Microendoscope-Assisted Posterior Decompression Technique Using a 12-mm Tubular Retractor of the SYNCHA Novel Microendoscopic System for Cervical Spondylotic Radiculopathy: A Technical Note
Motohiro Okada, Munehito Yoshida, Kazunori Nomura, Ken-ichi Yawatari, Sae Okada

TL;DR
This paper introduces a new minimally invasive surgical technique using a 12-mm tubular retractor with the SYNCHA system to treat cervical spondylotic radiculopathy.
Contribution
The novel contribution is the application of the SYNCHA system's 12-mm tubular retractor for posterior decompression in cervical spondylotic radiculopathy.
Findings
The 12-mm tubular retractor provided a consistent field of view comparable to the 16-mm retractor.
Adequate decompression was achieved despite the limited working space of the 12-mm retractor.
The technique is safe, minimally invasive, and potentially advantageous over other endoscopic spinal surgeries.
Abstract
The microendoscope-assisted posterior decompression technique for degenerative spinal disorders has gained popularity as a useful minimally invasive spinal surgery in Japan. We performed the technique in >9,000 cases of intervertebral lumbar disc herniation, lumbar spinal canal stenosis, cervical spondylotic myelopathy, and cervical spondylotic radiculopathy (CSR). We primarily used the METRx microendoscopic system (Medtronic Sofamor Danek, Minneapolis, MN) with a 16-mm tubular retractor. The SYNCHA (Teijin Nakashima Medical, Okayama, Japan) is a novel microendoscopic system developed by Yoshida. The features of this system include (1) a ball-link mechanism enabling joystick action and (2) tubular retractors ranging from 12 to 18 mm in diameter with lineup at 2 mm intervals. We are currently performing posterior decompression surgeries using a 12-mm tubular retractor that enables…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2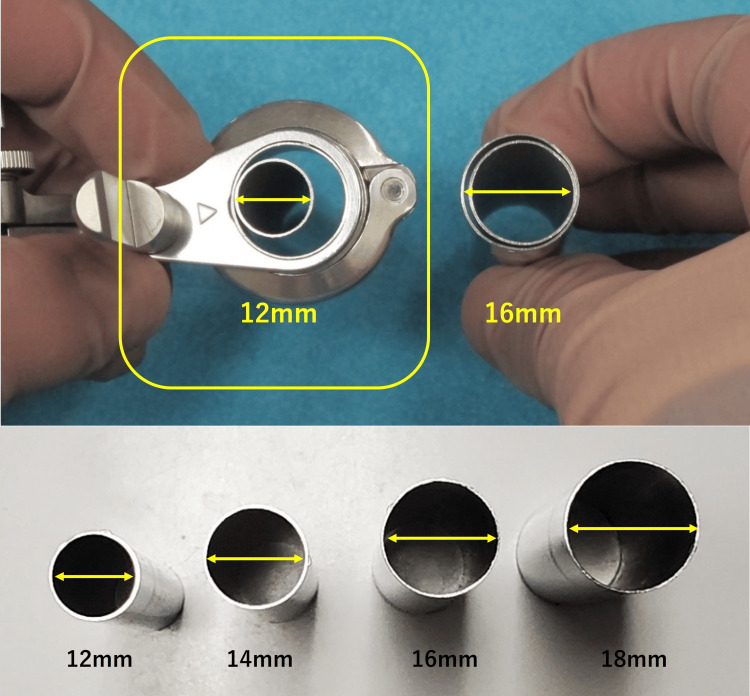 Figure 3
Figure 3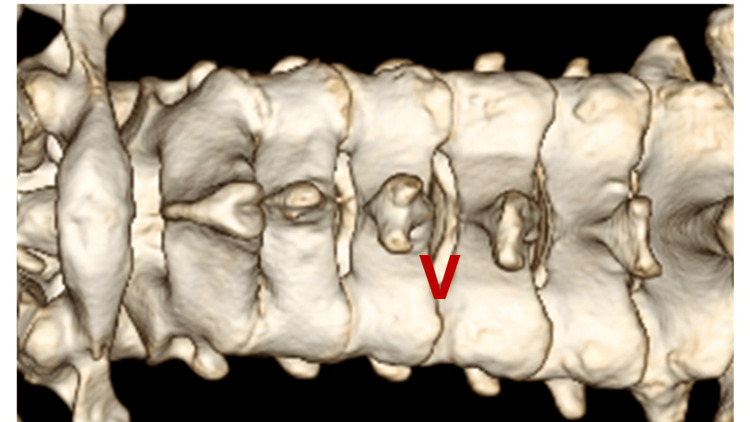 Figure 4
Figure 4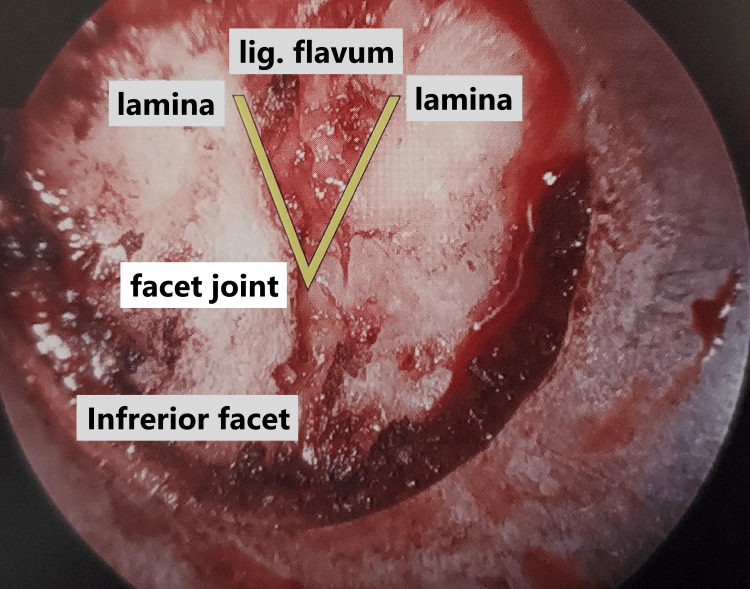 Figure 5
Figure 5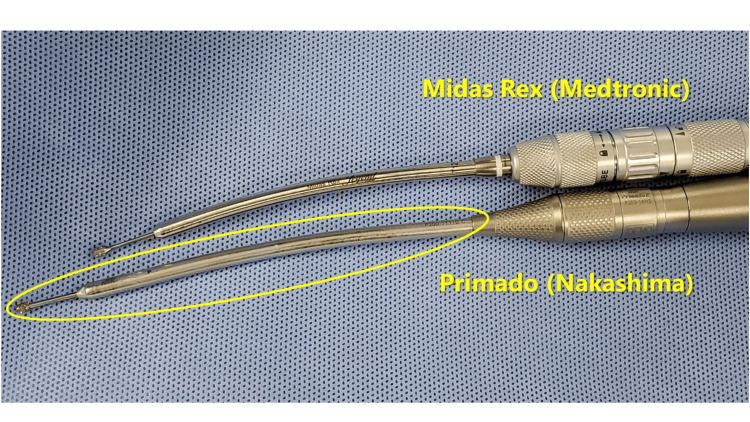 Figure 6
Figure 6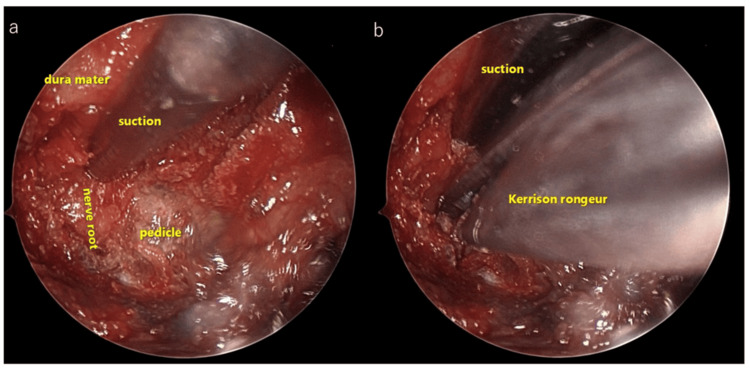 Figure 7
Figure 7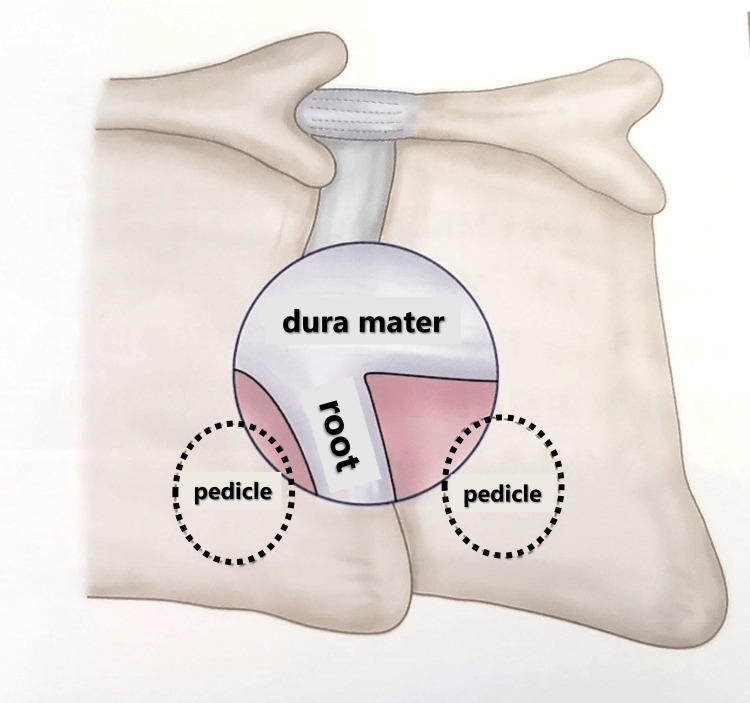 Figure 8
