Outcomes of Patients with Cirrhosis Undergoing Cardiac Defibrillator Placement: A Nationwide Analysis
Ahmed Younes, Hossam Albeyoumi, Ahmed K Mahmoud, Ibrahim Kamel, Ahmed M Maraey, Mahmoud Khalil

TL;DR
This study finds that patients with liver cirrhosis face higher risks and costs after getting a cardiac defibrillator.
Contribution
The study is the first nationwide analysis of cardiac defibrillator outcomes specifically in patients with cirrhosis.
Findings
Patients with cirrhosis had higher inpatient mortality and bleeding risks after defibrillator implantation.
Hospital stays and costs were significantly higher for cirrhosis patients undergoing the procedure.
Cirrhosis patients had a reduced risk of heart attacks but no significant difference in stroke risk.
Abstract
Background Invasive procedures pose a greater risk for patients with liver cirrhosis. This study investigates the impact of cirrhosis on the outcomes of implantable cardiac defibrillator (ICD) implantation. Methods We conducted a retrospective analysis using the National Readmissions Database (NRD) from 2016 to 2020. Adult patients who received an ICD, identified by the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) codes, were included. Outcomes were compared between patients with and without underlying liver cirrhosis. The primary outcome was all-cause inpatient mortality. Secondary outcomes included ischemic cerebrovascular accidents (CVA), major bleeding (gastrointestinal, intracranial, pulmonary, and other bleeding), packed red blood cell (pRBC) transfusion, pericardial complications (pericardial effusion, hemopericardium,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
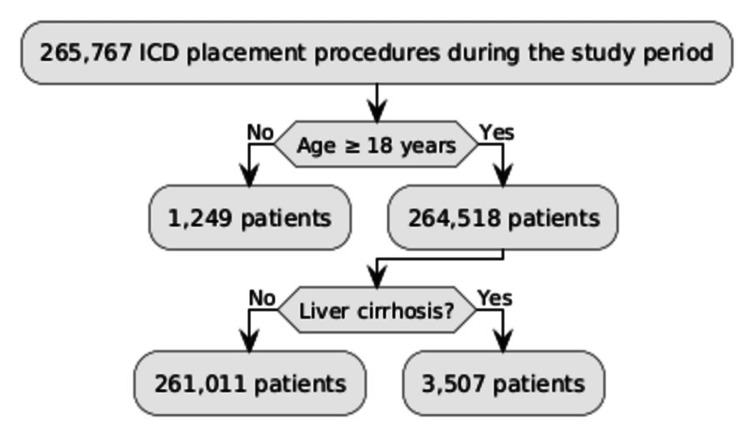 Figure 1
Figure 1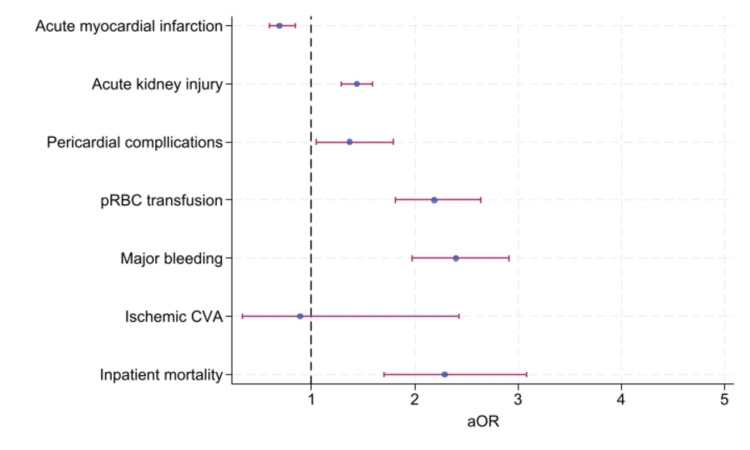 Figure 2
Figure 2| ICD with no cirrhosis N=261,011 (98.7%) | ICD with cirrhosis N = 3,507 (1.3%) | P-value | |
| Age, mean, and SD | 65.7 (±0.2) | 62.8 (±0.5) | <0.001 |
| Female (%) | 74,314 (28.4%) | 735 (20.9%) | <0.001 |
| Primary insurance (%) | <0.001 | ||
| Medicare | 160,662 (61.6) | 2,098 (59.9) | |
| Medicaid | 28,757 (11) | 700 (19.9) | |
| Private insurance | 57,003 (21.9) | 515 (14.7) | |
| Self-pay | 6,055 (2.3) | 80 (2.3) | |
| No charge/other | 8,212(3.1) | 110 (3.1) | |
| Median household income for patient's zip code (%) | <0.001 | ||
| 0-25th percentile | 77,090 (30.0) | 1,243 (35.9) | |
| 26th-50th percentile | 70,548 (27.4) | 877 (25.4) | |
| 51st-75th percentile | 61,274 (23.8) | 810 (23.4) | |
| 76th-100th percentile | 48,472 (18.8) | 527 (15.3) | |
| Hospital bed size (%) | 0.03 | ||
| Small | 23,334 (8.9) | 249 (7.1) | |
| Medium | 65,282 (25) | 892 (25.4) | |
| Large | 172,396 (66.1) | 2,367 (67.5) | |
| Hospital location and teaching status (%) | 0.28 | ||
| Metropolitan non-teaching | 42,175 (16.1) | 617 (17.6) | |
| Metropolitan teaching | 212,345 (81.4) | 2,809 (80.1) | |
| Non-metropolitan hospital | 6,492 (2.5) | 81 (2.3) | |
| Hypertension (%) | 53,648 (20.6) | 435 (12.4) | <0.001 |
| Diabetes mellitus (%) | 42,339 (16.2) | 825 (23.5) | <0.001 |
| Tobacco smoking (%) | 38,107 (14.6) | 729 (20.8) | <0.001 |
| PVD (%) | 17,572 (6.7) | 272 (7.8) | 0.09 |
| CKD (%) | 76,964 (29.5) | 1,364 (38.9) | <0.001 |
