive shock could not be stabilized by conventional therapy, veno-arterial extracorporeal membrane oxygenation (VA-ECMO) was established. Ischaemic stroke within previous six months was a contraindication for systemic fibrinolysis. Due to acute haemodynamic instability, interventional aspiration thrombectomy was performed and removed a large amount of thrombus material (Panel E). After further clinical stabilization, the ECMO could be removed after 5 days. On Day 8, the patient was extubated. Patent foramen ovale was most likely causal for multi-temporal, subacute, and older cerebral ischaemic insults, which were detected by CT (Panel F). After interdisciplinary assessment and shared decision-making with patients’ relatives, early transcatheter closure was performed (Panel G). The coagulation disorder assessment did not reveal thrombophilia. After neurological rehabilitation, the patient was discharged with oral anticoagulation and is now an active part in her family’s daily life again.