Ball versus other attachments in mini implant retained overdenture: a systematic review and meta-analysis
Zin Hnin Pwint Aung, Pyae Phyo Win, Thanapat Sastraruji, Pathawee Khongkhunthian

TL;DR
This study compares different attachment systems in mini implant overdentures and finds similar bone loss outcomes for ball, bar, and ERA® attachments, with telescopic attachments showing more bone loss.
Contribution
The study provides a systematic review and meta-analysis comparing ball attachments with other systems in mini-implant overdentures.
Findings
Ball attachments showed better results than telescopic ones in marginal bone loss (p < 0.05).
Ball, bar, and ERA® attachments had similar marginal bone loss outcomes.
Ball attachments required fewer interventions than ERA® attachments over one year.
Abstract
Mini implant retained overdentures have been treated in edentulous patients with promising long-term results. However, various attachment systems in this process remain insufficiently investigated. This systematic review and meta-analysis aimed to compare the effects of the ball and other attachments used in mini-implant overdentures. Marginal bone loss, bite force, implant survival rate, prosthetic maintenance, and complications were assessed. A systematic search was conducted across PubMed, Cochrane Library, and Scopus databases until 25th February 2025. This systematic review aimed to find studies that compare ball attachments with other attachment systems in mini dental implant (MDI) overdentures. The primary outcome was marginal bone loss, while the secondary outcomes were maximum bite force, implant survival rate, prosthetic maintenance, and complications. The risk of bias was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
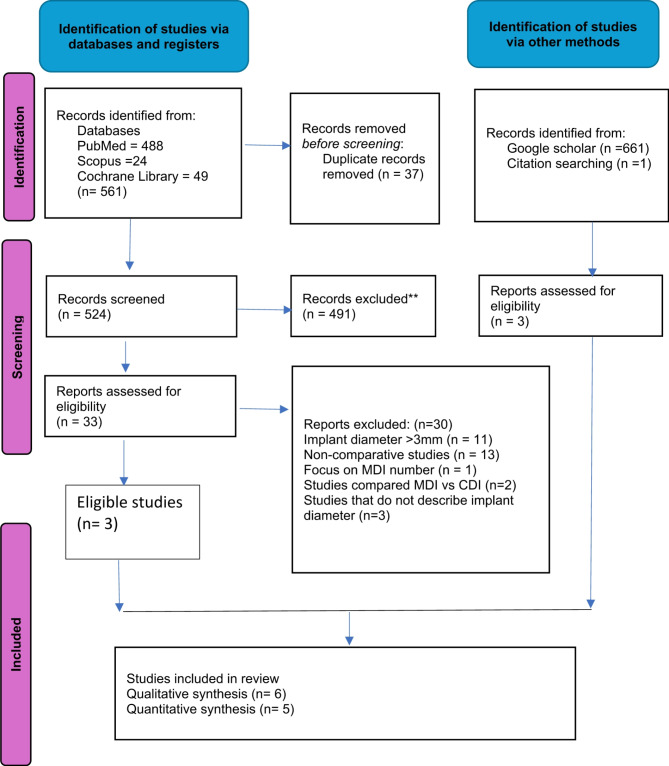 Figure 1
Figure 1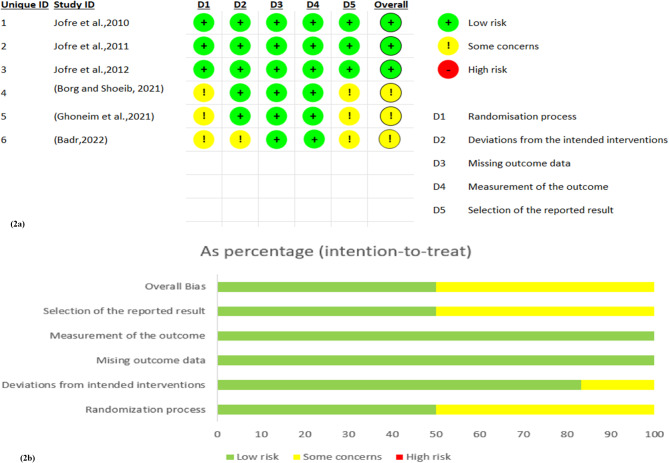 Figure 2
Figure 2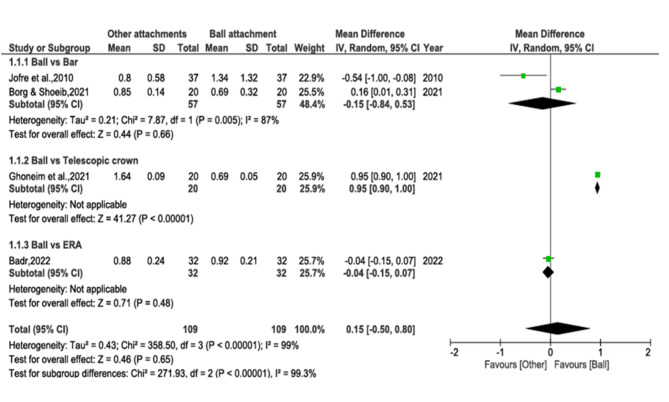 Figure 3
Figure 3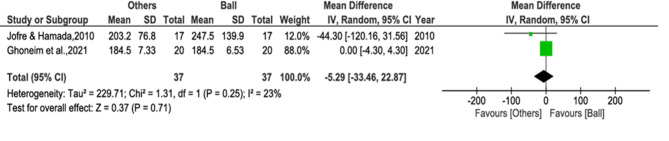 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Implant Techniques and Outcomes · Periodontal Regeneration and Treatments · Orthodontics and Dentofacial Orthopedics
Introduction
Two-implant retained overdentures are a widely recognized approach for rehabilitating mandibular edentulism, improving function and patient satisfaction [1–3]. Nevertheless, bone resorption after tooth loss often complicates conventional implant (CDI) placement, particularly in elderly or medically compromised individuals [4, 5]. Mini dental implants (MDIs), which are less than 3 mm in diameter, provide a viable alternative for atrophic alveolar ridges [6]. The Glossary of Oral and Maxillofacial Implants (GOMI) defines MDIs as “dental implants made from biocompatible materials comparable to conventional implants but with reduced dimensions” [7]. First introduced in 1994 and later approved by the FDA for both temporary and long-term use, MDIs are now widely applied in prosthodontics [8–10].
