Unmasking primary thyroid tuberculosis - A rare but deceptive diagnosis: A case report with review of literature
Areeba Khursheed, Shahbaz Habib Faridi, SyedHasan Harris, Bushra Siddiqui, Mohammad Nafees Ahmad, Ezaz Ahmed

TL;DR
This case report highlights the rare and challenging diagnosis of primary thyroid tuberculosis, emphasizing the importance of considering it to avoid unnecessary treatments.
Contribution
The paper presents a rare case of primary thyroid tuberculosis and reviews literature to emphasize diagnostic challenges and management strategies.
Findings
Thyroid tuberculosis is rare, occurring in 0.1-0.4% of all thyroid diseases.
Clinical signs are nonspecific, leading to potential misdiagnosis as malignancy or other benign conditions.
Fine-needle aspiration cytology is effective for diagnosis, and anti-tuberculosis treatment is typically sufficient.
Abstract
Thyroid tuberculosis is a rare condition, even in regions where tuberculosis (TB) is more common, possibly due to the thyroid gland's relative immunity. Diagnosing thyroid TB can be challenging as the clinical signs are often nonspecific. A 75-year-old male presented with a swelling in the midline of the neck with an abscess in the lower portion of the swelling. Thyroid function tests were normal, and the tuberculin skin test returned positive. USG of the neck showed heterogeneous hypoechoic collection in the left lobe of thyroid, with surrounding inflammation and multiple subcentimetric lymph nodes in right upper, mid and lower jugular region showing necrosis. FNA revealed mixed inflammatory infiltrate predominantly neutrophils with lympho-histiocytic clusters in necrotic background. No signs of tuberculosis were detected in other organs. Based on these findings, primary thyroid…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1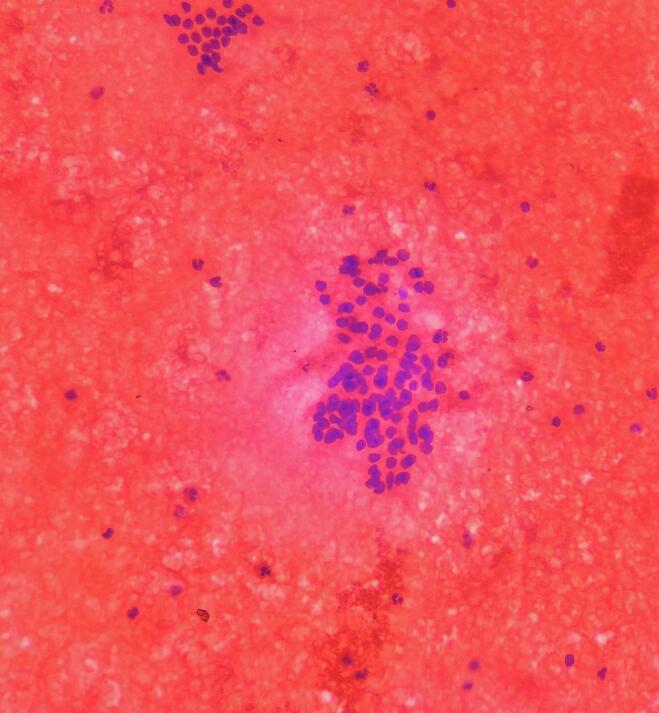 Figure 2
Figure 2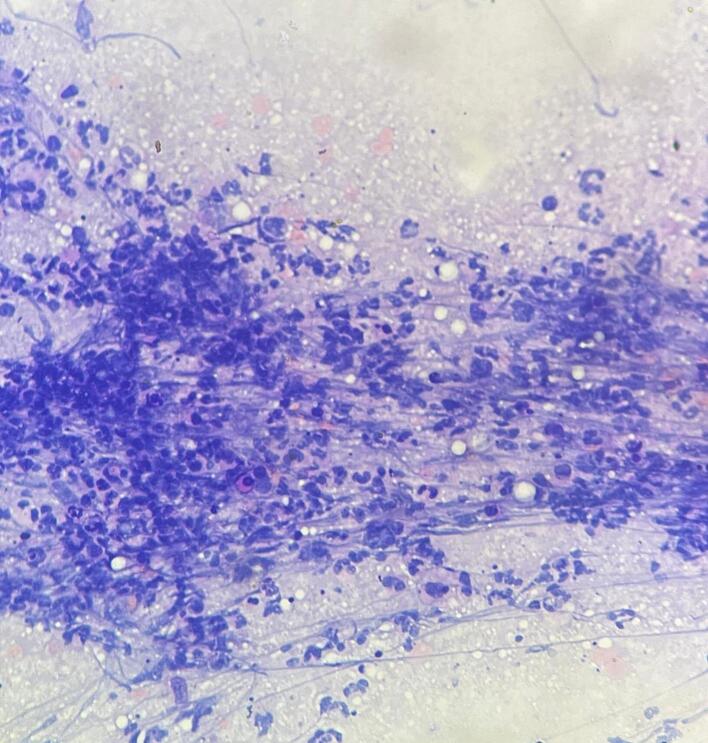 Figure 3
Figure 3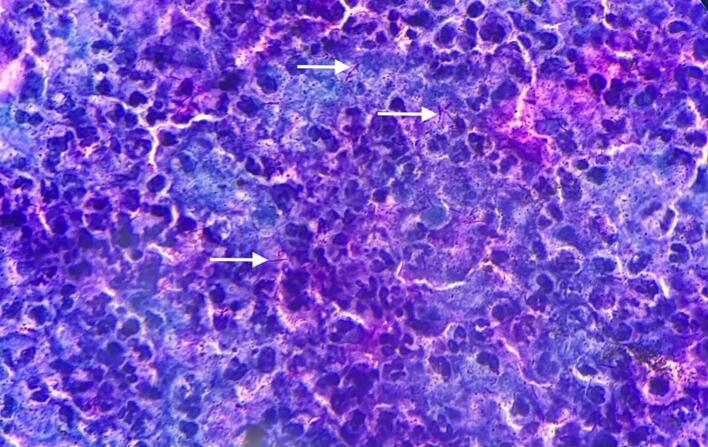 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Anomalies · Thyroid Disorders and Treatments · Thyroid Cancer Diagnosis and Treatment
Introduction
1
