The Prevalence and Characteristics of Infective Endocarditis in Liver Transplant Recipients: Insights From National Inpatient Sample Database
Ajit Brar, Ayushi Garg, Isha Kohli, Soumiya Ravi, Carol Singh, Aalam Sohal, M Luay Alkotob

TL;DR
This study finds that infective endocarditis is rare in liver transplant recipients but is linked to worse outcomes like higher mortality and longer hospital stays.
Contribution
The study provides the first national analysis of IE prevalence and outcomes in liver transplant recipients using a large inpatient database.
Findings
Infective endocarditis occurred in 0.003% of liver transplant recipients.
Patients with IE had higher in-hospital mortality, ICU admission, and hospital charges.
Staphylococcus and Enterococcus were the most common pathogens in IE cases.
Abstract
Liver transplant (LT) recipients are immunocompromised and thus predisposed to various bacterial and fungal infections, including infective endocarditis (IE). The current paper aims to determine the prevalence, characteristics, and outcomes of IE in LT recipients. The National Inpatient Sample (NIS) data from 2016 to 2020 was used to identify LT recipients. Patients were separated into two groups based on the presence of IE. Information was collected on patient demographics, hospital characteristics, infections, comorbidities, and outcomes. Multivariate logistic regression was performed to assess the impact of IE on outcomes after adjusting for confounding factors. A total of 170 650 patients who underwent LT were identified using NIS data from 2016 to 2020, of which 0.003% had IE. IE group had higher odds of in‐hospital mortality [aOR 2.2 (95% CI 1.07–4.78)], Shock [aOR 2.7 (95% CI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
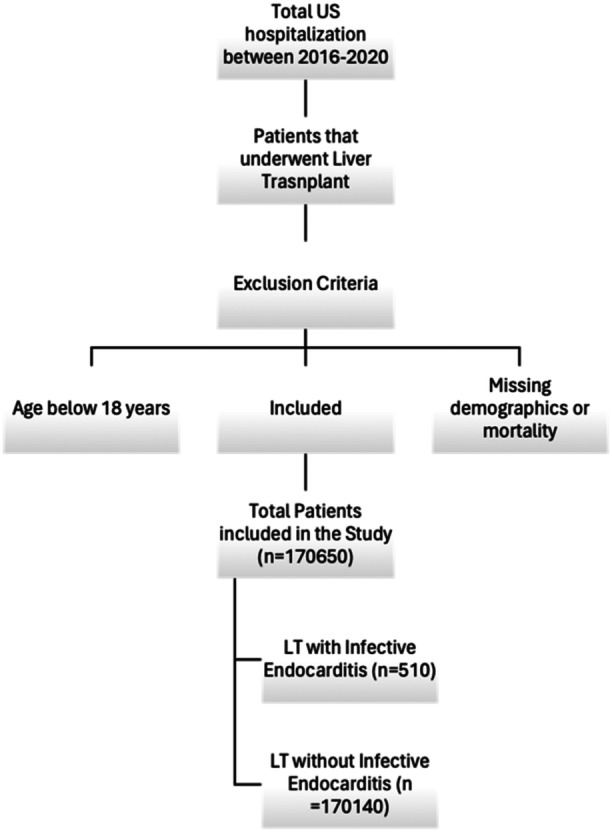 FIGURE 1
FIGURE 1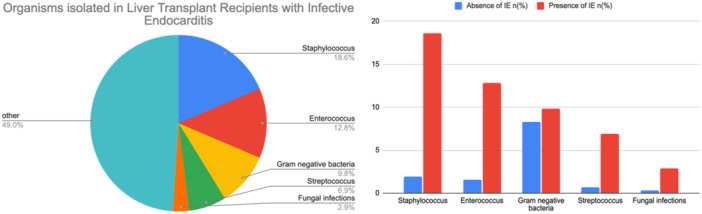 FIGURE 2
FIGURE 2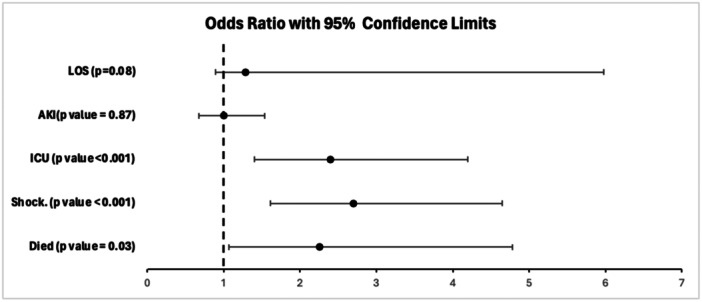 FIGURE 3
FIGURE 3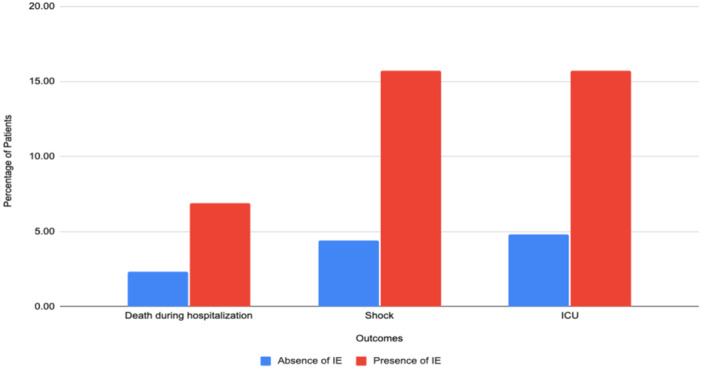 FIGURE 4
FIGURE 4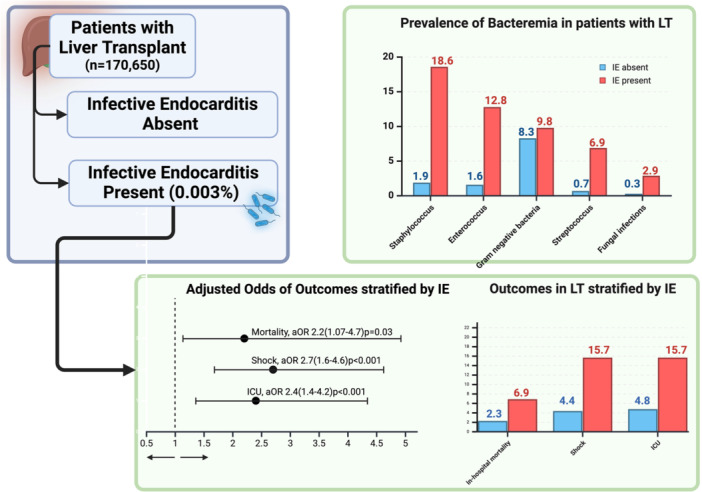 Central_Illustration 1
Central_Illustration 1| Demographics | Absence of IE | Presence of IE |
|
|---|---|---|---|
|
| 0.09 | ||
| 18‐44 | 2250 (13.1) | 35 (6.9) | |
| 45‐64 | 75 615 (44.4) | 215 (42.2) | |
| > 65 | 72 275 (42.5) | 260 (51) | |
|
| 0.03 | ||
| Male | 102 480 (60.2) | 360 (70.6) | |
| Female | 67 660 (39.8) | 150 (29.4) | |
|
| 0.29 | ||
| White | 120 155 (70.6) | 365 (71.6) | |
| African American | 15 605 (9.2) | 75 (14.7) | |
| Hispanic | 23 570 (13.9) | 55 (10.8) | |
