Awareness About the Protection of Children From Sexual Offences Act Among Healthcare Professionals and Their Role in the Care of Child Sexual Abuse Victims
Sameer S Patra, Sindhu Sankaran, Amit Satapathy, Rashmi R Das, Joseph John

TL;DR
This study finds that healthcare professionals in India lack knowledge and proper practices regarding the POCSO Act for protecting children from sexual abuse.
Contribution
The study provides new insights into the gaps in knowledge and practice of the POCSO Act among healthcare professionals in Eastern India.
Findings
Over 60% of participants lacked knowledge about key aspects of the POCSO Act, such as consent age and compensation conditions.
More than 90% of participants did not follow proper procedures for handling CSA cases, like providing first aid or collecting evidence.
Despite poor knowledge and practice, the attitude of healthcare professionals towards CSA victims was generally satisfactory.
Abstract
Introduction: Child sexual abuse (CSA) is prevalent worldwide. Many medical professionals feel uncomfortable or lack the skills required to manage cases of sexual abuse. Objectives: To assess the extent of knowledge, attitude, and practice (KAP) regarding the Protection of Children From Sexual Offences (POCSO) Act 2012 amongst healthcare professionals. Methods: This cross-sectional study was conducted in a tertiary care teaching hospital in Eastern India. After pre-testing, medical professionals were administered a questionnaire containing sections on knowledge, attitude, and practice, including healthcare workers' role in managing CSA victims. Statistical analysis was done using STATA software. Results: Out of a total of 403 medical professionals who participated, in the knowledge category, >60% did not know the age for obtaining consent from the child, the organization interested…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
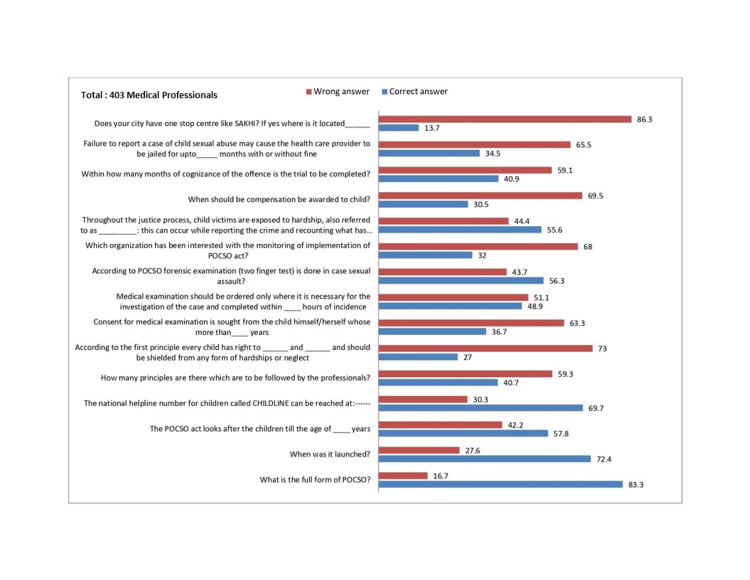 Figure 1
Figure 1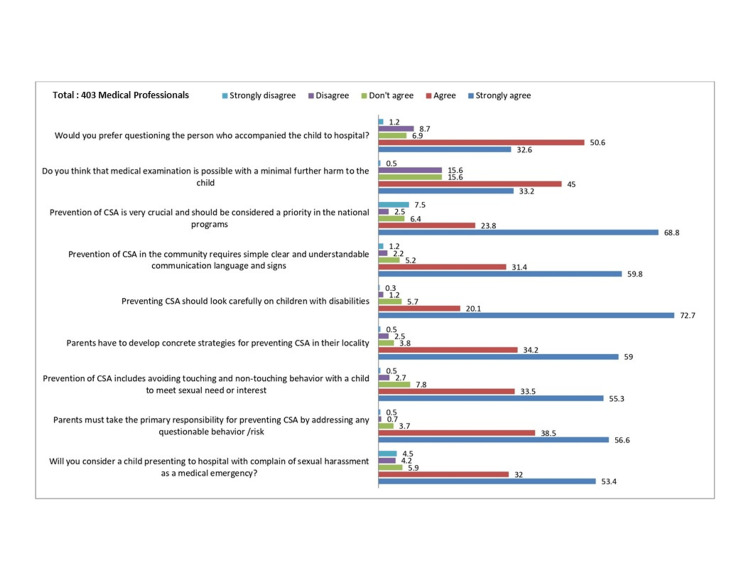 Figure 2
Figure 2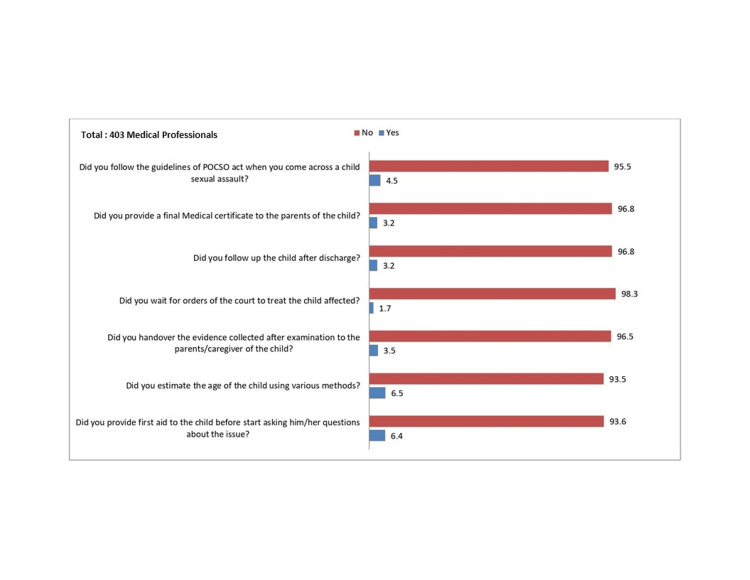 Figure 3
Figure 3| Characteristics | Number (%) | |
| Gender | Male | 227 (56.3) |
| Female | 176 (43.7) | |