One critical factor in assessing MDIs’ success is marginal bone loss (MBL), as it directly impacts implant stability and longevity [11]. Studies have shown that MDI-supported overdentures exhibit favourable MBL outcomes [12, 13], with Aunmeungtong [14] reporting less MBL in MDIs than CDI overdentures. Monitoring MBL is crucial for assessing implant performance and identifying complications such as peri-implantitis and implant failure [15]. Therefore, optimizing MBL outcomes is essential for the long-term success of MDI overdentures.
Beyond MBL, survival rates, bite force, and prosthetic maintenance influence MDIs’ efficacy. While MDIs offer a cost-effective and minimally invasive alternative for edentulous mandibles, their limited fatigue fracture resistance restricts them to removable prostheses [16, 17]. A systematic review by Jawad [18] reported a 95.63% survival rate for MDI overdentures, while Schiegnitz [19] found a similar rate of 94.7% for narrow-diameter implants (NDIs). Additionally, MDI overdentures enhance bite force and chewing efficiency, contributing to greater patient satisfaction [20]. Moreover, long-term success also depends on effective prosthetic maintenance to manage wear and retention loss [21, 22].
Overdenture success is influenced by attachment selection, surgical techniques, and implant positioning [23]. Attachment choice depends on intraoral anatomy, cost, retention needs and patient preferences [24–26]. Attachments are broadly categorized as splinted or non-splinted systems [27]. Splinted systems use bars to connect implants, securing overdenture with clips or other components [28, 29]. Non-splinted systems include balls/O-rings, Locator, ERA^®^ (Extra-Coronal Resilient Attachment), magnets, or crowns [30]. Among them, ball attachments remain popular for their simplicity and benefits in distributing loads on implants [31, 32]. Over time, they have surpassed bars due to cost-effectiveness, minimal prosthetic space requirements, and ease of hygiene maintenance [33, 34]. Biochemically, different attachment systems exhibit varying degrees of resilience, influencing stress distribution and peri-implant bone adaptation, particularly in the critical first year of loading [35–41]. Therefore, understanding whether attachment design impacts MBL in MDIs is essential.
While conventional implant studies suggest that attachment type does not significantly affect peri-implant bone resorption [42, 43], its impact on MDIs remains unclear due to their unique biomechanics. Most systematic reviews on MDIs primarily compare them to standard-diameter implants, focusing on survival rates, bone loss, and patient satisfaction, but often overlook variations in attachment mechanisms. For instance, Lemos’ review evaluated MDIs for complete overdentures but did not investigate differences in attachment designs [44]. Similarly, Borges’ review compared MDIs to standard implants regarding complications and clinical outcomes but did not specifically address attachment variations within MDIs systems [45]. Therefore, this systematic review aims to fill this gap by assessing the influence of ball attachments versus other systems on clinical outcomes, including MBL, bite force, implant survival, prosthetic maintenance, and complications in MDI-supported overdentures.
Materials and methods
This systematic review was conducted in adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [46, 47]. This review’s protocol was registered in PROSPERO under the registration number CRD42024610018. The objective of this review was to compare the ball attachment with other attachment systems in MDI overdentures. Eligible study designs included randomized controlled trials (RCTs), controlled clinical trials (CCTs) or comparative retrospective or prospective cohort studies with a minimum follow-up period of one year.
Following the Centre for Evidence-Based Medicine guidelines, the PICO framework was used to formulate the research question: “In edentulous individuals requiring mandibular mini implant-retained overdentures (P),* how does the use of ball attachments (I) compare to other attachment systems (C) influence marginal bone loss (MBL), maximum bite force*,* implant survival rate*,* prosthetic maintenance and complications (O)?”*
Population (P)
Individuals in optimal overall health with an edentulous mandible necessitating the placement of MDI overdentures.
