Evaluation of wooden spatula and plastic pipette methods for caries risk assessment in infants and toddlers
Silvina Tineo, Paulo Nelson-Filho, Thais Citolino Barbosa, José Maria Alvarez Gimenez, Raquel Assed Bezzera da Silva, Lea Assed Bezzera da Silva, Marta Estela Saravia

TL;DR
The study compared wooden spatula and plastic pipette methods for collecting saliva to assess caries risk in young children, finding both methods effective but the spatula better tolerated.
Contribution
The study introduces a comparison of saliva collection methods for caries risk assessment in infants and toddlers, emphasizing behavioral acceptance.
Findings
No significant difference in MS CFU counts between wooden spatula and plastic pipette methods.
Older children (18-29 months) had higher MS CFU counts than younger children (1-6 months).
Children showed better behavior during saliva collection with the wooden spatula.
Abstract
The study aimed to compare two different methods (wooden spatula and plastic pipette) for the collection of unstimulated saliva for colony counting of Mutans Streptococci species (MS) (microbiological caries risk), in infants and toddlers. The children’s behavior was favorable (very comfortable or comfortable) and unfavorable (uncomfortable or very uncomfortable), while the saliva collection, was also evaluated. Saliva samples were obtained from 19 children aged 1-29 months, of both sexes and seeded by both methods, obtaining the MS CFU numbers. The ANOVA test was used to statistically analyze the microbiological results, and the Z-test and chi-square test were used to analyze the behavioral assessment (α= 0,05%). 63.1% and 57.9% of children had MS in their saliva, using the saliva collection techniques with a spatula and a pipette, respectively. The number of CFUs was an average of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
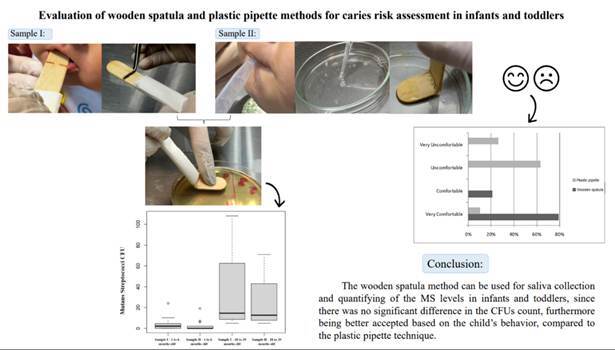 Figure 1
Figure 1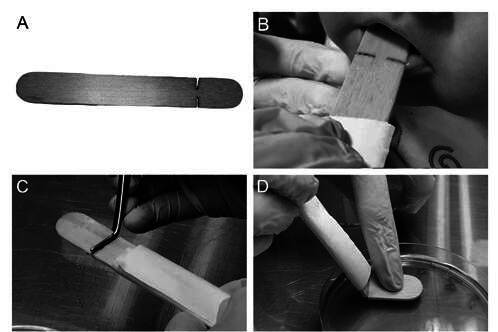 Figure 2
Figure 2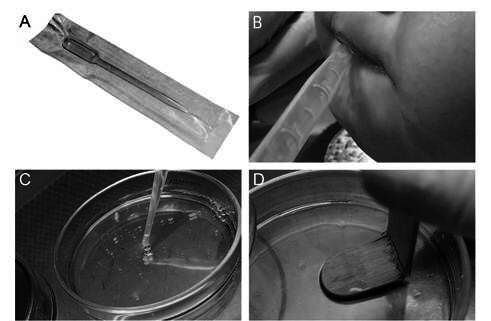 Figure 3
Figure 3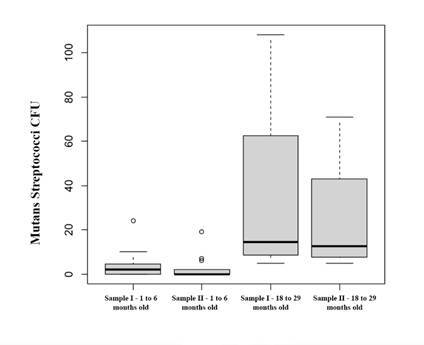 Figure 4
Figure 4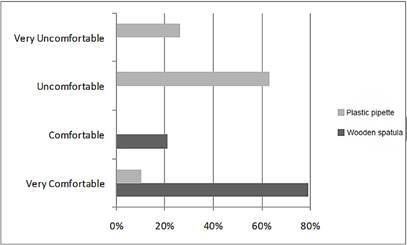 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Oral microbiology and periodontitis research · Dental Research and COVID-19
Introduction
Early Childhood Caries (ECC) can be defined as the presence of one or more decayed (cavitated/non-cavitated lesions), missing, or filled surfaces due to caries in the primary teeth of children under six years old 1. This condition remains a significant chronic disease of childhood and a public health problem 2.