| Age (Mean±SD) | Male | 24.64 ±5.9 |
| Female | 23.47± 4.8 | |
| Designation | Undergraduate students | 247 (61.3) |
| Junior resident | 45 (11.2) | |
| Senior resident | 61 (15.1) | |
| Nursing student | 38 (9.4) | |
| Nursing officer | 12 (3.0) | |
| Departments | Pediatrics | 27 (6.7) |
| Obstetrics & Gynecology | 18 (4.5) | |
| Forensic Medicine | 6 (1.5) | |
| Psychiatry | 8 (2.0) | |
| Others | 344 (85.3) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Abuse and Trauma · Migration, Health and Trauma · Ethics and Legal Issues in Pediatric Healthcare
Introduction
Child sexual abuse (CSA), as defined by the World Health Organization (WHO) Consultation on Child Abuse Prevention 1999, is the involvement of a child in a sexual activity that they do not fully comprehend, is unable to give informed consent to, or for which the child is not developmentally prepared and cannot give consent, or that violates the laws or social taboos of society [1]. CSA is a unique entity and cannot be dealt with in the same way as adult sexual abuse victims. Some characteristics of CSA are manipulation of trust rather than using physical force to hide the abuse; the abuser is generally a known person to the child. Intra-familial abuse accounts for about one-third of all CSA cases; it is usually chronic, with repeated episodes happening over weeks to years and the invasive nature escalating over time [2].
CSA is a pressing issue that is increasing in magnitude throughout the world. The prevalence of sexual abuse in the world is estimated to be 7% among girls and 7.9% among boys below the age of 18 [3]. India accounts for the world’s largest population of CSA victims. Many cases fail to be reported due to various socio-cultural factors and taboos, and children are not developmentally sound enough to realize that they are being abused and fear the abuser, who might be a known person or close family member.
CSA has profound adverse consequences on the child’s health, including failure of proper growth and development, poor mental and social health outcomes, relational challenges, substance abuse, and even increased risk of becoming perpetrators of sexual abuse as adults [4-6].