Interventions (I)
Ball attachments used in MDI overdentures.
Comparison (C)
Other attachments rather than ball attachments used in MDI overdentures.
Outcomes (O)
The primary outcome was marginal bone loss.
Maximum bite force, survival rate, prosthetic maintenance and complications were the secondary outcomes.
Time (T)
Studies with a minimum follow-up period of one year.
Study design (S)
Randomized controlled trials (RCTs), controlled clinical trials (CCTs) and comparative retrospective or prospective cohort studies.
Search strategy
A comprehensive literature search was performed using three electronic search platforms: PubMed, Scopus and Cochrane Library. The search was conducted up to February 25th, 2025, to ensure the inclusion of the most recent studies. No restrictions were applied regarding language, publication year, or study type. Both free-text keywords and Medical Subject Headings (MeSH) terms were utilized to maximize the retrieval of relevant studies.
The search technique was designed in accordance with each database and constructed according to the PICO approach as shown in Table 1. Additionally, manual searches were conducted on the reference list of included studies and the relevant systematic reviews related to MDIs for possible additional studies. Moreover, an additional search was implemented in Google Scholar for the analysis of grey literature with the purpose of minimizing publication bias.
Finally, the screening and search terms were performed using a Boolean combination of the following terms; (mini-implant* OR “mini dental implant*” OR “mini implant*”) AND (overdenture* OR “over denture*” OR over-denture*) OR (“complete denture*” OR “full-lower denture*” OR “full lower denture*”) AND (attachment* OR attach* OR “precision attachment*”) OR (ball* OR bar OR magnet* OR splint* OR telescopic OR " double crown*” OR locator* OR equator*) AND (“clinical outcome*”) OR (“marginal bone loss*”)) OR (“maximum bite force*”) OR (“implant survival rate*”) OR (“prosthetic maintenance and complication*”) AND (“Mandible“[Mesh]).
Table 1. Construction of search terms according to PICO formatPatient(mini-implant* OR “mini dental implant*” OR “mini implant*”) AND (overdenture* OR “over denture*” OR over-denture*) OR (“complete denture*” OR “full-lower denture*” OR “full lower denture*”) AND (“Mandible“[Mesh])Intervention and comparison(attachment* OR attach* OR “precision attachment*”) OR (ball* OR bar OR magnet* OR splint* OR telescopic OR " double crown*” OR locator* OR equator*)Outcome(“clinical outcome*”) OR (“marginal bone loss*”)) OR (“maximum bite force*”)) OR (“implant survival rate*”) OR (“prosthetic maintenance and complication*”)
Study selection
Inclusion criteria
- Randomized controlled trials (RCTs), controlled clinical trials (CCTs), comparative retrospective or prospective investigations, or cohort studies with adult human participants who wear mandibular overdentures retained by MDIs.
- Studies at least a follow-up of 1 year.
- Research that had been written in English.
- Outcomes reporting details about marginal bone loss, survival rates, maximum bite force, prosthetic maintenance and complications with various attachments in a mini dental implant mandibular overdenture.
Exclusion criteria
- Research investigated partial removable prostheses supported by implants.
- Studies that specified dental implants over 3 mm in diameter.
- Studies including mini-implant overdenture attachment in the maxillary arch.
At first, a systematic review software application (Rayyan Web) [48] was employed to eliminate duplicate entries. Two investigators (Z.H., P.P.) independently examined the headings and abstracts of every research study gathered through computerized searches. The full text was gathered for papers that satisfied the inclusion criteria or lacked sufficient information upon abstract review for offering a definitive judgment. Two investigators (Z.H., P.P.) independently assessed an in-depth paper obtained from several electronic and alternative search methodologies to ascertain if the studies fulfilled the eligibility criteria. Conflicts were resolved through discussion. A third investigator (P.K.) was consulted when a resolution could not be attained.
Data extraction
Systematic data extraction from the included reports was conducted, and two assessors (Z.H. and P.P.) independently verified the data. In the event of discrepancies during the extraction process, a third assessor (P.K.) was consulted, and resolution was achieved through consensus discussion. Peri-implant marginal bone loss or change (MBL) was the primary outcome. Secondary outcomes were implant survival rate and maximum bite force, prosthetic maintenance and complications.
The following data were collected from the included full-text studies:
- The first author’s name and the publication year.
- Research design.
- Number and age of individuals taking part.
- Dimension, length and manufacturer of inserted MDIs.
- Kind of attachment.
- Type of loading.
- Radiographic method.
- Duration of follow-ups.
- Outcomes.
Quality assessment
The risk of bias was evaluated utilizing the Cochrane Risk of Bias Assessment Tool 2 (RoB 2.0) [49]. The initial author (Z.H.) assessed the selected papers, while the second author (P.P.) then examined any divergent viewpoints about those works. The resultant evaluations were classified according to study methodologies as “Low risk,” “Some Concerns”, or “High risk” of bias, as seen in the following domains:
- Bias arising from the randomization process.
- Bias due to deviations from intended interventions.
- Bias due to missing outcome data.