Figure 8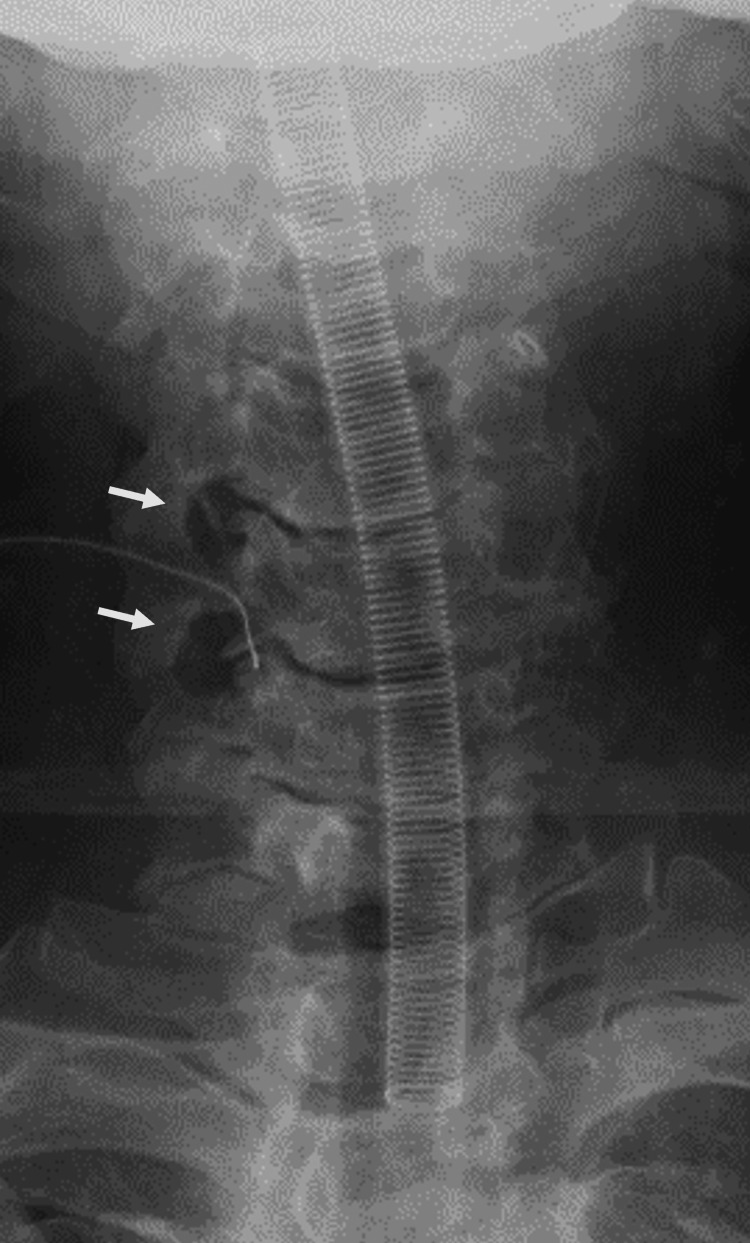 Figure 9
Figure 9 Figure 10
Figure 10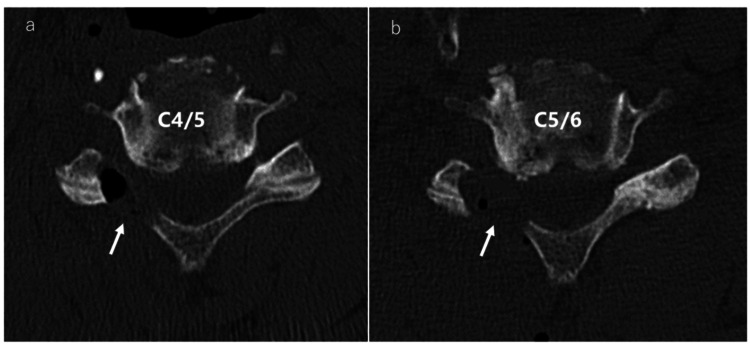 Figure 11
Figure 11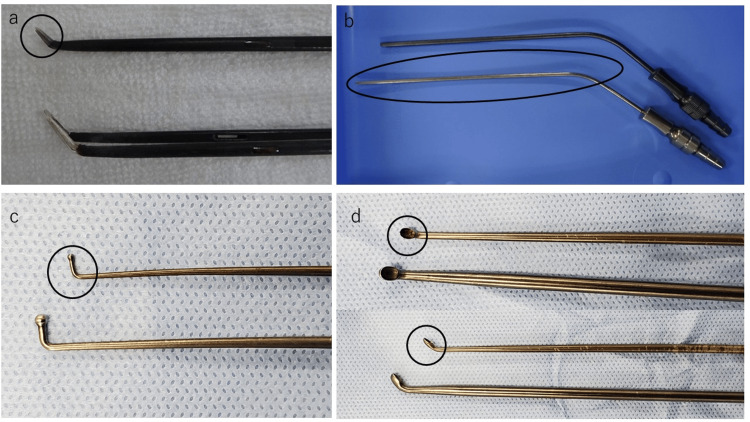 Figure 12
Figure 12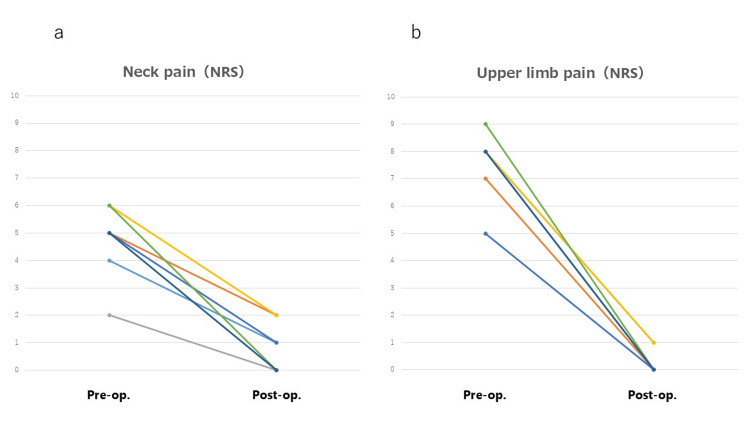 Figure 13
Figure 13| Disease | No. | Age, years | Sex | Level | Follow-up period (months) | Preop. NRS of neck pain | Postop. NRS of neck pain | Preop. NRS of arm pain | Postop. NRS of arm pain | Operating time (mins) | Blood loss (mL) |
| CSR | 1 | 46 | M | C5/6 | 12 | 4 | 1 | 8 | 1 | 90 | 16 |
| 2 | 56 | M | C4/5 | 6 | 5 | 2 | 7 | 0 | 84 | 14 | |
| 3 | 51 | M | C5/6 | 12 | 2 | 0 | 8 | 0 | 78 | 10 | |
| 4 | 59 | F | C5/6 | 12 | 6 | 2 | 8 | 1 | 81 | 16 | |
| 5 | 41 | M | C5/6/7 | 6 | 5 | 1 | 5 | 0 | 132 | 12 | |
| 6 | 44 | F | C4/5 | 6 | 6 | 0 | 9 | 0 | 84 | 3 | |
| 7 | 65 | M | C4/5/6 | 6 | 5 | 0 | 8 | 0 | 158 | 21 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Cervical and Thoracic Myelopathy · Spinal Fractures and Fixation Techniques
Introduction