| Asian/Pacific Islander | 4645 (2.7) | ** | |
| Native American | 1215 (0.71) | 0 (0) | |
| Other | 4950 (2.90) | 10 (1.9) | |
|
| 0.51 | ||
| Medicare | 104 170 (61.2) | 360 (70.6) | |
| Medicaid | 17 680 (10.4) | 50 (9.8) | |
| Private insurance | 43 380 (25.5) | 95 (18.6) | |
| Uninsured | 1605 (0.9) | 0 | |
|
| 0.74 | ||
| Lowest quartile | 43 965 (25.8) | 140 (27.5) | |
| Second quartile | 44 470 (26.1) | 130 (25.5) | |
| Third quartile | 44 650 (26.2) | 150 (29.4) | |
| Fourth quartile | 37 055 (21.8) | 90 (17.7) | |
|
| 0.36 | ||
| Northeast | 33 600 (19.8) | 85 (16.7) | |
| Midwest | 37 035 (21.8) | 140 (27.5) | |
| South | 65 905 (38.7) | 170 (33.3) | |
| West | 33 600 (19.8) | 115 (22.6) | |
|
| 0.50 | ||
| Rural location | 7315 (4.3) | 15 (2.9) | |
| Urban location | 162 825 (95.7) | 495 (97.1) | |
|
| 0.85 | ||
| Non teaching hospitals | 3485 (17.9) | 95 (18.6) | |
| Teaching hospitals | 139 655 (82.1) | 415 (81.4) | |
|
| 0.71 | ||
| Small | 21 385 (12.6) | 55 (10.8) | |
| Medium | 3305 (22.5) | 130 (25.5) | |
| Large | 110 450 (64.9) | 325 (63.7) |
| Absence of IE | Presence of IE |
| |
|---|---|---|---|
| Prosthetic heart valve | 2330 (1.4) | 25 (4.9) | 0.002 |
| Acute myocardial infarction | 14 040 (8.3) | 60 (11.8) | 0.198 |
| Congestive heart failure | 34 545 (20.3) | 200 (39.2) | < 0.001 |
| Peripheral vascular disease | 9645 (5.7) | 65 (12.8) | 0.002 |
| Cerebrovascular disease | 9065 (5.3) | 80 (15.7) | < 0.001 |
| Dementia | 4045 (2.4) | 15 (2.9) | 0.709 |
| Chronic obstructive pulmonary disease | 29 385 (17.3) | 105 (20.6) | 0.366 |
| Rheumatoid disease | 3295 (1.9) | ** | 0.481 |
| Peptic ulcer disease | 2855 (1.7) | 10 (2) | 0.824 |
| Mild liver disease | 157 350 (92.5) | 480 (94.1) | 0.531 |
| Diabetes without complications | 34 680 (20.4) | 130 (25.5) | 0.199 |
| Diabetes with complications | 51 620 (30.3) | 180 (35.3) | 0.265 |
| Hemiplegia or paraplegia | 2240 (1.3) | 5 (1) | 0.765 |
| Renal disease | 97 295 (57.2) | 360 (70.6) | 0.005 |
| Cancer | 7995 (4.7) | 20 (3.9) | 0.71 |
| Moderate to severe liver disease | 15 930 (9.4) | 35 (6.9) | 0.387 |
| Metastatic cancer | 4740 (2.8) | 15 (2.9) | 0.923 |
| AIDS | 415 (0.2) | 0 | 0.64 |
| Hyperlipidemia | 41 950 (24.7) | 130 (25.5) | 0.846 |
| Smoking | 60 790 (35.7) | 200 (39.2) | 0.472 |
| Alcohol abuse | 15 440 (9.1) | 20 (3.9) | 0.07 |
| Obesity | 20 000 (11.7) | 55 (10.8) | 0.759 |
| ALD | 6400 (3.8) | 10 (2) | 0.339 |
| Hepatitis B | 3330 (2) | 15 (2.9) | 0.473 |
| Hepatitis C | 16 320 (9.6) | 55 (10.8) | 0.68 |
| NASH | 4970 (2.9) | 0 | 0.08 |