Recognizing the need in India, the Prevention and Protection of Children from Sexual Offences (POCSO) Act 2012 emerged as a comprehensive law to provide for the protection of children from sexual assault, sexual harassment, and pornography while safeguarding and providing child-friendly mechanisms along every step of the judicial process [7]. It also clearly states the role of medical professionals, including proper examination, which causes as little distress to the child as possible.
It is extremely crucial that all healthcare professionals are well aware of the POCSO Act and its guidelines about the responsibilities of medical personnel. There are few studies regarding the awareness of the management of CSA among healthcare workers and none regarding the POCSO Act [8,9]. This study was conducted to determine the extent of healthcare providers' knowledge about the POCSO Act, the management of CSA, and the attitude of medical professionals toward CSA in a tertiary care center.
Materials and methods
This cross-sectional, questionnaire-based (Appendix) study was conducted amongst medical professionals in a tertiary care teaching institute in Eastern India. The study was conducted over four months in the Department of Pediatrics from September 2019 to December 2019. The medical professional included all doctors, including junior residents, senior residents, faculties, medical students, nursing students, and nursing staff. First-year medical and nursing undergraduate students (as they are newly enrolled in the course) and those participating in another study at the same time were excluded.
After ethical clearance, first, a pretest of the questionnaire with a sample size of 30 was done. Each questionnaire consisted of 31 questions: 15 were related to knowledge, nine were related to attitude, and seven were related to practice. All were multiple-choice questions (MCQs). After making the required modifications to the questionnaire, medical professionals were approached with the self-administrable questionnaire containing various sections on knowledge, attitude, and practice (KAP) regarding the various principles of the POCSO Act 2012, including the role of healthcare workers in the management of CSA victims. The study's purpose and procedure for filling out the questionnaire were explained to the participants.
Sample size calculation
Considering that no prior study had been done before, taking 50% as the prevalence of CSA with an alpha level of 5%, the total sample size was calculated to be 400.
Statistical analysis
As this was a qualitative study based on a questionnaire, descriptive statistics were used to present the data. Statistical analysis was conducted using STATA software.
Results
A total of 403 medical professionals participated. There were 227 males (56.3%) and 176 females (43.7%). All the participants responded to all the questions. The characteristics of medical professionals who participated in the study have been described in Table 1.
Around 61% of the participants were undergraduate students, and 26% were residents (junior and senior). Approximately 83% of the participants had some knowledge about child abuse and the POCSO Act. In the knowledge category, >60% did not know about the following: the age for consent from the child, the organization interested in monitoring and implementing the act, when compensation should be awarded to the child, and the punishment if the medical professional fails to report the case under the act as shown in Figure 1.
Knowledge about the POCSO act. The numbers on the top of the bars represent the % of responses (right). The questions are related to knowledge mentioned on the left (total of 403 participants).
The attitude parameters were satisfactory, as shown in Figure 2.
Attitude about the POCSO act. The numbers on the top of the bars represent the % of responses (right). The questions related to attitude are mentioned on the left (total of 403 participants).
In the practice category, >90% did not do the following: provide first aid to the child before asking questions related to CSA, estimate the age of the child, hand over the evidence collected after examination to the parents or caregivers, follow up with the child, or provide a medical certificate to the parents or caregivers when coming across a child with CSA, as shown in Figure 3.
Practice of the POCSO act. The numbers on the top of the bars represent the % of responses (right). The questions related to practice are mentioned on the left (total of 403 participants).
Discussion
CSA encompasses many types of sexual maltreatment of children, including penetrative or non-penetrative sexual intercourse, sexual harassment, sexual exploitation of children for commercial purposes, sex tourism, and pornography [10]. A report by UNICEF tells us that CSA is a global and widespread phenomenon where approximately 4.5% of girls in India between the ages of 15 and 19 have been exposed to sexual violence [11]. These numbers are just a minor reflection of the true numbers, as many cases go unnoticed or unreported due to diverse socio-cultural factors. A survey amongst adolescents in Kerala, India, reported an astounding 36% and 35% of boys and girls who had experienced sexual abuse in their lives [12]. The UNICEF and Indian Medical Association joined hands in 2015 to combat CSA and came up with a teaching manual and 10 key messages to be distributed to more than 2.5 lakh doctors across India regarding the management of CSA as a medical emergency and treatment to be provided free of cost by both government and private hospitals [11].