In recent years, the number of elderly patients with degenerative cervical and lumbar disorders has been on the rise with the increase in the average life span. Conventional spinal posterior decompression techniques were associated with large skin incisions and damage to posterior supportive tissues including muscles, ligaments, facet joints, and capsules, carrying the risk of chronic neck or low back pain and spinal instability. Microendoscopic discectomy (MED) was developed as a minimally invasive surgical technique for the treatment of intervertebral lumbar disc herniation (LDH) by Smith and Foley in 1997 [1]. The microendoscope-assisted posterior decompression technique for treating degenerative spinal disorders has been gaining popularity as a useful, minimally invasive spinal surgery in Japan since Yoshida reported the first case of LDH in the country in 1998 [2]. We have treated >9,000 cases of LDH, lumbar spinal canal stenosis, cervical spondylotic myelopathy, and cervical spondylotic radiculopathy (CSR). Most patients with CSR receive conservative treatment to relieve their symptoms such as neck and upper limb pain. However, upon failure of conservative treatment or in cases of progressive or severe neurological deficit, surgical treatment is recommended.
The main advantage of the microendoscope-assisted posterior decompression technique is that the surgical field is magnified and illuminated, allowing not only minimally invasive techniques but also enabling the procedure to be performed safely and accurately. Furthermore, microendoscopic surgery has the advantage of minimizing damage to the posterior supportive tissues, which also contributes to spinal stability. We have primarily used the METRx microendoscopic system (Medtronic Sofamor Danek, Minneapolis, MN) with a 16-mm tubular retractor [2]. The SYNCHA (Teijin Nakashima Medical, Okayama, Japan) instrument is a novel microendoscopic system developed by Yoshida in 2020. The features of this system include (1) a ball-link mechanism enabling joystick action and (2) tubular retractors ranging from 12 to 18 mm in diameter with a lineup at 2 mm intervals. We are currently treating CSR cases with posterior decompression surgery using a 12-mm tubular retractor to ensure minimal invasiveness.
