A Rare Presentation of Patient With CIDP Found to Have Respiratory Failure and Encephalopathy
Pankti Sheth, Armando Rodriguez Lopez, Shradha Acharya, Bryan Dunn

TL;DR
A rare case of CIDP presented with respiratory failure and encephalopathy, requiring intubation and limited improvement with treatment.
Contribution
This case report highlights an atypical presentation of CIDP with respiratory failure and encephalopathy.
Findings
CIDP presented with respiratory failure requiring intubation and encephalopathy.
Plasma exchange and steroids resulted in minimal clinical improvement.
Prompt diagnosis and treatment are emphasized for such rare CIDP features.
Abstract
Chronic inflammatory demyelinating polyneuropathy (CIDP) is a rare neuropathy that presents with progressive weakness, sensory disturbances, areflexia, and ataxia. Respiratory failure and encephalopathy are rare and atypical presentations in patients with CIDP. In this report, we discuss a rare presentation of respiratory failure that required intubation and encephalopathy in a patient presenting with clinical signs of typical CIDP supported by nerve conduction, neuroimaging, and cerebrospinal fluid studies. Treatment with plasma exchange and steroids led to minimal clinical improvement in this scenario. Prompt diagnosis and treatment is important, and further research is warranted to understand associations between CIDP and such rare features.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
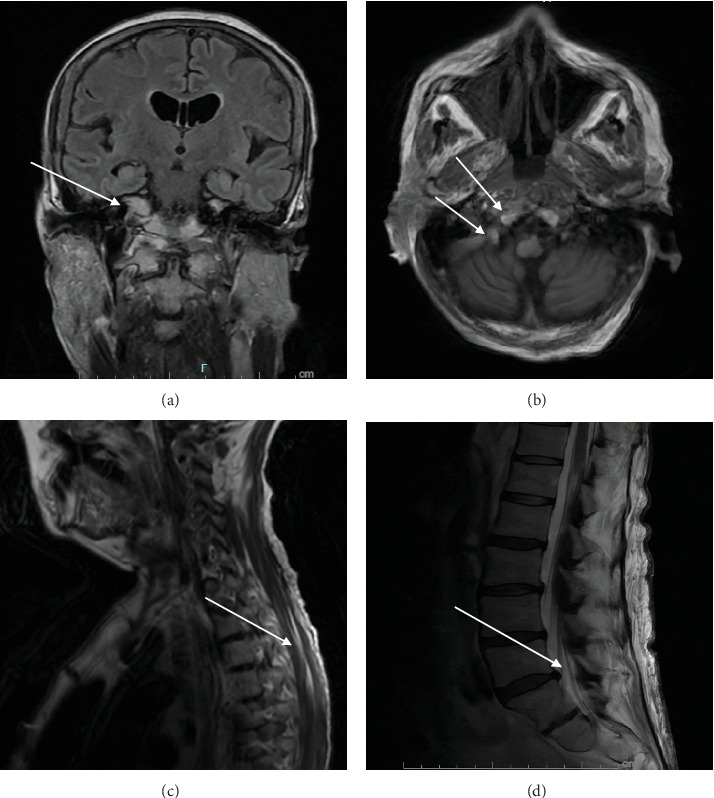 Figure 1
Figure 1- —East Carolina University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Hereditary Neurological Disorders · Amyotrophic Lateral Sclerosis Research
1. Introduction
Chronic inflammatory demyelinating polyneuropathy (CIDP) is an acquired neuropathy that primarily affects the peripheral nervous system. The 2021 European Academy of Neurology/Peripheral Nerve Society (EAN/PNS) guideline describes typical CIDP as having all of the following criteria: progressive or relapsing, symmetric weakness of the proximal and distal muscles of upper and lower limbs, with sensory involvement of at least two limbs which develops over at least 2 months in addition to absent or diminished tendon reflexes in all extremities—sometimes affecting cranial nerves [1]. CIDP variants exist such as focal, multifocal, distal, pure motor, and pure sensory.
The leading theory for pathogenesis of CIDP is cell-mediated and humoral-based immune mechanisms [2]. CIDP is primarily a demyelinating disease with some secondary axonal loss [3].