ECC is preventable, but currently affects more than 600 million children worldwide, causing a negative impact on children’s life quality. ECC, like other forms of dental caries, is considered to be a biofilm‐mediated, sugar‐driven, multifactorial, dynamic disease that results in the imbalance of demineralization and remineralization of dental hard tissues 1.
Bacterial colonization of an infant’s oral cavity is a key factor for caries risk 3. Traditional microbial risk markers for ECC include acidogenic-aciduric bacterial species, especially Mutans Streptococci (MS) species, that can be detected by microbial culture and molecular biology. It is known that high levels of Streptococcus mutans are a strong risk factor for ECC 4 and that the amount of S. mutans is significantly higher in the saliva and biofilm of children with cavitated lesions 5.
In children and neonates, saliva makes the perfect diagnostic medium for microbiological risk diagnosis of caries because of its noninvasive collection, easy handling, and storage of samples 6 .
There is a variety of saliva collection methodologies, but collection of unstimulated saliva by passive drool directly into plastic tubes 7 and sterile pipettes 3 are the most utilized methods. However, the choice of collection method should be carefully evaluated, considering the involved populations (elderly, neonates, and children) 6. According to Fey et al. (2024) 8, the absorption and suction methods, including the use of plastic pipettes, were preferred in situations involving young and uncooperative children.
In 1979, Köhler and Bratthall 9 developed a method (stamp method) to facilitate the estimation of MS levels in saliva, using wooden spatulas pressed directly against a selective medium, in adults and children under 3 to 6 years. However, the literature on this topic is scarce using this technique in young children 10 , and it has not been assessed so far in infants and toddlers (children aged 0 to 3 years old).
Thus, this study aimed to compare two methods (wooden spatula and plastic pipette) for the collection of unstimulated saliva for colony counting of MS (microbiological caries risk), in children 1-29 months old. The child’s behavior during the collection of saliva samples using the two techniques was also evaluated.
Materials and methods
This study was carried out in the Oral Biology Laboratory of the School of Dentistry of the National University of Tucumán (LABOFOUNT) in Argentina, with samples obtained from infants and toddlers, of both sexes, from 1 to 29 months old (mean of 7.68 months). Children who used antimicrobial agents or antibiotics in the previous 3 months were excluded. The study was previously approved by the Research Ethics Committee involving Human Beings of the School of Medicine of the UNT (PIUNT J/611). The signing of the informed consent form was required before participation, by the mother, who signed on her name and her child.
Saliva samples were collected from each patient using 2 different methods (Sample I and Sample II), sequentially, in the morning, at least 2 hours after the last food intake and the last cleaning of the oral cavity:
Sample I (n=19): Unstimulated saliva samples were collected by the wooden spatula method 9. An adapted wooden sterilized spatula (Figure 1A), was introduced into the oral cavity of each child (Figure 1B), being moistened with saliva using rotating movements. It should be highlighted that the spatula was gently pressed not only on the tongue’s surface but also on all surfaces of the oral cavity, mainly on the cheek’s surface and on the back of the tongue, for 1 minute. Then, the spatula was broken with the aid of sterilized tweezers (Figure 1C) and softly pressed on a Petri dish containing the SB-20M culture médium 11 (Figure 1D).
Figure 1. Collection of saliva samples in infants and toddlers, by wooden spatula technique and seeding in SB-20M culture medium. A - Adapted wooden spatula; B - Collection of saliva sample; C- Spatula breakage with the aid of sterilized tweezer; D - Sample seeding in the SB-20M culture medium.
Sample II (n=19): Unstimulated saliva samples (2mL) were collected from the floor of the mouth with a 3mL disposable plastic pipette (Pasteur Prolab Materials for Laboratory Pipette - Brazil), by aspiration (Figures 2A and B). The 2mL of saliva was deposited in sterilized Petri dishes (Figure 2C). Wooden spatulas, similar to those used for sample I, were broken with the aid of sterilized tweezers and soaked in the saliva contained in these Petri dishes for 1 minute. Later, the spatula was softly pressed on a Petri dish containing the SB-20M culture medium 11, as described for sample I (Figure 2D). Thus, for each patient, the samples collected with the 2 techniques were seeded in the same Petri dish.
Figure 2. Collection of saliva samples in infants and toddlers, by disposable plastic pipette technique and seeding in SB-20M culture medium. A - Disposable plastic pipette; B - Collection of saliva sample; C- Saliva sample deposited in sterilized Petri dishes, for the immersion of the wooden spatula; D - Wooden spatula seeding in the SB-20M culture medium.