In this report, we describe the surgical procedure using a 12-mm tubular retractor for treating seven cases of CSR and evaluate their preliminary clinical outcomes, feasibility, and safety; we also compare it with the conventional 16-mm tubular retractor and discuss the advantages of the procedure over other microendoscopic techniques such as full-endoscopic spinal surgery (FESS) and biportal endoscopic spinal surgery (BESS).
Technical report
Figures 1-3 illustrate the SYNCHA endoscopic system and its various elements.
Aspects of SYNCHA (Teijin Nakashima Medical, Okayama, Japan) endoscopic system
Ball-link mechanism enabling joystick action in the SYNCHA system
Lineup of the tubular retractors of the SYNCHA system
Surgical procedures for CSR employed a 12-mm tubular retractor and were conducted according to the methods using a 16-mm tubular retractor as described previously by Adamson [3].
The procedure was as follows:
The patient's head was secured in a Mayfield head holder and placed in a prone position under general endotracheal anesthesia. The neck was secured in a neutral position. The fluoroscopic C-arm was carried to the surgical site, and we marked the target level with a pen under lateral fluoroscopic guidance. The operator stood on the symptomatic side and a video monitor was located on the opposite side of the patient. An approximately 13-mm paramedian skin incision was created above the spinous process. After performing a paramedian fasciotomy on the side of the approach, the paravertebral muscles were split with serial dilators of the SYNCHA microendoscopic system. A 12-mm tubular retractor was passed over the dilators and fixed to a flexible arm mounted on the table-side rail, and an oblique-viewing microendoscope was attached to the tubular retractor. Lateral fluoroscopy confirmed the precise localization of the tubular retractor after resection of the residual musculature and soft tissues on the lamina and facet joint. The following procedures were performed microendoscopically. With the overlap of the superior and inferior articular processes, the so-called interlaminar V (Figures 4, 5) was optically visualized. A high-speed drill with a long curved endoscopic bar (Primado 2, Nakanishi, Kanuma, Tochigi, Japan; Figure 6) was used to cut the inferior articular process while performing the joystick action of the 12-mm tubular retractor repeatedly until the superior articular process was exposed.
Preoperative 3D-CT imageThe overlap of the superior and inferior articular processes enabled the visualization of the so-called Interlaminar VCT: computed tomography
Intraoperative findings of the interlaminar V
Long-curved endoscopic bar
Subsequently, the superior articular process was cut approximately 7-10 mm outward from the medial edge to achieve decompression beyond the Luschka joint (also known as the uncovertebral joint) (Figures 7-11) using a long-curved high-speed drill and curved Kerrison rongeurs. The extent of bone resection should be measured using preoperative CT. The cranial and caudal pedicles are considered the endpoints of cranial-caudal decompression of the nerve root. When significant bleeding from the internal venous plexus was anticipated after posterior bony decompression, we avoided the removal of perineural membranes. After ensuring that the nerve root was adequately decompressed, hemostasis and irrigation were completed, a drain was placed, and the fascia and the skin were closed in layers with 2-0 Vicryl (Johnson & Johnson, New Brunswick, NJ) and Steristrips (3M Company, Maplewood, MN).
Intraoperative findings in the 12-mm tubular retractor of SYNCHA endoscopic systema: Intraoperative findings of dura mater, nerve root and pedicle in the 12-mm tubular retractor. b: The SYNCHA endoscopic system allows the use of both hands
Schematic of posterior decompression for cervical spondylotic radiculopathy (CSR)
Postoperative anterior-posterior X-rayPosterior decompression is achieved beyond the Luschka joint. The arrows show the decompression sites
Postoperative 3D-CT imagePosterior decompression is achieved beyond the Luschka joint. The arrows show the decompression sitesCT: computed tomography
Postoperative CT axial imagesPosterior decompression is achieved beyond the Luschka joint. The arrows show the decompression sitesa: Postoperative CT axial image at C4/5. b: Postoperative CT axial image at C5/6CT: computed tomography
We used a Fine Instrument (Tanaka Medical, Tokyo, Japan; Figure 12) that employed a 12-mm tubular retractor designed to enable fine procedures within a limited working space.