| Hepatocellular carcinoma | 1445 (0.8) | 10 (2) | 0.219 |
| Ascites | 11 640 (6.8) | 45 (8.8) | 0.429 |
| Varices | 580 (0.3) | 0 | 0.55 |
| Spontaneous bacterial peritonitis | 820 (0.5) | 15 (2.9) | < 0.001 |
| Hepatorenal syndrome | 1660 (1) | 0 | 0.322 |
| Hepatic encephalopathy | 10 805 (6.4) | 60 (11.8) | 0.026 |
| Absence of IE | Presence of IE |
| |
|---|---|---|---|
| Staphylococcus | 3195 (1.9) | 95 (18.6) | < 0.001 |
| Enterococcus | 2665 (1.6) | 65 (12.8) | < 0.001 |
| Gram negative bacteria | 14 085 (8.3) | 50 (9.8) | 0.57 |
| Streptococcus | 1270 (0.7) | 35 (6.9) | < 0.001 |
| Fungal infections | 540 (0.3) | 15 (2.9) | < 0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Cytomegalovirus and herpesvirus research · Transplantation: Methods and Outcomes
Introduction
1
LT is the only curative treatment available for patients with End‐stage liver disease (ESLD) [1]. Infections and Cardiovascular disease are leading causes of mortality in patients who have undergone Liver transplantation [2, 3]. Impairment of the immune system due to ESLD predisposes these patients to various bacterial and fungal infections [4, 5, 6, 7]. As a result, liver disease is associated with a higher incidence of IE than individuals without liver disease [8]. Furthermore, IE and bacteremia in the setting of immunosuppression correlate with higher mortality [9]. While much is known regarding the prevalence and outcomes of IE in patients with ESLD, similar data regarding outcomes or characteristics in LT recipients is currently sparse.
A significant amount of data on the subject of IE in LT stems from case reports and small case series. To summarize the current literature, Ioannou et al. performed a meta‐analysis of 39 studies and 62 liver transplant recipients [10]. In their study, Loannou et al. observed a mortality rate of 43.5%. Furthermore, 69.4% of mortality was attributed to gram‐positive bacteria, followed by 25.8% to fungal infections [10]. On the other hand, another study of 14 cases of IE in liver and kidney transplant recipients reported mortality to be as low as 4.6%. No nationwide study has comprehensively reported the prevalence, causative organisms, and outcomes of IE in LT recipients [11]. In this study, we used the NIS to assess the prevalence and impact of IE on outcomes in liver transplant recipients (LTR).
Patients and Methods
2
Data Source
2.1