Subsequently, the samples I and II Petri dishes were incubated in anaerobic jars, under microaerophilic conditions, using the candle flame system, for 72 hours, at 37ºC 12 ^,^ 13. After the incubation period, MS Colony Forming Units (CFUs) were counted per mL of saliva, based on typical morphological characteristics. The count was carried out by an experienced evaluator (S.T.) and calibrated (kappa=0.85), using a stereomicroscope (ZTX-3D-C2 Numak, China). with reflected light, at 20x magnification, as described by Saravia et al. 2 ^,^ 15 ^) (^ 12. After counting the colonies the samples were divided into two groups based on the ages of the infants (1-6 months) and toddlers (18-29 months).
In cases of uncertainty about the morphological identification of MS, proteomic identification was performed by the MALDI-TOF mass spectrometry technique 13.
The clinical evaluation of infants' behavior during saliva sample collection for the wooden spatula technique and the plastic pipette technique, was also performed by an operator with clinical experience in Pediatric Dentistry (S.T.). The following categories were considered:
Very comfortable: The sample collection process was very comfortable for both the patient and operator.
Comfortable: The sample collection process was comfortable for both the patient and operator, with minor difficulty for the operator.
Uncomfortable: The sample collection process was not entirely comfortable for both the patient and the operator.
Very uncomfortable: The sample collection process was entirely uncomfortable for both the patient and the operator.
The microbiological results were statistically analyzed by the ANOVA, using the R language software. The Z-test using the R language and the chi-square test were used to analyze the behavior of the infants and toddlers. The significance level was set at 5%.
Results
The results are expressed in Table 1 and Figures 3 and 4.
Table 1. Number of CFUs obtained after collecting unstimulated saliva using a wooden spatula or plastic pipette in infants and toddlers.PatientAge (months)Sample I (wooden spatula)Sample II (plastic pipette)1106222032004200526063307310784009552105001150212524191350014631156411618551719108711824121019291715Total of CFU 199137Mean7.6810.477.32SD8.2624.5116.38CV107%234%224%
As shown in Table 1, it should be noted that MS was detected in the saliva of 63.1% and 57.9% of children, using the wooden spatula (Sample I) and the plastic pipette (Sample II) techniques, respectively. The number of CFUs ranged from 0 to 108, with an average of 10.47 for saliva collected with the wooden spatula and 7.32 for saliva collected with the plastic pipette. When comparing the two different methods of saliva collection in infants and toddlers, no statistically significant difference was observed between them (p=0.696653).
Figure 3 presents that in children aged 1-6 months, the average CFUs was 3.80 for the wooden spatula and 2.53 for the plastic pipette. On the other hand, in children aged 18-29 months, the average CFU was 35.50 for the wooden spatula and 25.25 for the plastic pipette. The statistical analysis showed a significant difference (p=0.000383) between the age groups of 1-6 months and 18-29 months, with higher numbers of CFU in older children, for both saliva collection techniques.
Figure 3. Boxplot showing the number of CFUs obtained in infants (children aged 1-6 months) and toddlers (children aged 18-29 months), after collecting saliva using a wooden spatula (Sample I) or plastic pipette (Sample II).
Figure 4 presents the results of the clinical assessment of the child’s behavior during the collection of saliva samples using the wooden spatula and plastic pipette techniques.
Figure 4. Results of the evaluation of infants and toddlers' behavior during unstimulated saliva collection using a wooden spatula or plastic pipette.
For the wooden spatula the predominant behavior was “Very Comfortable” (78.95%), while for the plastic pipette the predominant behavior was “Uncomfortable” (63.16%).
The statistical analysis showed a significant difference (p<0.001) between the saliva sample collection techniques, with positive behavior (very comfortable and comfortable) from the child when the wooden spatula was used.
Discussion
According to Carrol (2024) 14, the factors found to be relevant in the development of ECC were the child's age, toothbrushing quality/plaque control, parental involvement in toothbrushing, fluoride exposure, pattern of dental attendance, dietary sugar exposure, habits, clinically carious active lesion presence, the socio-economic status of the child and their family, and the oral bacterial composition (Streptococcus mutans presence). Thang Le et al. (2021) 15 also observed that high levels of MS are a potential risk factor for ECC. However, obtaining saliva samples from young children (infants and toddlers) for microbiological caries risk assessment may present some difficulties related to cooperation and a disadvantageous perception of the procedure.
In this regard, during the clinical phase of the present study, we observed that obtaining saliva samples with the spatula, in this young population group, was easier for the operator and more convenient and comfortable for the child, compared to the plastic pipette. This fact shows that the wooden spatula technique can contribute to a more positive and less stressful experience during saliva collection. When using the pipette, it was clinically observed that the children closed their mouths more frequently and showed reflexes and actions of refusal during the saliva collection procedure. In parallel, the operator performed the procedure with a sense of unease, cautiously to avoid damaging the soft tissues, since the pipette has a rigid tip, unlike the wooden spatula which, despite being rigid, is circular and does not have sharp edges.