Details of the Fine Instrument (Tanaka Medical, Tokyo, Japan)a: Curved bipolar coagulator. b: Long suction instrument. c: Ball-tipped probe. d: Curette
Discussion
This is the first report in the literature to describe applying the 12-mm tubular retractor of SYNCHA microendoscopic system for the treatment of CSR. We conducted the surgical procedure for seven cases (nine levels) of CSR between January 2022 and December 2023. Patient demographics and clinical outcomes are presented in Table 1. The follow-up period was at least six months. Clinical records were retrospectively analyzed. We evaluated the following parameters: (1) the numerical rating scale (NRS) for neck and upper limb pain before surgery and at the final follow-up; (2) operating time per single level; (3) intraoperative blood loss per single level; and (4) perioperative complications.
The NRS scores for neck and upper limb pain were found to be improved at the final follow-up in all CSR cases (Table 1, Figure 13). The mean NRS scores for neck pain were 4.7 and 0.9 points before surgery and at the final follow-up, respectively (Figure 13a). The mean NRS scores for upper limb pain were 7.5 and 0.3 points before surgery and at the final follow-up, respectively (Figure 13b). The mean operating time and intraoperative blood loss per single level were 78.6 minutes and 10.2 mL, respectively (Table 1). No dural tear or CSF leakage occurred in any of the cases. No other perioperative complications including neurological deterioration were observed.
NRS scores for neck and upper limb painThe scores were found to be improved at the final follow-up in all CSR casesa: NRS scores for neck pain. b: NRS scores for upper limb painCSR: cervical spondylotic radiculopathy; NRS: numerical rating scale
We have previously reported the usefulness and minimal invasiveness of decompression surgery using the METRx microendoscopic system with the 16-mm tubular retractor [2,4]. In this study, we used the 12-mm tubular retractor of the SYNCHA microendoscopic system for more minimal invasiveness instead of the 16-mm tubular retractor to perform posterior decompression surgery for the treatment of CSR. The SYNCHA novel microendoscopic system was developed by Yoshida in 2020. Thanks to its joystick action, the 12-mm tubular retractor provided a consistently equivalent field of view compared to the 16-mm tubular retractor. Despite the limited working space, it was possible to perform adequate decompression by using the 12-mm tubular retractor. Although decompression surgery using a 12-mm tubular retractor appeared to take longer operating time compared with the 16-mm tubular retractor, we considered surgeries using a 12-mm tubular retractor to be more minimally invasive techniques because these could be performed with a smaller skin incision and the intraoperative blood loss was comparable to a 16-mm tubular retractor. Furthermore, satisfactory clinical outcomes were obtained while employing a 12-mm tubular retractor.
Additionally, we highlight that using the 12-mm tubular retractor has the following advantages over FESS [5-7] and BESS [8-10]: (1) The 12-mm tubular retractor of the SYNCHA microendoscopic system is fixed to the table-side rail, allowing the use of both hands, whereas in FESS and BESS, one hand must hold a microendoscope, and decompression procedures, including dissection of the fibrous adhesions around the dura mater and nerve roots, can only be performed with the other.
(2) The 12-mm tubular retractor of the SYNCHA microendoscopic system does not require continuous irrigation with normal saline, and hence there is no concern regarding elevated cerebrospinal fluid pressure.
(3) The SYNCHA microendoscopic system can be applied to cervical and thoracic myelopathy.
(4) The SYNCHA microendoscopic system can be also applied through the transforaminal approach at the L5/S level, whereas in FESS, the iliac bone interferes, making it difficult to insert the microendoscope.
(5) Minor dural tears can be easily detected and repaired using the SYNCHA microendoscopic system.
(6) The ability to use both hands allows the surgeon to secure the surgical field while suctioning blood and using bipolar forceps, and manage sudden massive bleeding from the venous plexus in the 12-mm tubular retractor of the SYNCHA microendoscopic system.