Thyroid tuberculosis (TB) is an uncommon condition, even in regions where TB is endemic, accounting for approximately 0.1–0.4 % of all thyroid diseases [1]. Primary involvement of the thyroid by TB is even rarer.
Historically, the thyroid was considered resistant to TB until Lebert's report in 1862, where he described thyroid involvement in disseminated tuberculosis [2]. This rare occurrence is thought to be due to the thyroid's relative immune resistance.
The clinical manifestations of thyroid TB can vary significantly, ranging from asymptomatic to symptoms that may resemble benign or malignant thyroid disorders.
The progression of the disease can also be highly variable, influenced by factors such as thyroid dysfunction and the presence of complications.
While fine-needle aspiration cytology (FNAC) can be used to diagnose thyroid TB, its diagnostic yield is often low. A definitive diagnosis is typically made through histopathological examination, which shows caseating granulomas. Acid-fast bacillus (AFB) staining provides additional support for confirming TB. Due to the potential for misdiagnosis as a malignancy or other benign conditions, maintaining a high index of suspicion is essential to avoid unnecessary treatments, such as total thyroidectomy.
Case report
2
A 75-year-old male from eastern India presented to the outpatient clinic with a midline neck swelling that had been present for four months, accompanied by an abscess in the lower left part of the swelling for the past three months (Fig. 1). The patient did not have any prior history of BCG vaccination. Upon physical examination, a 3 × 3 cm firm, irregular swelling was noted in the midline, with minimal tenderness. The swelling moved with swallowing, and an abscess was observed in the lower left portion of the swelling. No palpable cervical lymphadenopathy was noted, and indirect laryngoscopy revealed no abnormalities.Fig. 1. Clinical photograph showing thyroid swelling with healed abscess.Fig. 1
Blood investigations were done which included a complete blood count, renal function and liver function tests, random blood sugars and serum electrolytes which were normal except for a markedly elevated erythrocyte sedimentation rate (118 mm/h). Thyroid function tests indicated a euthyroid state.