In the present study, 83.3% of the participants had knowledge about child abuse and the POCSO Act. Whereas in a study done at a tertiary care teaching institute in Chandigarh, this figure was 81% [13]. In a study done in Ahmednagar, Maharashtra, this figure was 72.6% [14]. However, in a study from Chennai, only 45% of the participants were aware of the exact features of the POCSO Act [15]. The discrepancies noted amongst the studies may be related to the participant composition as well as sensitization about the POCSO Act during the course of teaching and training. In the present study, 26% were junior and senior residents, whereas, in the study from Chandigarh, 95% were junior and senior residents (this high number is because it is a post-graduate institute) [13]. The study from Ahmednagar consisted of medical practitioners, whereas that from Chennai consisted of students and interns. Regarding awareness about the age of children up to 18 years included in the act, 57% were correct in the present study and the study from Chennai, but in the Ahmednagar study, it was only 34%. The proportion of participants being aware of the helpline number (1098) and the punishment to be awarded in case of failure to report a case of CSA was nearly the same in the present study and the studies from Chandigarh and Ahmednagar. Awareness regarding the availability of a one-stop center at a respondent’s hospital was present in 70% of the Chandigarh study, in contrast to only 14% in the present study.
In the practice category, the present study showed a very poor response with >90% not adhering to most practice parameters outlined in the POCSO Act 2012. This was in contrast to other studies.
Though the study is unique of its kind as it evaluated all the parameters of the POCSO Act 2012 through a large (403 participants) questionnaire-based survey, it has certain important limitations. First, the risk factors of CSA, which may be useful to inform the government and policymakers, were not evaluated. Second, the findings still may not be generalizable as the proportions of participants in different subgroups were not uniform (undergraduate students form the majority of the respondents).
Conclusions
The present study showed that the knowledge and practice of the POCSO Act among medical professionals were highly unsatisfactory.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization: Report of the consultation on child abuse prevention World Health Organization 3 2025 World Health Organization Geneva.Geneva. 2931 Geneva: World Health Organization 1999 https://iris.who.int/handle/10665/65900
- 2World Health Organization: Guidelines for medico-legal care for victims of sexual violence 3 2025 World Health Organisation Geneva Geneva 75931999 Geneva: World Health Organization 2003 https://iris.who.int/bitstream/handle/10665/42788/924154628 X.pdf?sequence=1
- 3The Journalist's Resource: Global prevalence of child sexual abuse 3 2025 Wihbey J 2011 https://journalistsresource.org/criminal-justice/global-prevalence-child-sexual-abuse/
- 4Child sexual abuse in India: a systematic review P Lo S One Choudhry V Dayal R Pillai D 013201810.1371/journal.pone.0205086 PMC 617717030300379 · doi ↗ · pubmed ↗
- 5Ten-year research update review: child sexual abuse J Am Acad Child Adolesc Psychiatry Putnam FW 2692784220031259577910.1097/00004583-200303000-00006 · doi ↗ · pubmed ↗
- 6Clinical characteristics of children presenting with history of sexual abuse to a tertiary care centre in India Asian J Psychiatr Sowmya BT Seshadri SP Srinath S 44491920162695733710.1016/j.ajp.2015.12.007 · doi ↗ · pubmed ↗
- 7India Code: The protection of children from sexual offences act 2012 3 2025 2013 https://www.indiacode.nic.in/bitstream/123456789/2079/1/AA 2012-32.pdf
- 8Knowledge and attitude in regards to physical child abuse amongst medical and dental residents of central Gujarat: a cross-sectional survey J Indian Soc Pedod Prev Dent Deshpande A Macwan C Poonacha KS 1771823320152615627010.4103/0970-4388.160344 · doi ↗ · pubmed ↗