The National Inpatient Sample (NIS), maintained by the Healthcare Cost and Utilization Project (HCUP), is the largest database of inpatient hospital stays in the United States. It contains information on 35 million weighted hospitalizations annually. Information regarding this data source has been discussed in previous studies. Each hospitalization is deidentified and maintained in the NIS as a unique entry with one primary discharge diagnosis and up to 39 secondary diagnoses during that hospitalization, depending on the year of data collection. Each entry carries patient demographics, including age, sex, race, insurance status, primary and secondary procedures (up to 25), hospitalization outcome, total charges, and LOS. IRB approval was not required as this study was conducted on publicly available deidentified data. It collects data from a 20% stratified sample of hospitals in 37 states in the United States and has been reliably used to estimate disease burden and outcomes. NIS contains data on 7 million unweighted and 35 million weighted hospitalizations annually. Each hospitalization is deidentified and maintained in the NIS as a unique entry with one primary discharge diagnosis and up to 39 secondary diagnoses. Each entry carries patient demographics, including age, sex, race, insurance status, primary and secondary procedures (up to 25), hospitalization outcome, total charges, and LOS. IRB approval was not required as it is publicly available deidentified data.
Study Population
2.2
Patients with an index diagnosis of LT were identified using International Classification of diseases‐10th revision (ICD‐10) codes from the National Inpatient Sample (NIS) 2016–2020. We excluded patients with missing demographics/mortality, age < 18 years, or a history of other organ transplants. 170 650 patients were included in the study. The patients were stratified into two groups based on the absence or presence of IE, as presented in Figure 1.
Inclusion flow diagram of the study population.
Study Variables
2.3
Data was collected regarding patient demographics such as age, gender, race, insurance status, income quartile, and hospital characteristics (such as region, bed size, location, and academic status). We also further assessed Charlson comorbidities using the Charlson‐Deyo Comorbidity Index. This is a well‐validated index based on ICD 10‐CM codes meant to be used in large administrative data to predict mortality and hospital resource use. Data regarding decompensations of liver disease was also collected. We also collected data on common infectious causes such as staphylococcus, streptococcus, enterococcus, gram‐negative bacteria, and fungal infection.