It is diagnosed using clinical, electrodiagnostic, and other supportive criteria. The electrodiagnostic criteria include abnormalities in motor and sensory conduction suggestive of demyelination. Supportive criteria include clinical improvement after being treated with immunomodulatory agents, ultrasound of median nerve or brachial plexus showing nerve enlargement in at least two sites, magnetic resonance imaging (MRI) showing enhancement or enlargement of nerve roots, cerebrospinal fluid (CSF) with albuminocytological dissociation with elevated CSF protein and leukocyte count < 10/mm^3^, and/or nerve biopsy showing thinly myelinated or demyelinated axons/nodes or perivascular macrophage clusters [1].
We present a patient who met several diagnostic criteria of CIDP who presented with 3 months of progressive weakness in her bilateral lower and upper extremities in addition to numbness and tingling in her hands and feet, severe acute hypoxemic respiratory failure, and acute encephalopathy that required admission to the intensive care unit (ICU). We discuss the rare presentation of this case with supportive evidence and similar presentations through pertinent literature review.
2. Case Presentation
A 58-year-old woman with a history of hypothyroidism, noninsulin-dependent Type 2 diabetes mellitus with diabetic polyneuropathy, colon cancer treated with resection and chemotherapy, thyroid cancer treated with thyroidectomy, chronic hepatitis C virus (HCV), latent syphilis, polysubstance use (cocaine, marijuana, and alcohol), and major depressive disorder with psychotic features presented with 3 months of progressive weakness in her bilateral lower limbs which progressed to her upper limbs making her wheelchair bound. She also experienced gait ataxia, numbness and tingling in her hands and feet, and fecal incontinence around the same time. The family found her unresponsive one morning and brought her to the hospital on July 21, 2024. Notably, on presentation, her blood glucose was low at 38 mg/dL which was corrected with dextrose (D50).
Her physical exam was remarkable for absent motor strength, unresponsiveness to painful stimuli, and absent deep tendon reflexes in the bilateral upper and lower extremities. She did not have a corneal, pupillary, gag, or cough reflex. She required endotracheal intubation and mechanical ventilation for airway protection on the day of her admission. Extensive workup was pursued.
Her lumbar puncture showed CSF remarkable for albuminocytologic dissociation (elevated protein of 132 mg/dL and total nucleated cell count of 0/μL), low glucose of 35 mg/dL, and a negative meningitis/encephalitis CSF panel for Haemophilus influenza, Listeria monocytogenes, Neisseria meningitidis, Streptococcus agalactiae, Streptococcus pneumonia, cytomegalovirus, Herpes Simplex Virus 1 and 2, enterovirus, varicella zoster, and Cryptococcus neoformans.
MRI of the brain showed no acute infarction or intracranial abnormality; however, it showed nonspecific, patchy, low attenuation in the periventricular deep white matter typical of chronic microvascular changes. It also displayed subtle abnormal enhancement along the fifth, seventh, and eighth cranial nerves and along the leptomeningeal margin of the upper cervical cord, and chronic right orbital blowout fracture (Figure 1a,b). MRI of the spine showed subtle abnormal enhancement along the upper cervical cord, lumbar nerve roots, and upper cauda equina (Figure 1c,d). Continuous electroencephalogram (EEG) showed continuous slowing and was negative for seizures.
Electromyography (EMG) nerve conduction study found significantly prolonged motor distal latencies, decreased conduction velocities, decreased amplitude, and prolonged F-wave latency difference which suggested demyelination with axonal loss as seen in CIDP (Tables 1 and 2).
Serum motor neuropathy panel was negative for anti-GQ1b, anti-GD1a, anti-GD1b, anti-GM1, and anti-MAG antibodies; however, it demonstrated elevated IgG (2449 mg/dL) and IgA (509 mg/dL).
She had chronic HCV infection with positive HCV antibody. Her viral load was elevated with HCV RNA of 4 million IU when tested during admission (July, 2024) which was higher than previous levels of 2 million IU in June, 2024 and 833,000 IU in 2020. However, she had normal liver function tests and no signs of decompensated cirrhosis. It was unknown if she received treatment for the infection. Her serum cryoglobulin levels were negative with normal complement C4 levels which suggested her peripheral symptoms were not secondary to cryoglobulinemia in the setting of HCV. There have been case reports that show HCV as a potential trigger of CIDP [4, 5] and HCV-related encephalomyelitis [6]. The patient had a history of latent syphilis which was treated with penicillin G and doxycycline. Her fluorescent treponemal antibody absorption (FTAB) was positive; however, her VDRL was negative with no CSF findings suggestive of neurosyphilis.