- Bias in the measurement of outcome.
- Bias in the selection of the reported result.
Studies classified as low risk demonstrated a well-defined randomization process, a clearly described intervention with minimal or no deviations, and little to no loss of follow-up. Additionally, they included appropriate, transparent measurement and reporting of outcomes. If any of these criteria were not fully met, the study was considered to have some concerns or a high risk of bias, depending on the level of uncertainty. The RoB 2 Excel tool was used to evaluate the overall risk of bias for each study, incorporating the reviewer’s critical judgment.
Data analysis
The meta-analysis was conducted by Z.H. and T.S. by utilizing RevMan (version 5.4) [50]. Means and standard deviations (SD) for marginal bone loss (MBL) and maximum bite force (MBF) were extracted from the studies included in the analysis. If a study reported MBL at multiple sites (mesial, distal, buccal, lingual), the overall mean was calculated, and the SD was pooled. When only an average value was provided, it was directly used for data analysis.
MBL data analysis
Three studies done by Jofre [54], Ghoneim [58], and Badr [59] measured MBL at multiple implant sites but provided an average MBL value, which was used directly in the analysis. Jofre reported a single averaged value, Ghoneim provided both site-specific and averaged values (with the latter used), and Badr reported only an averaged MBL value.
The fourth study, conducted by Borges & Shoeib [57], measured MBL at four implant sites but did not provide an overall mean or SD. To obtain these values, the mean was calculated by averaging the four site-specific values, and the pooled SD was determined using the pooled standard deviation formula to account for variability across sites.
For consistency with the inclusion criteria of a minimum one-year follow-up, the data at 15 months were taken from the Jofre study [54], while the data at 12 months were extracted from the Ghoneim [57], Borges [58], and Badr [59] studies. This ensured uniformity in the follow-up period across studies.
MBF data analysis
For the analysis of maximum bite force (MBF), the means and SD from each study were directly utilized. Data were extracted based on the study’s inclusion criteria, which required a minimum follow-up of one year. Specifically, for Jofre et al. [55], the data at 15 months were selected, as it was the closest follow-up time to one year. For Ghoneim et al. [58], data at 12 months were used. While both studies measured MBF at multiple time points, only the data corresponding to the one-year follow-up were included to align with the study’s inclusion criteria.
Heterogeneity and statistical methods
To compare the ball attachment group with other attachment types, weighted mean differences (WMDs) with 95% confidence intervals (CIs) were calculated for these continuous outcomes. The I² index was used to assess heterogeneity, which reflects the percentage of variability in the results due to heterogeneity rather than chance. The following thresholds were used to interpret I² values: 25% for low heterogeneity, 50% for moderate, and 75% for high heterogeneity [51].
The results were derived using either a fixed-effect model or a random-effects model depending on the heterogeneity. A random-effects model was used when the I² value was 50% or higher, or when clinical heterogeneity (e.g., different measurement methods or follow-up durations) was present. A fixed-effects model was applied when no significant statistical or clinical heterogeneity was detected. Specifically, for marginal bone loss (MBL), a random-effects model was selected due to high statistical heterogeneity (I² = 99%), indicating substantial variability among studies. For maximum bite force (MBF), although statistical heterogeneity was low (I² = 23%), a random-effects model was applied due to notable clinical differences in measurement methods and follow-up durations among studies. A p-value of < 0.05 was considered statistically significant. Forest plots were created to visually represent the meta-analysis results.
Subgroup analysis
Subgroup analysis was performed to explore how different attachment types used in mandibular MDI-retained overdentures might influence the overall effect estimate. This analysis aimed to determine whether specific attachment types contributed to variations in the overall outcomes.
Certainty of evidence
Utilizing the GRADE system [52], which distinguishes evidence quality as “high,” “moderate,” “low,” or “very low,” the evidence’s degree of certainty was assessed. This assessment is based on a variety of factors, including risk of bias, imprecision, inconsistency, and indirectness. The GRADEpro software was employed to generate a table that summarized the quality of the evidence [53].
Results
Search outcomes
A total of 561 articles were identified through searches across three databases. Duplicate citations were subsequently removed, leaving 524 studies for further evaluation. A thorough assessment of the abstracts led to the exclusion of 491 additional articles, resulting in 33 studies being considered for full-text review. After screening the full texts, three studies met the inclusion criteria, while 30 studies were excluded. Additionally, one study was selected from the reference lists of the included studies, and two studies were identified through Google Scholar. A total of six studies were determined to be appropriate for inclusion, with five studies suitable for quantitative analysis. All the included studies were randomized controlled trials. No eligible controlled clinical trials (CCTs) or comparative cohort studies were identified. The research selection process, conducted in accordance with PRISMA guidelines, was outlined in Fig. 1.
Fig. 1PRISMA 2020 flow diagram illustrating the outcomes of the process
Study characteristics
Six studies were eligible to be included [54–59] as shown in Table 2. All six included studies were randomized controlled trial designs. The initial three studies were authored by the same individual in the same publication year on the same population; however, all were considered due to their distinct outcomes: the first Jofre’s study [54] addressed marginal bone loss, the second study [55] examined maximum bite force, and the third investigated MDIs survival rate [56]. Therefore, the likelihood of data overlapping may be diminished.