| Heart failure (%) | 224,828 (86.1) | 3,212 (91.6) | <0.001 |
| History of CAD (%) | 107,838 (41.3) | 1,264 (36) | <0.001 |
| Atrial fibrillation (%) | 109,295 (41.9) | 1,734 (49.4) | <0.001 |
| Parameters | ICD without cirrhosis N=261,011 (98.7%) | ICD with cirrhosis N = 3,507 (1.3%) | aOR/aMD (95% CI) | p-value |
| Inpatient mortality (%) | 2,876 (1.1%) | 94 (2.7%) | 2.29 (1.70 - 3.08) | <0.001 |
| Ischemic CVA (%) | 484 (0.2%) | 6 (0.2%) | 0.89 (0.33 - 2.43) | 0.83 |
| Major bleeding (%) | 6,424 (2.5%) | 222 (6.3%) | 2.40 (1.97-2.91) | <0.001 |
| pRBC transfusion (%) | 8,609 (3.3%) | 260 (7.4%) | 2.19 (1.81 - 2.64) | <0.001 |
| Pericardial complications (%) | 5,579 (2.1) | 101 (2.9) | 1.37 (1.05 - 1.79) | 0.02 |
| Acute kidney injury (%) | 78,186 (29.9) | 1,494 (42.6) | 1.44 (1.29 - 1.59) | <0.001 |
| Acute myocardial infarction (%) | 30,042 (11.5) | 287 (8.2) | 0.69 (0.59 - 0.84) | <0.001 |
| LOS, days, mean (SD) | 8.3 (±0.1) | 11.9 (±0.6) | 2.79 (2.20 - 3.37) | <0.001 |
| Total charges, $, mean (SD) | 241,723 (±4,923) | 287,661 (±13,596) | 35,624 (23,698 - 47,549) | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Liver Disease Diagnosis and Treatment · Organ Transplantation Techniques and Outcomes
Introduction
Implantable cardioverter defibrillators (ICDs) are a cornerstone therapy for preventing sudden cardiac death in high-risk patients. Survival benefits have been demonstrated in clinical trials and real-world clinical practice data [1].
Cirrhosis is a significant global public health issue with an increasing prevalence. Recent estimates indicate that between 107 and 119 million people worldwide have cirrhosis, with about 2.4% of global deaths related to it [2,3]. Patients with cirrhosis often experience systemic complications that present considerable clinical challenges. Among these is cirrhotic cardiomyopathy, which increases the risk of arrhythmias and heart failure [4].
Patients with liver cirrhosis undergoing invasive procedures generally face increased risks of adverse outcomes, particularly those with higher Child-Pugh classes or Model for End-Stage Liver Disease (MELD) scores exceeding 13 [5]. However, there is limited data on the safety and outcomes of ICD implantation in this population.
Utilizing a large national database in this study, we aim to evaluate the risk of patients with cirrhosis undergoing ICD placement to better inform clinical decision-making.
Materials and methods
Data sources, study population, and outcomes
This retrospective study utilizes the National Readmission Database (NRD) from 2016 to 2020 [6]. The NRD is a comprehensive, public, all-payer database provided by the Agency for Healthcare Research and Quality (AHRQ) that includes more than 50% of hospitalizations in the United States [7]. To ensure the generalizability of results, discharge weights were applied to each record.
The study included adult patients (aged >18 years) who underwent ICD placement during the study period. Patients were identified using the appropriate International Statistical Classification of Diseases and Related Health Problems 10^th^ Revision (ICD-10) codes [8] detailed in Appendix A. Outcomes were then compared between patients with and without liver cirrhosis.