Fine needle aspiration cytology (FNAC) was performed from two distinct areas: (1) the enlarged left thyroid lobe and (2) the base of the abscess. The aspirate from the thyroid contained blood-mixed material, while the abscess yielded a whitish substance. Cytological examination showed normal follicular cells arranged in acinar and papillary formations from the thyroid (Fig. 2) and neutrophils with lympho-histiocytes in necrotic background suggestive of tuberculous etiology, likely of tuberculous origin (Fig. 3).Fig. 2. Fine need aspiration cytology from the left lobe of the thyroid gland showing thyroid follicular cells with blood mixed colloid in the background along with mixed inflammatory infiltrates.Fig. 2. Fig. 3Fine need aspiration cytology from the thyroid abscess showing degenerated and viable neutrophils with lymphohistiocytes in the necrotic background (H&E ×100).Fig. 3
Pus from the abscess was sent for bacteriological culture and Ziehl-Neelsen staining for acid-fast bacilli (AFB), which revealed a high presence of AFB (Fig. 4). X-ray of the chest revealed no abnormalities (Fig. 5). Neck ultrasound revealed a heterogeneous hypoechoic collection (22 × 10 mm) in the left lobe of thyroid, surrounded by inflammation. Multiple small necrotic lymph nodes were observed in the right upper, middle, and lower jugular regions.Fig. 4. Ziehl-Neelsen stain ×100 showing acid fast bacilli (white arrows) and dense inflammatory infiltrates.Fig. 4. Fig. 5Chest x-ray of the patient showing no significant findings.Fig. 5
A Mantoux test using 1 TU of purified protein derivative (PPD) showed a positive result with an induration of 18 mm after 48 h. Other routine investigations, including chest x-ray, USG of the abdomen did not reveal any primary foci of tuberculosis. The patient was started on anti-tubercular therapy with two months of intensive phase (HRZE) followed by four months of continuous phase (HRE). The patient showed complete resolution of symptoms after a six months follow up.
Discussion
3
Tuberculosis of the thyroid gland is an uncommon condition, accounting for only 0.1–0.4 % of all thyroid diseases [1], with primary thyroid tuberculosis being even rarer. This low incidence is attributed to factors such as the gland's high iodine content, the antibacterial properties of colloid, its rich blood supply, the protective thyroid capsule, and the potential antitubercular effect of thyroid hormones [3]. The infection can spread to the thyroid either through hematogenous or lymphatic routes from a distant tuberculosis focus [4].
Barnes and Weatherstone identified two primary forms of thyroid tuberculosis: (1) miliary tuberculosis spread to the thyroid, often from pulmonary or cervical lymph node involvement, and (2) primary thyroid tuberculosis with no identifiable external focus [5].
The presentation of thyroid tuberculosis can vary greatly, ranging from asymptomatic cases to more severe manifestations like multiple diffuse lesions, goiter with caseating necrosis, cold abscesses, acute abscess formation, or chronic fibrosing tuberculosis [6].
In the early stages, thyroid function may remain normal, but later on, patients may develop hypo- or hyperthyroidism [7]. Routine lab tests are typically unremarkable, except for an elevated erythrocyte sedimentation rate. Imaging studies, such as chest X-rays and ultrasound of the abdomen and spine, can help locate any primary tuberculosis focus.
Seed (1944) outlined three essential criteria for diagnosing thyroid tuberculosis [1]:
- 1.Identification of acid-fast bacilli (AFB) in the thyroid tissue.
- 2.Presence of necrosis or abscess formation within the thyroid.
- 3.Evidence of a tuberculosis focus outside the thyroid.
Histological and bacteriological evidence is sufficient for diagnosis, although the third criterion is not mandatory when diagnosing primary thyroid tuberculosis.
Fine needle aspiration cytology (FNAC) under ultrasound guidance and histopathological analysis are considered the gold standard for diagnosing thyroid tuberculosis. FNAC can confirm the diagnosis in up to 73 % of cases [8]. The cytological patterns of tuberculous thyroiditis are categorized into three types [1]:
- •Type I: Epithelioid granuloma without necrosis,
- •Type II: Epithelioid granuloma with necrosis,
- •Type III: Necrosis without granuloma.