Study Outcomes
2.4
The primary outcome of the study was in‐hospital mortality. Secondary outcomes included shock, intensive care unit (ICU), acute kidney injury (AKI), length of stay (LOS), and total hospitalization charges (THC). A patient was considered to have ICU admission if they required mechanical ventilation or vasopressor use.
Statistical Analysis
2.5
National estimates were generated using discharge weights provided by NIS. Categorical variables were compared using the chi‐square, whereas an independent sample t‐test was used for continuous variables. Univariate analysis was done to identify relationships between the study variables and outcomes. To assess the impact of IE on outcomes, multivariate logistic and linear regression analysis was performed by including only those variables that were noted to have p < 0.1 on univariate analysis. A two‐sided p < 0.05 indicates statistical significance, and the result was reported as adjusted ORs (aORs) for categorical variables and adjusted coefficients (adj coeff.) with 95% confidence intervals (CIs) (Tables 1, 2, 3).
Results
3
Baseline Characteristics
3.1
A total of 170 650 patients who underwent LT were identified using NIS data 2016–2020, of which 0.003% had IE. In the IE group, males represented 70.6%, 71.6% were Caucasians and 70.6% had medicare insurance. The IE with LT group had a higher prevalence of congestive heart failure (39.2% vs. 20.9%), peripheral vascular disease (12.8% vs. 5.7%), renal disease(70.6% vs. 57.2%), cerebrovascular disease(15.7% vs. 5.3%) prosthetic heart valve (4.9% vs. 1.4%) Spontaneous bacterial peritonitis (2.9% vs. 0.5%) and hepatic encephalopathy (11.8% vs. 6.4%). In the IE with LT group, the most common causative organisms were staphylococcus (18.6%), enterococcus (12.8%), gram‐negative bacteria (9.8%), and streptococcus (6.9%), as noted in Figure 2a. A complete list of demographic characteristics is presented in Supporting Information S1: Table SI, comorbidities in Supporting Information S1: Table SII, and Organisms identified in Supporting Information S1: Table SIII and Figure S2b.
(a) Organisms isolated in LT with IE (b) Bacterial infections stratified by the presence of IE.
Adjusted odds ratio stratified by the presence of infective endocarditis.
Outcomes stratified by the presence of infective endocarditis.
Outcomes
3.2
In‐hospital mortality‐ The presence of IE was associated with a significantly higher mortality rate of 6.9% compared to 2.3% in LT without IE. Multivariate regression model revealed IE in the LT group had increased odds of mortality [aOR 2.2 (95% CI 1.07–4.78, p = 0.03)] as noted in Figures 3 and 4.
- 2. Shock‐ The presence of IE was associated with a significantly higher rate of shock of 15.7% compared to 4.4% in LT without IE. Multivariate regression model revealed IE in the LT group had increased odds of shock [aOR 2.7 (95% CI 1.61–4.65, p < 0.001)]
-
ICU admissions‐ The presence of IE was associated with a significantly higher rate of ICU admission of 15.7% compared to 4.8% in LT without IE. Multivariate regression model revealed IE in the LT group had increased odds of ICU admission [aOR 2.4 (95% CI 1.4–4.2, p < 0.001)]
- 4. Acute Kidney Injury‐ The presence of IE was associated with a significantly higher rate of AKI of 42.2% compared to 38.2% in LT without IE. The multivariate regression model revealed no significant difference between LT with and without IE groups.
-
Length of stay‐ The presence of IE was associated with a significantly longer length of stay of 10.6 days compared to 5.6 days in LT without IE. The multivariate regression model revealed IE in the LT group had increased odds of shock [adj. Coeff‐ 3.4 days (95% CI 0.89–5.9, p < 0.008)].
- 6. Total hospitalization charges‐ The presence of IE was associated with significantly higher hospitalization charges of 67 997 in LT without IE. The multivariate regression model revealed IE in the LT group had increased odds of shock (adj. Coeff.‐ 14 825–$115 718, p‐0.01).