The collection of saliva samples in young children has been carried out mainly using sterile swabs 16 ^,^ 17, passive drool directly into sterile vials 18, sterile tongue blades 19 ^,^ 20, and pipettes 3. It should be noted that in studies that used sterile tongue blades, the samples were collected by keeping the spatula on the tongue for 1 minute. In the present study, we observed that children showed positive behavior when the wooden spatula was used, with a statistically significant difference, compared to the pipette technique. Possibly, the children accepted the procedure better with the spatula, as it was moved, for 1 minute, over all surfaces of the oral cavity, mainly the cheeks on both sides and the tongue, and not kept just on the surface of the tongue, which made the procedure clinically more pleasant for infants and toddlers.
The wooden spatula technique proposed by Köhler and Bratthall in 1979 9 was initially described for adults and children under 3 to 6 years and used in different populations to determine caries risk, for example, in dental students 12 and children of up to 3 years old 21 ^,^ 22. Our results showed that this technique can be used to determine the microbiological caries risk in infants and toddlers. It should be noted that, due to the ease of implementation and the comfort it provides to the patient, the wooden spatula technique can also be used to quantify other microorganisms involved in pathologies of the oral cavity.
In the present study, two techniques for obtaining unstimulated saliva samples in children aged 1-29 months were compared, one by wetting a wooden spatula in the baby’s mouth and the other by absorbing saliva with a plastic pipette. The results with both techniques did not show a statistically significant difference in the CFU count of MS. As each child underwent saliva collection using both techniques, we can assume that possible differences would be attributed solely to the saliva sampling technique.
Another important result of the present study was the significant difference between the age groups of 1-6 months and 18-29 months, with higher numbers of CFUs in older children, for both the saliva collection techniques. These results are in agreement with those obtained by Fujiwara et al. (1991) 23, who evaluated the number and species distribution of salivary Mutans Streptococci in children aged 0-2 years old, observing that the detection rate of MS increased with age, correlated with the number of erupted teeth.
Conclusion
Therefore, we conclude that the wooden spatula method can be used for saliva collection and quantifying of the Mutans Streptococci levels in infants and toddlers, since no significant difference was observed in the CFUs count, being better accepted based on the child’s behavior, as well as the operator clinically determined that using the spatula provides greater comfort, compared to the plastic pipette technique.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Early Childhood Caries IAPD Bangkok Declaration Int J Paediatr Dent 20192933843863109912910.1111/ipd.12490 · doi ↗ · pubmed ↗
- 2American Academy of Pediatric Dentistry Proceedings of theconference: innovations in the prevention and management of early childhood caries, Ill 2014 Chicago Pediatr Dent 201537319829926063549 · pubmed ↗
- 3Wassel MO Salman NS Metwalli NE A preliminarily investigation on oral colonization and counts of Streptococcus mutans and Streptococcus mitis in a group of predentate infants in relation to some maternal and infant factors (a longitudinal observational study)Int J Clin Pediatr Dent 202316179863702078410.5005/jp-journals-10005-2486 PMC 10067990 · doi ↗ · pubmed ↗
- 4Kirthiga M Murugan M Saikia A Kirubakaran R Risk factors for early childhood caries: a systematic review and meta-analysis of case control and cohort studies Pediatr Dent 2019154129511230992106 PMC 7100045 · pubmed ↗
- 5Manchanda S Cheung BPK Lee GHM Lo ECM Yiu CKY Quantitative analysis of salivary and biofilm bacteria associated with cavitated and non-cavitated carious lesions in pre-school children Arch Oral Biol 202314610560710.1016/j.archoralbio.2022.10560736543040 · doi ↗ · pubmed ↗
- 6Pappa E Kousvelari E Vastardis H Saliva in the "Omics" era: a promising tool in paediatrics Oral Dis 201925116252975038610.1111/odi.12886 · doi ↗ · pubmed ↗
- 7Kaczor-Urbanowicz KE Deutsch O Zaks B Krief G Chaushu S Palmon A Identification of salivary protein biomarkers for orthodontically induced inflammatory root resorption Proteomics Clin Appl 20171191010.1002/prca.20160011928371361 · doi ↗ · pubmed ↗
- 8Fey JMH Bikker FJ Hesse D Saliva Collection methods among children and adolescents: a scoping review Mol Diagn Ther 202428115263795013610.1007/s 40291-023-00684-9PMC 10786738 · doi ↗ · pubmed ↗