Treatment typically involves anti-tuberculosis medications, while surgery is reserved for cases requiring drainage of large thyroid abscesses or partial thyroidectomy for significant gland involvement.
Conclusion
4
Although thyroid tuberculosis is uncommon, it should be considered as a potential diagnosis for thyroid masses, especially in regions where tuberculosis is prevalent. A history of prior tuberculosis, the presence of cervical lymphadenopathy, and an elevated erythrocyte sedimentation rate (ESR) can support the diagnosis, but thyroid tuberculosis can still occur without these signs. Fine-needle aspiration cytology (FNAC) is an effective diagnostic method. Treatment typically involves anti-tuberculosis medications, but drainage may be needed for large abscesses, and thyroidectomy might be required if the FNAC results are inconclusive. Follow up with neck ultrasound and chest x-ray is essential to ensure complete recovery after completion of antitubercular regimen.
The work has been submitted in line with the SCARE criteria [9].
CRediT authorship contribution statement
Concept and design: Shahbaz Habib Faridi, Md Nafees Ahamad, Syed Hasan Harris.
Acquisition, analysis and interpretation of data: Areeba Khursheed, Ezaz Ahmed, Bushra Siddiqui.
Drafting of the manuscript: Areeba Khursheed, Ezaz Ahmed.
Critical review of the manuscript: Shahbaz Habib Faridi, Bushra Siddiqui.
Supervision: Shahbaz Habib Faridi, Md Nafees Ahamad, Syed Hasan Harris.
Consent
Written consent was taken from the patient and may be obtained as per requirement.
Ethical approval
Ethical approval was exempted from the ethical committee.
Guarantor
I, Areeba Khursheed, corresponding author of the case report take full responsibility for the work and conduct of the study.
Funding
No funding procured.
Research registration
Not applicable.
Declaration of competing interest
The authors have declared that no competing interests exist.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ghosh A.Saha S.Bhattacharya B.Chattopadhay S.Primary tuberculosis of thyroid gland: a rare case report Am. J. Otolaryngol.2820072672701760604510.1016/j.amjoto.2006.09.005 · doi ↗ · pubmed ↗
- 2Chacko A.Ajaykumar K.Geetha C.G.‘Primary thyroid tuberculosis’- the masquerader: a case report Indian J. Otolaryngol. Head Neck Surg.74Suppl. 32022 S 5436 S 543910.1007/s 12070-021-02736 PMC 989535036742529 · doi ↗ · pubmed ↗
- 3Pachipala M.Aiyappan S.Two interesting cases of thyroid gland tuberculosis Cureus 1620241610.7759/cureus.68733 PMC 1145328639371708 · doi ↗ · pubmed ↗
- 4Baidya A.Singha A.Bhattacharjee R.Dalal B.S.Tuberculosis of the thyroid gland: two case reports Oxf. Med. Case Rep.2015201526226410.1093/omcr/omv 028PMC 466483926634141 · doi ↗ · pubmed ↗
- 5Thirunavukkarasu S.Subramanian A.M.A rare case of thyroid tuberculosis Int. Surg. J.5201826792681
- 6Lacka K.Maciejewski A.Rare thyroid non-neoplastic diseases Thyroid. Res.8201552590894110.1186/s 13044-015-0017-3PMC 4407423 · doi ↗ · pubmed ↗
- 7Araújo A.N.Matos T.Boavida J.Bugalho M.J.Thyroid tuberculosis: an unexpected diagnosis BMJ Case Rep.142021 e 23879510.1136/bcr-2020-238795 PMC 789360733597161 · doi ↗ · pubmed ↗
- 8Darre T.Amana B.Pegbessou E.Winga F.Warou D.Napo-Koura G.Tuberculosis of the thyroid in Togo: a clinicopathologic study of 11 presumed cases Trop. Dr.484201831331610.1177/004947551878955530114986 · doi ↗ · pubmed ↗