The progressive symmetric weakness in the bilateral upper and lower extremities along with areflexia over 3 months, CSF findings of albuminocytologic dissociation, EMG nerve conduction study showing demyelinating neuropathy and axonal loss findings with significantly prolonged motor distal latencies, and MRI findings of leptomeningeal and nerve root enhancement highly support the diagnosis of CIDP.
Patient underwent initial therapy of CIDP with five sessions of plasmapheresis (last session on August 3, 2024). She also received 1 g of intravenous methylprednisolone for 5 days around the same time. While receiving treatment, she showed nonpurposeful movements of the head and left upper and lower extremities. She had a return of cough and gag reflex with an eventual return of corneal and pupillary reflex. She opened both of her eyes and turned her head toward the voice when her name was called and withdrew to painful stimulus elicited on the left upper extremity only. This was a mild improvement compared to her initial presentation. Unfortunately, she did not show any other meaningful clinical improvement and remained intubated during her stay in the ICU.
3. Discussion
The diagnosis of CIDP should be considered when a patient presents with progressive, symmetric weakness of the proximal and distal muscles, sensory disturbances, areflexia, and gait ataxia over a course of two or more months as seen in the case presented. AIDP (acute inflammatory demyelinating polyneuropathy) presents with similar clinical features; however, one of the required criteria states that the nadir must be reached within < 4 weeks from symptom onset [7]. In this case, the patient's symptoms kept worsening over the course of 3 months which is not consistent with the diagnosis of AIDP.
Diagnosis of CIDP can be made using clinical, electrodiagnostic, and other supportive criteria that has been aforementioned. The initial therapy for CIDP includes intravenous immune globulin (IVIG), plasma exchange, or glucocorticoids. About 66% of patients with CIDP initially respond to therapy while 10%–15% of patients are resistant to all therapies [8]. In this case report, the patient showed minimal improvement after being treated with five sessions of plasma exchange and steroids.
The specific triggers remain unclear but prior research has shown association of CIDP with hepatitis B or C, human immunodeficiency virus, systemic lupus erythematosus, thyroid disorders, diabetes mellitus, nephrotic syndrome, and inflammatory bowel disease [1, 4, 5, 9].
Although respiratory failure is not a typical clinical feature in CIDP, there are case reports of patients with CIDP who had respiratory failure that required admission to ICU with some requiring intubation [10]. Another case report explored four patients with CIDP who had respiratory failure secondary to diaphragmatic paralysis in the setting of phrenic nerve palsy with two requiring ventilatory support [11]. Of note, not all patients responded to treatments. Studies have shown that patients with CIDP who develop respiratory failure tend to have phrenic nerve involvement and diaphragmatic paralysis [11, 12]. Phrenic nerve conduction studies have been shown to have increased response latencies, EMG can confirm loss of motor units in diaphragm, and postmortem findings have shown axonal loss in the phrenic nerve [12–14]. The patient in this case was not subjected to phrenic nerve conductions studies or EMG of the diaphragm.
Central nervous system (CNS) involvement in CIDP has been reported in a few prior studies [15–17]. HCV-related acute encephalopathy could also have contributed to the patient's altered consciousness as well as initial low glucose and oxygen levels [6]. However, hypoglycemic encephalopathy and hypoxic encephalopathy usually present with focal or diffuse lesions on MRI of the brain [18, 19] which were not found in this case presentation.
Given her respiratory failure requiring mechanical ventilation and encephalopathy, Bickerstaff's brainstem encephalitis (BBE), a Miller–Fisher variant of Guillain–Barré syndrome was considered; however, the patient's presentation with areflexia and absent anti-GQ1B antibodies argued against that diagnosis [20]. MRI findings of high-intensity areas on T_2_-weighted images of the brainstem, thalamus, cerebellum, and cerebrum may be seen in BBE [20] whereas patients with Miller–Fisher syndrome may present with enhancement of oculomotor, abducens, and facial nerves bilaterally with no brainstem abnormalities on the MRI [21]. These imaging findings were not appreciated in the MRI scans of the patient presented in this case report further making BBE and Miller–Fisher as the less likely diagnoses.