Key patient characteristics examined included age, sex, hypertension, diabetes mellitus, smoking, peripheral vascular disease (PVD), chronic kidney disease (CKD), heart failure, history of coronary artery disease (CAD) (defined as a history of myocardial infarction, percutaneous coronary intervention, or coronary artery bypass graft), atrial fibrillation (AF), primary insurance type, and median income for the patient’s Zone Improvement Plan (ZIP) code. Hospital-level characteristics included bed size, location, and teaching status. Baseline characteristics are summarized in Table 1.
The primary outcome was all-cause inpatient mortality, while secondary outcomes included ischemic cerebrovascular accidents (CVA), major bleeding (defined as gastrointestinal, intracranial, pulmonary, and other bleeding), packed red blood cell (pRBC) transfusion, pericardial complications (defined as pericardial effusion, hemopericardium, or pericardial tamponade), acute kidney injury (AKI), length of stay (LOS), and total charges.
Statistical analysis
In this study, categorical variables were expressed as frequencies and percentages, with comparisons performed using chi-square tests. Continuous variables were expressed as means and standard deviations, and comparisons were conducted using Student's t-tests. Logistic regression was employed to analyze dichotomous and categorical variables, while linear regression was used for continuous variables. Multivariate models were developed for both logistic and linear regressions.
The models were adjusted for age, sex, hypertension, diabetes mellitus, smoking, PVD, CKD, heart failure, history of CAD, AF, and primary insurance type. These variables were selected based on their statistical significance (P<0.05) in univariate analyses of baseline characteristics against the primary outcome. A P-value threshold of <0.05 was considered statistically significant for all analyses. This study did not require ethical approval as no data from human subjects or animals were collected.
Results
Among 264,518 patients who underwent ICD placement, 3,507 patients (1.3%) had liver cirrhosis. Baseline characteristics are summarized in Table 1. The flow chart summarizing the patient population is in Figure 1.
Flowchart summarizing patient populationICD: implantable cardiac defibrillator
Primary outcomes
Liver cirrhosis was associated with significantly increased inpatient mortality (adjusted odds ratio (aOR): 2.29, 95% confidence interval (CI): 1.70-3.08, P<0.001).
Secondary outcomes
Liver cirrhosis was associated with significantly increased major bleeding (aOR: 2.40, CI: 1.97-2.91, P<0.001), pRBC transfusion (aOR: 2.19, CI: 1.81-2.64, P<0.001), pericardial complications (aOR: 1.37, CI: 1.05-1.79, P=0.02), and AKI (aOR: 1.44, CI: 1.29-1.59, P<0.001), without significant difference in ischemic CVA (aOR: 0.89, CI: 0.33-2.43, p=0.83) and with reduced incidence of AMI (aOR: 0.69, CI: 0.59-0.84, P<0.001). The primary and secondary outcomes are summarized in Table 2 and the forest plot is in Figure 2.
Forest plot of the primary and secondary outcomespRBC: packed red blood cell; CVA: cerebrovascular accident; aOR: adjusted odds ratio
Resource utilization
Liver cirrhosis was also associated with increased resource utilization with increased LOS (adjusted mean difference (aMD): 2.79 days, CI: 2.20-3.37, P<0.001), and total charges (aMD: $35,624, CI: 23,698-47,549, P<0.001).
Discussion
This study utilized the NRD from 2016 to 2020 [6] to evaluate the impact of liver cirrhosis on outcomes after ICD placement. We found that patients with cirrhosis are generally at increased risk of inpatient mortality and postprocedural complications.
Implantable cardiac defibrillators have demonstrated a survival benefit, reducing the risk of sudden cardiac death in high-risk patients [1]. However, our study shows that liver cirrhosis is associated with about a two-fold increased risk of inpatient mortality after ICD placement. This finding aligns with the understanding that cirrhosis is associated with multiple systemic complications, including cirrhotic cardiomyopathy, which can increase the risk of arrhythmias and heart failure [4]. Furthermore, patients with advanced liver disease, particularly those with higher Child-Pugh classes or MELD scores exceeding 13, generally face increased risks of adverse outcomes after invasive procedures [5].
We also found that liver cirrhosis is associated with a significant increase in major bleeding and the need for pRBC transfusion. This is consistent with the known coagulopathy and altered hemostasis commonly observed in patients with cirrhosis [9]. Impaired hepatic synthetic function, portal hypertension, reduced platelet count and function, and increased fibrinolysis can contribute to an increased risk of bleeding in this population [10].