Table 2A brief description of the included MDI studiesStudy name & typeNumber of patients& ageMDI length, diameter & CompanyFollow-upRadiographic MethodType of attachment & loading conditionOutcome ParametersMBL (mm)MBF (N)SR (%)(Jofre et al., 2010) [54]RCT45NRØ1.8 × 15 mmSendax MDI, IMTEC5,10,15, and 24 monthsPeriapicalradiographBall & BarImmediateMBL, At 15 months, Ball = 1.34 ± 1.32 Bar = 0.80 ± 0.58MBF (NR)SR (NR)(Jofre et al., 2010) [55]RCT45NRØ1.8 × 15 mmSendax MDI, IMTEC5,7,10, 15 monthsBall & BarImmediateMBF,At 15 months Ball = 247.5 ± 139.9 Bar = 203.2 ± 76.8SR (NR)(Jofre et al., 2010) [56]RCT45NRØ1.8 × 15 mmSendax MDI, IMTECup to 2 yearsBall & BarImmediateMBL (NR)MBF (NR)SR, At 2 years,Group Bar = 97.8%Group Ball = 90.9%Borg and Shoeib,2021) [57]RCT2055–70 years2.3 mm in diameterSlimline, Dentium, South Korea6,12 monthsCBCTBall & BarImmediateMBL, At 12 monthsBall = 0.69 ± 0.32Bar = 0.85 ± 0.2MBF (NR)SR (NR)(Ghoneim et al.,2021) [58]RCT2055–65 yearsØ2.4 × 13 mmNR12 monthsCBCTBall & TelescopicImmediateMBL, At 12 months Ball = 0.69 ± 0.05 Telescopic = 1.64 ± 0.09MBF, At 12 months Ball = 184.55 ± 6.53 Telescopic = 184.5 ± 7.33SR (NR)(Badr,2022) [59]RCT1660–65 yearsØ2.4 × 13 mmCowellmedi Co., Ltd (Korea)Sterngold ERA^®^ (USA)6,12 monthsCBCTBall & ERA^®^ImmediateMBL, At 12 months ERA^®^= 0.88 ± 0.24 Ball = 0.92 ± 0.21MBF (NR)SR (NR)Pt’s no = patient’s number, MDI = mini dental implant, MBL = marginal bone loss,MBF = maximum bite force, SR = survival rate, mm = millimeter, N = newton, NR = not reported,RCT = randomized controlled trial, CBCT = Cone-beam computed tomography
All studies included follow-up durations minimum of 1 year; two studies [54, 56] had follow-ups of 2 years, one study lasted 15 months [55], and three investigations [57–59] extended up to 12 months. All experiments indicated immediate loading in each case regarding the loading methodology. Concerning the MDIs number, a total of 234 MDIs were distributed to 101 individuals. All studies employed two mini dental implants (MDIs) for the retention of mandibular overdentures, except for one study [59] that utilized four MDIs for denture retention. Four research studies [54, 57–59] provided data on the primary outcome of MBL, two studies [55, 58] offered results for maximum bite force, one study [56] presented findings on MDI survival rate and one [59] evaluated prosthetic maintenance and complications.
Quality assessment
Comprehensive explanations of the risk of bias in the included trials are presented in the “Risk of bias” figures, illustrated in Fig. 2a and b. Of the six selected studies, three exhibited some issues in their results [57–59], whilst three were assessed to have a low risk of bias [54–56]. Due to the experimental character of the studies, it was difficult to blind participants and personnel.
The assessment of bias arising from the randomization process indicates low risk in three studies by Jofre [54–56], as they were conducted with independent allocation and random numbers, with no involvement from the surgeon or prosthodontist in patient assignment. In contrast, the studies by Borg [57] and Ghoneim [58] lacked a clear explanation of their randomization methods. In Badr’s study [59], although software was used for randomization, it did not provide adequate details for a thorough risk evaluation. Regarding bias due to deviations from intended interventions, all studies were considered low risk, as they adhered closely to treatment protocols without noted deviations. The risk associated with missing outcome data was also low across all studies. Three studies [54–56] maintained clear documentation of participant randomization and reported dropouts that occurred in one group while retaining overall clarity on participant follow-up. The other studies [57–59] reported no missing outcome data. In the domain of outcome measurement, all studies were classified as low risk, offering clear descriptions of their measurement methods and demonstrating no significant discrepancies between intervention groups. Lastly, concerning bias in the selection of reported results, three studies [54–56] exhibited low risk by registering their protocols and outcomes on ClinicalTrials.gov, allowing for external verification. Conversely, the remaining studies [57–59] raised uncertainties about reporting bias due to the absence of pre-trial protocols, potentially affecting the comprehensiveness and reliability of reported outcomes.