(7) Because irrigation with normal saline is not required in the 12-mm tubular retractor of the SYNCHA microendoscopic system, placement of hemostatic agents, such as topical gelatin-thrombin matrix sealant, is possible.
(8) The SYNCHA microendoscopic system allows multilevel spinal surgeries and tandem operations.
When using a 12-mm tubular retractor, we encountered no perioperative complications such as a dural tear, CSF leakage, or neurological deterioration. In case of an intraoperative dural tear, it is possible to perform dural suturing microendoscopically through a 16-mm tubular retractor. However, it is currently unclear whether dural suturing can be performed through a 12-mm tubular retractor. We believe that the patch technique alone, with Vicryl mesh (Ethicon, Raritan, NJ) and fibrin glue [11] may be possible within a 12-mm tubular retractor.
The limitations of this technical note are as follows: (1) the small sample size; (2) the short follow-up period; (3) the outcome measure is limited to neck and upper limb pain, with no use of other standard scores; and (4) there is no direct comparison with the 16-mm tubular retractor, FESS, and BESS.
Conclusions
We are currently treating CSR cases by performing posterior decompression surgery using a 12-mm tubular retractor of the SYNCHA novel microendoscopic system. Although this study had a small sample size as it is just a technical note, we believe that our preliminary data show that the microendoscope-assisted posterior decompression technique using the SYNCHA microendoscopic system with a 12-mm tubular retractor is not only safe, minimally invasive, and effective for the treatment of CSR, but it may also provide advantages over FESS and BESS. Future studies with larger sample sizes, long-term follow-up, and randomized prospective comparison with the 16-mm tubular retractor, FESS, and BESS are necessary to confirm the advantages of this technique.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Microendoscopic approach to far-lateral lumbar disc herniation Neurosurg Focus Foley KT Smith MM Rampersaud YR 07199910.3171/foc.1999.7.6.616918212 · doi ↗ · pubmed ↗
- 2Assessment of the learning curve for microendoscopic decompression surgery for lumbar spinal canal stenosis through an analysis of 480 cases involving a single surgeon Global Spine J Nomura K Yoshida M 5458720172845151010.1055/s-0036-1583943 PMC 5400167 · doi ↗ · pubmed ↗
- 3Microendoscopic posterior cervical laminoforaminotomy for unilateral radiculopathy: results of a new technique in 100 cases J Neurosurg Adamson TE 515795200110.3171/spi.2001.95.1.005111453432 · doi ↗ · pubmed ↗
- 4Clinical outcomes after microendoscopic laminotomy for lumbar spinal stenosis: a 5-year follow-up study Eur Spine J Minamide A Yoshida M Yamada H Nakagawa Y Hashizume H Iwasaki H Tsutsui S 3964032420152534180410.1007/s 00586-014-3599-x · doi ↗ · pubmed ↗
- 5Full endoscopic spine surgery for cervical spondylotic myelopathy: a systematic review World Neurosurg Chang CJ Liu YF Hsiao YM 14215017520233716907710.1016/j.wneu.2023.05.012 · doi ↗ · pubmed ↗
- 6Full-endoscopic versus microscopic spinal decompression for lumbar spinal stenosis: a systematic review & meta-analysis Spine J Chin BZ Yong JH Wang E Sim SI Lin S Wu PH Hey HW 102210332420243819089210.1016/j.spinee.2023.12.009 · doi ↗ · pubmed ↗
- 7Contraindications and complications of full endoscopic lumbar decompression for lumbar spinal stenosis: a systematic review World Neurosurg Ju CI Kim P Ha SW Kim SW Lee SM 39841016820223652721910.1016/j.wneu.2022.07.066 · doi ↗ · pubmed ↗
- 8Short-term efficacy of unilateral biportal endoscopy technology in the treatment of cervical spondylotic radiculopathy Eur Spine J Wen M Li X Lu X Chen T Qin R 1181273420253950395310.1007/s 00586-024-08545-7 · doi ↗ · pubmed ↗