Our study identified a higher risk of pericardial complications, including pericardial effusion and tamponade, in cirrhotic patients. While pericardial complications are rare in the general ICD population, cirrhotic patients may be more susceptible due to homeostatic imbalances, venous congestion, and a propensity for pericardial effusion associated with advanced liver disease [11]. Previous studies have reported an increased risk of pericardial effusion following cardiovascular interventions in cirrhotic patients, further supporting our findings [12].
Patients with cirrhosis face a significantly elevated risk of developing AKI due to systemic complications associated with their liver disease. The hallmark hyperdynamic circulation in cirrhosis leads to reduced effective blood volume, triggering vasoconstrictive responses and chronic renal hypoperfusion [13]. This makes cirrhotic patients more vulnerable to AKI from common events like infections or bleeding [14,15]. Factors such as nephrotoxic medications, intrinsic kidney diseases, and cholemic nephropathy further compound the risk of AKI in this population [16].
Interestingly, our study found that cirrhosis is associated with a decreased risk of AMI. This finding is consistent with previous research suggesting that cirrhotic patients have a lower prevalence of AMI despite their high burden of cardiovascular risk factors [17]. The underlying mechanism remains unclear but may be related to altered coagulation profiles in cirrhosis, which can confer a form of “natural anticoagulation,” reducing the incidence of coronary thrombosis [18]. Additionally, cirrhotic patients often have lower systemic vascular resistance and altered lipid metabolism, potentially contributing to a reduced risk of atherosclerosis and subsequent AMI [18].
A major strength of our study is the utilization of a large, nationally representative database, allowing for a robust comparison of the outcomes between patients with and without cirrhosis. The adjustment for multiple confounders, including comorbid conditions and hospital-level factors, enhances the validity of our findings. However, the study also has limitations. As a retrospective observational study using an administrative database, it is subject to potential biases related to coding accuracy and unmeasured confounders. The NRD lacks granular data on disease severity beyond ICD-10 coding, limiting our ability to stratify outcomes. Lastly, long-term outcomes beyond the initial hospitalization were not assessed, warranting further studies to evaluate longer-term mortality and morbidity in this high-risk cohort.
Conclusions
In conclusion, patients with liver cirrhosis undergoing ICD placement face significantly higher risks of inpatient mortality, major bleeding, pericardial complications, and AKI. These findings highlight the need for careful risk assessment and multidisciplinary management to improve outcomes. While ICDs remain crucial for preventing sudden cardiac death, clinicians should weigh their benefits against the increased procedural risks in cirrhotic patients. The lower incidence of AMI in this population suggests unique cardiovascular pathophysiology that warrants further study. Future research should focus on refining risk prediction models and exploring alternative management strategies for high-risk patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Survival of patients receiving a primary prevention implantable cardioverter-defibrillator in clinical practice vs clinical trials JAMA Al-Khatib SM Hellkamp A Bardy GH 556230920132328022510.1001/jama.2012.157182 PMC 3638257 · doi ↗ · pubmed ↗
- 2Epidemiology of liver cirrhosis and associated complications: current knowledge and future directions World J Gastroenterol Liu YB Chen MK 591059302820223640510610.3748/wjg.v 28.i 41.5910 PMC 9669831 · doi ↗ · pubmed ↗
- 3Global epidemiology of cirrhosis - aetiology, trends and predictions Nat Rev Gastroenterol Hepatol Huang DQ Terrault NA Tacke F Gluud LL Arrese M Bugianesi E Loomba R 3883982020233697779410.1038/s 41575-023-00759-2PMC 10043867 · doi ↗ · pubmed ↗
- 4Review article: comprehensive analysis of cirrhotic cardiomyopathy Aliment Pharmacol Ther Chahal D Liu H Shamatutu C Sidhu H Lee SS Marquez V 9859985320213368916910.1111/apt.16305 · doi ↗ · pubmed ↗
- 5Do patients with liver cirrhosis undergoing cardiac surgery have acceptable outcomes?Interact Cardiovasc Thorac Surg Modi A Vohra HA Barlow CW 6306341120102073940510.1510/icvts.2010.241190 · doi ↗ · pubmed ↗
- 6National Readmissions Database 2024 https://hcup-us.ahrq.gov/nrdoverview.jsp
- 7Socioeconomic and demographic determinants of readmission rates in congestive heart failure patients: insights from the nationwide readmissions database Cureus Mohyeldin M Allu S Schmidt P Shrivastava S Parikh H Khaja M 0162024 https://pmc.ncbi.nlm.nih.gov/articles/PMC 11280965/10.7759/cureus.63227 PMC 1128096539070351 · doi ↗ · pubmed ↗
- 8ICD-10: International Statistical Classification of Diseases and Related Health Problems: tenth revision, 2nd ed 2004 https://iris.who.int/handle/10665/429803376487 · pubmed ↗