Fig. 2. Summary of risk of bias (2a) Evaluations of each bias risk criterion for every included study. (2b) Representation of risk of bias as a percentage for each of the included studies in a graphical format
Qualitative synthesis
Regarding marginal bone loss (MBL), four studies assessed changes in bone levels over time using different imaging techniques. Borg & Shoeib, Ghoneim et al., and Badr et al., [57–59] utilized CBCT (Cone-beam computed tomography) to evaluate crestal bone loss at four implant surfaces (distal, mesial, buccal, and lingual). Measurements were recorded at baseline, six, and twelve months, using standardized reference points. Borges & Shoeib [57] reported the highest bone loss at the buccal site and the lowest at the lingual site, with average values of 0.69 ± 0.32 mm for the ball group and 0.85 ± 0.2 mm for the bar group after 12 months. Similarly, Ghoneim et al., [58] documented 0.69 ± 0.05 mm for the ball group and 1.64 ± 0.09 mm for the telescopic crown group after 12 months. Badr et al., [59] reported bone loss values of 0.88 ± 0.24 mm for the ERA group and 0.92 ± 0.21 mm for the ball group in 12 months. In contrast, Jofre et al., [54] measured MBL using standardized periapical radiographs and a digital caliper, assessing bone levels from the first implant thread to bone contact at mesial and distal sites with follow-ups at baseline, five, ten, fifteen, and twenty-four months. At fifteen months, the mean MBL was 1.34 ± 1.32 mm for the ball group and 0.80 ± 0.58 mm for the bar group. Additionally, Jofre et al., [54] classified 51% of MDIs as exhibiting vertical bone loss and 49% as horizontal bone loss, providing further insights into bone loss morphology.
Maximum bite force (MBF) was evaluated in two studies (Jofre & Hamada and Ghoneim [55, 58]). In the Jofre study [55], MBF was recorded using a thin (98 μm) press-sensitive Dental Prescale sheet at baseline (pre-surgical) and at 5, 7, 10, and 15 months. A progressive increase in MBF was observed in both groups over time, with values reaching 247.53 ± 132.91 N for the ball group and 203.23 ± 76.85 N for the bar group at 15 months. Similarly, Ghoneim [58] measured MBF at the molar and premolar regions on both sides using a portable occlusal force gauge. Measurements were taken at baseline, six, and twelve months. A significant increase in MBF was noted across all follow-up periods, with the highest values recorded at 12 months: 184.55 ± 6.53 N for the ball group and 184.50 ± 7.33 N for the telescopic crown group.
Regarding the implant survival rate, Jofre study [56] compared the survival rates of implants in the ball and bar groups over a two-year follow-up period. After two years, one implant failure was recorded in the ball group (1/46), while four implants failed in the bar group (4/44). The corresponding survival rates were 97.8% for the ball group and 90.9% for the bar group.
Prosthetic maintenance and complications were assessed by Badr et al., [59] who compared ball and ERA attachments through monthly follow-ups. The total number of interventions was five in the ERA group and two in the ball group. In the ERA group, interventions included two sore spot adjustments, one relining, and two nylon male replacements. In the ball group, maintenance involved one denture base fracture repair and one nylon cap replacement (Table 2).
Quantitative synthesis/meta-analysis
Marginal bone loss
The following meta-analysis includes four studies [54, 57–59] with a follow-up of not less than 12 months, comparing the marginal bone loss between ball attachments and other attachment types. The comparison of MBL between the ball and other attachment groups yielded a substantial heterogeneity Chi² value of 350.13 (P < 0.00001) and an I² value of 99%. Therefore, instead of the fixed-effect model, DerSimonian–Laird model as a random-effect model was applied. No statistically significant difference of MBL was detected between ball and other attachments (WMD = 0.15, 95% CI– 0.50 to 0.81, p = 0.65). Given the non-significant overall effect, the results suggest that there is no clear preference for ball attachments over other types of attachments based on the included studies. (Fig. 3)
Marginal bone loss- subgroup analysis
According to the different attachments applied in these studies, three subgroups (i.e. ball vs. bar, ball vs. telescopic crown and ball vs. ERA) showed the comparison of average MBL in the subgroups, respectively. In the ball vs. bar attachments subgroup analysis [54, 57], no significant difference was detected between ball and bar attachments. (WMD − 0.15, 95%CI − 0.84 to 0.53, p = 0.66) (Fig. 3).
In ball vs. telescopic attachments [58], a significant difference exists between the two groups, as evidenced by the observation of a statistical significance level of (P < 0.05). After analysing the data from this single experiment on bone loss, it was found that the ball attachment had less bone loss compared to the telescopic attachment (WMD = 0.95, 95% CI 0.90 to 1.00, p < 0.00001) (heterogeneity = not applicable, total MDIs = 40, one study, Z-score = 41.27).
In ball vs. ERA^®^ attachment [59], both groups did not show a significant difference (P > 0.05) when the data from this one experiment was combined (WMD = -0.04, 95%CI -0.15 to 0.07, p = 0.48) (heterogeneity = not applicable, total MDIs = 64, one study, Z-score = 0.71).