Discussion
4
The aim of our study was to assess the prevalence of IE in LT in the United States using the national data of hospitalized patients and the most common causative organisms identified. To our knowledge, this is the first national database study to compare the difference between outcomes in LT recipients with and without IE. Our study noted the frequency of IE in LT to be 0.3%. This is slightly lower than a study by Paterson et al. that reported the incidence of IE in LT recipients to be 1.7% in a multicenter study [12]. The incidence in our study is likely lower as this was a cross‐sectional and did not follow patients over multiple hospitalizations. On the other hand, SOT accounts for 1.6%–1.8% of all IE cases. Baral et al. identified SOT in 1.6% of IE cases through the NIS database. However, their study only studied 9 LT patients [13]. Similarly, Martinez‐Selles et al. observed that 1.8% of patients had SOT with IE [11]. and their study included 18 liver transplant recipients. In summary, most data on SOT involve relatively low numbers of LT. Our study is one of the largest studies reporting outcomes in 510 liver transplant recipients diagnosed with IE.
The IE with LT subgroup in our study consisted of 29.4% females. This may be attributed to the ability of estrogen to protect against epithelial damage and mount a stronger response to bacteremia, as demonstrated in various animal models [14] [15, 16]. The IE with LT subgroup demonstrated a higher prevalence of comorbidities, including CHF, PVD, renal disease, CVA, SBP, and hepatic encephalopathy. Furthermore, IE in the LT group had a higher prevalence of prosthetic valves. The higher prevalence of SBP and hepatic encephalopathy in the IE with LT group may be attributed to a predisposition to infections due to decreased protein and immunoglobulin synthesis in ESLD patients [17].
Our study identified causative organisms in 51% of cases of LT with IE. Staphylococcus accounted for 18.6% of all cases, followed by 12.8% enterococcus, 9.8% gram‐negative bacteria, 6.9% streptococcus, and 2.9% fungal (Figure 2a). This is in agreement with the findings of Eichenberger et al. who observed staphylococcal was the most common cause of SOT with IE [18]. Interestingly, the incidence of gram‐negative infection in the LT with IE was higher than that of streptococci (Figure 2b). Moreover, the incidence of gram‐negative bacteria noted in our study is similar to the 9.7% reported by Ioannau et al. [10]. The prevalence of fungal infections in the IE group was 2%. Although rare, fungal endocarditis portends higher mortality and adverse outcomes [19].
LT with IE may be linked with a higher mortality rate in comparison with SOT with IE. A meta‐analysis by Ionnau et al. observed a mortality rate of 43.5% in LT with IE [10]. However, these results should be read cautiously as this meta‐analysis of 62 patients included 28 case reports, which may have confounded the results. In our study, LT with IE exhibited an in‐hospital mortality rate of 6.9% as well as a higher odds of death in comparison with LT without IE (Figure 3). Additionally, this is higher than the 4.6% mortality rate highlighted by Baral et al. in the SOT with IE group [13]. Additionally, our study presented significantly higher rates of shock and ICU admissions in LT with IE group (Figure 4). Finally, a significantly higher LOS and total charges were observed in LT with the IE group. These may be attributed to higher disease severity or the need for further investigation, such as transesophageal echocardiogram or even valvular surgery. This highlights the need to identify these patients earlier during the disease course, thereby preventing IE‐related complications (Central Illustration 1).
The impact of Infective Endocarditis in patients with Liver Transplant needs further inquiry. Analysis of 170 650 patients with LT based on the presence of infective endocarditis was performed. Staphylococcus (18.6%) and Enterococcus (12.8%) were the most common strains identified in patients with IE. Patients with IE had higher odds of in‐hospital mortality, shock, and ICU admission.