The patient meets the clinical, electrodiagnostic, and supportive (CSF and MRI findings) criteria based on the 2021 EAN/PNS guidelines which strongly supports the diagnosis of CIDP [1]. CIDP primarily affects the peripheral nervous system; however, few studies have shown concomitant presence of respiratory failure and CNS involvement. In this case presentation, the patient has multiple comorbidities. We state the potential etiologies of the respiratory failure and encephalopathy and explain the reasoning behind the most and least likely etiologies. CIDP develops over at least 8 weeks as seen in this patient. She eventually develops respiratory failure and encephalopathy. We provide evidence that helps exclude other pathologies that could be responsible for such atypical symptoms. Further investigation is warranted to explore cases of CIDP with this atypical involvement and examine treatment options, response, and prognosis.
4. Conclusion
Progressive weakness of proximal and distal muscles, sensory involvement, areflexia, and gait ataxia over a course of eight or more weeks should prompt investigation of CIDP. The diagnosis can be supported by characteristic EMG nerve conduction findings, neuroimaging, lumbar puncture findings, and nerve biopsy. In rare cases, patients with CIDP are found to have concomitant presence of respiratory failure and CNS involvement. Early recognition and management are important while further investigation is needed to identify prevalence as well as efficacious therapies for such rare variants.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Van den Bergh P. Doorn P. Hadden R. European Academy of Neurology/Peripheral Nerve Society Guideline on Diagnosis and Treatment of Chronic Inflammatory Demyelinating Polyradiculoneuropathy: Report of a Joint Task Force–Second Revision European Journal of Neurology 202126324226810.1111/jns.1245534085743 · doi ↗ · pubmed ↗
- 2Mathey E. Park S. Hughes R. Chronic Inflammatory Demyelinating Polyradiculoneuropathy: From Pathology to Phenotype Journal of Neurology, Neurosurgery & Psychiatry 201586997398510.1136/jnnp-2014-3096972-s 2.0-8494065877625677463 PMC 4552934 · doi ↗ · pubmed ↗
- 3Harbo T. Anderson H. Jakobsen J. Length-Dependent Weakness and Electrophysiological Signs of Secondary Axonal Loss in Chronic Inflammatory Demyelinating Polyradiculoneuropathy Muscle & Nerve 20083821036104510.1002/mus.210002-s 2.0-4944909004218642356 · doi ↗ · pubmed ↗
- 4Corcia P. Barbereau D. Guennoc A. Toffol B. Bacq Y. Improvement of a CIDP Associated With Hepatitis C Virus Infection Using Antiviral Therapy Neurology 200463117918010.1212/01.WNL.0000131899.33969.E 52-s 2.0-324266249015249636 · doi ↗ · pubmed ↗
- 5Ersoz G. Tekin F. Bademkiran F. Chronic Inflammatory Demyelinating Polyneuropathy in an HCV-Related Cirrhotic Patient With Acute Hepatitis B Superinfection European Journal of Internal Medicine 2007183 p. 25710.1016/j.ejim.2006.09.0212-s 2.0-3424714017317449405 · doi ↗ · pubmed ↗
- 6Monaco S. Ferrari S. Gajofatto A. Zanusso G. Mariotto S. HCV-Related Nervous System Disorders Journal of Immunology Research 201220121923614810.1155/2012/2361482-s 2.0-84864944747 PMC 341408922899946 · doi ↗ · pubmed ↗
- 7Doorn P. Van den Bergh P. Hadden R. European Academy of Neurology/Peripheral Nerve Society Guideline on Diagnosis and Treatment of Guillain-Barré Syndrome European Journal of Neurology 202330123646367410.1111/ene.1607337814552 · doi ↗ · pubmed ↗
- 8Gorson K. Schaik I. Merkies I. Chronic Inflammatory Demyelinating Polyneuropathy Disease Activity Status: Recommendations for Clinical Research Standards and Use in Clinical Practice Journal of the Peripheral Nervous System 201015432633310.1111/j.1529-8027.2010.00284.x 2-s 2.0-7865083897121199104 · doi ↗ · pubmed ↗