Fig. 3. Analysis 1– Comparative assessment of marginal bone loss between ball and bar, ball and telescopic crown, ball and ERA^®^ attachment
Maximum bite force
The following forest plot includes two studies [55, 58] that measure the maximum bite force of ball attachments versus other attachment types. The heterogeneity among the studies is low, as indicated by a Chi² value of 1.31 with 1 degree of freedom (P = 0.25) and an I² value of 23%. It indicates that there is no significant difference in maximum bite force among ball and other attachment types (WMD = -5.29, 95% CI -33.46 to 22.87, p = 0.71) (Fig. 4).
Fig. 4. Analysis 2– Comparison of maximum bite force between ball and alternative attachments
Certainty of evidence
The level of evidence from the marginal bone was judged to be very low, while the maximum bite force is moderate. The level of evidence for marginal bone loss is low due to several limitations. Risk of bias is a concern, as three out of four studies had unclear randomization. The.
evidence was downgraded as very serious for inconsistency (I² = 99%) and serious for imprecision, as the wide CI (WMD = 0.15, 95% CI − 0.49 to 0.80, p = 0.64) suggests substantial uncertainty. The certainty is rated as very low, and results should be interpreted with caution. For maximum bite force, the evidence is based on two randomised trials. Serious imprecision was noted due to the wide CI (CI = -33.46 to 22.87), indicating uncertainty. With low heterogeneity (I² = 23%), the certainty is rated as moderate, and results should be interpreted with caution. More details on the level of evidence, based on the GRADE criteria, are described in Table 3.
Table 3. Evaluation of the certainty of evidence following GRADE guidelinesCertainty assessment№ of patientsEffectCertaintyImportance№ of studyStudy designRisk of biasInconsistencyIndirectnessImprecisionOther considerationsBallothersRelative(95% CI)Absolute(95% CI) Marginal Bone Loss 4RCTserious^a^very serious^b^not seriousserious^c^none109109-MD 0.15 higher(0.49 lower to 0.8 higher)⨁◯◯◯Very low^a, b,c^CRITICAL Maximum Bite force 2RCTnot seriousnot seriousnot seriousserious^d^none3737-MD 5.29 lower(33.46 lower to 22.87 higher)⨁⨁⨁◯Moderate^d^CRITICAL Note: bold values are the exact same number taken from the forest plots (all figures before) CI: confidence interval; MD: mean difference; RCT: randomized controlled trial Explanations ^a^. Three out of four studies showed potential risk of bias.^b^. Heterogeneity (I² = 99%) in marginal bone loss assessment of four studies.^c^. Wide range of confidence intervals.^d^. Wide range of confidence intervals and small sample size
Discussion
This systematic review and meta-analysis compared clinical outcomes of ball attachments versus other attachments in MDI-retained overdentures, evaluating MBL, maximum bite force (MBF), survival rates, prosthetic maintenance, and complications. Six randomized controlled trials with a minimum follow-up period of one year were included in the qualitative analysis, while five were eligible for quantitative analysis.
The meta-analysis revealed no significant difference in MBL between the ball and other attachment types (bar, ERA^®^, telescopic crowns) in MDI overdentures (P > 0.05). In subgroup analysis, no significant difference in MBL was found between ball vs. bar or ball vs. ERA (P > 0.05), while MBL was significantly lower with ball compared to telescopic crowns (P < 0.05). Nevertheless, the average MBL across all attachment groups was under 2 mm, indicating clinically acceptable levels of bone loss [60].
Included 2 studies in this systematic review comparing ball and bar attachments yielded conflicting results. Jofre [54] reported higher MBL in the ball group, whereas Borg and Shoeib [57] found greater MBL in the bar group. This discrepancy may be due to implant diameter, follow-up duration, and bone density. Study implants (MDIs) differed greatly in diameter. Jofre et al. [54] used narrower Ø1.8 × 15 mm Sendax MDI (IMTEC) implants, while Borg and Shoeib [57] used 2.3 mm Slimline (Dentium, South Korea) implants. As narrower implants are subjected to increased biomechanical pressure, which can increase bone resorption [61], this likely contributed to the differences in MBL across the studies. Follow-up duration also varied, with Jofre’s study spanning 15 months and Borg’s 12 months. While both used immediate loading, differences in observation periods could influence reported bone loss. Additionally, neither study provided details on bone density, a crucial factor affecting implant stability and MBL [62]. Variations in bone quality could have contributed to the observed differences in outcomes. Despite these differences, the MBL variation was not statistically significant, supporting evidence that attachment type may not significantly impact MBL. Further research with standardized parameters is needed to confirm these findings.