We acknowledge the following limitations of our study. We could not obtain access to the immunosuppressive regimen for LT recipients. We could not ascertain if the etiological organism would vary based on differences in the regimen. We could not identify causative organisms in 49% of cases of IE with LT. We were also unable to assess the effect of the time from immunosuppressant induction on the distribution of organisms. Furthermore, NIS are administrative databases that rely on the accuracy of coders. In addition, they lack clinical information on lab investigations, imaging, pharmacotherapy, and compliance. Finally, NIS is a cross‐sectional database that collects data during a single admission. Despite these limitations, the strength of our study is its large sample size, which limits the possibility of bias, which in turn imparts added validity to our conclusions. Inference may favor association analysis, and further studies may be warranted to establish causation.
Conclusion
5
Staphylococcus was present in 18.6% versus 1.9%, followed by enterococcus in 12.8% versus 1.6%, streptococcus in 6.9% versus 0.7%, and fungal infections in 2.9% versus 0.3% in the IE with LT group compared with IE without LT. Concomitant IE and LT were associated with increased in‐hospital death, ICU stay, and shock. The IE group was also associated with increased LOS and total charges compared to the LT without IE. Our study provides comparative insights that underscore the need for early identification and tailored management by recognizing the unique clinical profiles among patients with IE and LT. Further research is needed to evaluate the characteristics of attributable organisms for IE in LT recipients.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Supplementary Table I. Patient demographics and hospital characteristics stratified by development of Infective Endocarditis. Supplementary Table II.Underlying Comorbidities seen in patients stratified by development of Infective Endocarditis*‐ Values < 10 were not reported as per HCUP policy. Supplementary Table III‐ Bacterial infections, stratified by the presence of Infective Endocarditis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1N. Jalan‐Sakrikar , T. Brevini , R. C. Huebert , and F. Sampaziotis , “Organoids and Regenerative Hepatology,” Hepatology 77, no. 1 (2023): 305–322.35596930 10.1002/hep.32583 PMC 9676408 · doi ↗ · pubmed ↗
- 2K. D. S. Watt , R. A. Pedersen , W. K. Kremers , J. K. Heimbach , and M. R. Charlton , “Evolution of Causes and Risk Factors for Mortality Post‐Liver Transplant: Results of the NIDDK Long‐Term Follow‐Up Study,” American Journal of Transplantation 10, no. 6 (2010): 1420–1427.20486907 10.1111/j.1600-6143.2010.03126.x PMC 2891375 · doi ↗ · pubmed ↗
- 3N. Shbaklo , F. Tandoi , T. Lupia , S. Corcione , R. Romagnoli , and F. G. De Rosa , “Bacterial and Viral Infections in Liver Transplantation: New Insights From Clinical and Surgical Perspectives,” Biomedicines 10, no. 7 (2022): 1561, 10.3390/biomedicines 10071561.35884867 PMC 9313066 · doi ↗ · pubmed ↗
- 4H. Liu and S. Lee , “Cardiopulmonary Dysfunction in Cirrhosis,” Journal of Gastroenterology and Hepatology 14, no. 6 (1999): 600–608.10385072 10.1046/j.1440-1746.1999.01920.x · doi ↗ · pubmed ↗
- 5E. Tuchendler , P. K. Tuchendler , and G. Madej , “Immunodeficiency Caused by Cirrhosis,” Clinical and Experimental Hepatology 4, no. 3 (2018): 158–164.30324140 10.5114/ceh.2018.78119 PMC 6185932 · doi ↗ · pubmed ↗
- 6T. Gustot , F. Durand , D. Lebrec , J. L. Vincent , and R. Moreau , “Severe Sepsis in Cirrhosis,” Hepatology 50, no. 6 (2009): 2022–2033.19885876 10.1002/hep.23264 · doi ↗ · pubmed ↗
- 7A. Safdar , Principles and Practice of Transplant Infectious Diseases (Springer, 2019), 1173.
- 8S. K. Garg , H. Goyal , I. Obaitan , et al., “Incidence and Predictors of 30‐day Hospital Readmissions for Liver Cirrhosis: Insights From the United States National Readmissions Database,” Annals of Translational Medicine 9, no. 13 (2021): 1052.34422964 10.21037/atm-20-1762 PMC 8339830 · doi ↗ · pubmed ↗