The certainty of evidence for MBL in this review was rated very low due to a significant risk of bias, high heterogeneity (I² = 99%), and small sample sizes. Consequently, these findings must be interpreted with caution. The uncertainty of MBL is influenced by multiple factors, including implant number, distribution, and design. Among the included studies, only Badr et al. [59] used four MDIs to support overdentures, while Jofre et al. [54], Borg & Shoeib [57] and Ghoneim et al. [58] used two MDIs. This variation in implant number may act as a confounding factor in MBL assessment. Chatrattanarak et al. [63] reported that overdentures supported by two MDIs exhibited less bone loss than those with four MDIs, suggesting that implant distribution influences peri-implant bone remodelling. Similarly, implant design may also contribute to MBL variability. Although all four included studies [54, 57–59] used one-piece MDIs, the implants came from different manufacturers, introducing potential design-related differences that may affect bone response. In the literature, the impact of implant configuration remains unclear. Aunmeungtong et al. [64] found similar stress distributions between one-piece and two-piece MDIs, while Trang et al. [65] observed lower stress levels in one-piece implants, suggesting a potential biomechanical advantage. Therefore, implant design may act as an additional confounding factor in interpreting MBL outcomes. These findings highlight the multifactorial nature of MBL and the need for individualized treatment planning based on patient-specific biomechanical and anatomical considerations.
Regarding maximum bite force (MBF), the certainty of evidence was rated as moderate. The wide confidence interval (CI = -33.46 to 22.87) reflects substantial uncertainty. Although heterogeneity was low (I² = 23%), additional research is required to validate these findings. In statistical analysis, Ghoneim et al. [58] and Jofre & Hamada [55] reported no significant differences in maximum bite force (MBF) between ball and bar or ball and telescopic crown attachments. Both studies observed increased MBF over time as patients adapted to their prostheses; however, methodological differences in MBF measurement (e.g., Dental Prescale sheets in the Jofre study vs. hydraulic pressure gauges in the Ghoneim study) limit the reliability and generalizability of findings.
Regarding survival rates, MDIs demonstrated high success, which is consistent with the findings of Balaji’s study [66], reporting a survival rate of 94.2%. Among the included studies, only one directly compared attachment types, reporting survival rates of 90.9% for ball attachments and 97.8% for bar attachments. Therefore, limited comparative data necessitate further research to assess the impact of different attachment types on survival rates.
When selecting an attachment system, prosthetic maintenance and complications are important considerations. Rosa’s study [67] reported that ball attachment requires less maintenance compared to bar attachments. Similarly, the included study [59] in this review found that ball attachments required fewer interventions than the ERA^®^ attachment, with the ball primarily needing denture repairs and nylon cap replacements, whereas the ERA^®^ group required more frequent adjustments and nylon replacements. These findings suggest that ball attachments may offer advantages in terms of easier maintenance.
Only a few studies met the inclusion criteria for this systematic review. In addition, comparisons were limited to ball vs. bar, ball vs. telescopic crowns, and ball vs. ERA^®^ attachments in MDI overdentures due to the scarcity of available data. Research on other attachment types such as locator, equator, magnetic systems, were mostly case reports or non-controlled studies or comparisons with standard diameter implants using the same attachment type, making them ineligible for inclusion. Small sample sizes in some trials also contributed to the variability in results, as they may lack sufficient statistical power. In addition, heterogeneity in implant diameter, design, length, number, and follow-up duration, along with confounding factors such as patient demographics, occlusal forces, implant positioning, and oral hygiene, may have influenced variability in MBL outcome. Consequently, further well-designed studies with larger sample sizes and longer follow-up periods are needed to validate these findings.
Despite the confounding factors in the analysed studies, MDIs remain a valuable option in prosthodontic rehabilitation, particularly for patients with anatomical, financial, or medical limitations [66, 68]. Moreover, the flapless surgical technique reduces morbidity and recovery time, making MDIs accessible to medically compromised or economically disadvantaged patients [56, 68–74]. Additionally, the immediate loading capability of MDIs allows for same-day prosthodontic rehabilitation, improving patient satisfaction and quality of life [56, 66, 68–72]. While long-term data is still limited, current evidence suggests MDIs achieve satisfactory survival rates.
Within its limitations, this systematic review found no clear superiority among ball, bar, and ERA^®^ attachments in terms of MBL, though telescopic attachments tended to cause more bone loss. However, due to the low certainty of evidence, these findings should be interpreted with caution. No significant differences were observed in maximum bite force between ball, bar, and telescopic crown attachments in MDI overdentures. Given the moderate certainty of evidence, ball attachments may be a suitable choice for MBF. Clinicians should consider factors beyond MBL and MBF, such as patient preferences, ease of maintenance, cost, and oral hygiene when selecting an attachment system for MDI-retained overdentures. Additional long-term research with larger sample sizes is necessary to confirm these findings and further inform clinical decision-making.
Conclusions
Within the limitations of the study, it can be concluded that ball, bar, and ERA^®^ attachments yield similar outcomes in marginal bone loss while telescopic attachments show more statistically significant marginal bone loss (p < 0.05). The type of attachment does not significantly affect maximum bite force.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Laney WR. Glossary of oral and maxillofacial implants. Int J Oral Maxillofac Implants. 2017;32(4). 10.11607/jomi.2017.4.gomi.10.11607/jomi.2017.4.gomi 28708903 · doi ↗ · pubmed ↗
- 2Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P et al. Implant success, survival, and failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent. 2008;17(1):5–15. 10.1097/ID.0b 013e 318167605910.1097/ID.0b 013e 318167605918332753 · doi ↗ · pubmed ↗