Plasma Insulin-Like Growth Factor-Binding Protein-2 Levels Predict Severe Septic Acute Kidney Injury: A Mendelian Randomization Analysis
Bozhi Zhao, Zuyi Zhao, Zhengkai Wang

TL;DR
This study shows that high IGFBP-2 levels in blood can predict severe kidney injury in sepsis patients, but there is no direct cause-and-effect link.
Contribution
The study introduces IGFBP-2 as a potential early biomarker for sepsis-induced kidney injury using a Mendelian randomization approach.
Findings
IGFBP-2 alone predicted SA-AKI with high sensitivity and specificity.
Combining IGFBP-2 with clinical scores improved prediction accuracy.
MR analysis found no causal link between IGFBP-2 and AKI.
Abstract
Background: Sepsis-associated acute kidney injury (SA-AKI) currently lacks highly sensitive biomarkers for early detection, resulting in delayed identification and intervention during its early stages and an independent risk of death. Objective: This study aimed to investigate the relationship between insulin-like growth factor-binding protein-2 (IGFBP-2) levels and the occurrence of sepsis-induced kidney injury and to evaluate the causal relationship between the two through Mendelian randomization (MR) analysis. Methods: This study employed a single-center, prospective cohort design involving 79 sepsis patients from the Intensive Care Unit (ICU) at the First Affiliated Hospital of Xinjiang Medical University, Ürümqi, China. The patients were divided into two groups, the SA-AKI group and the non-SA-AKI group, on the basis of whether they developed SA-AKI. The primary endpoint was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
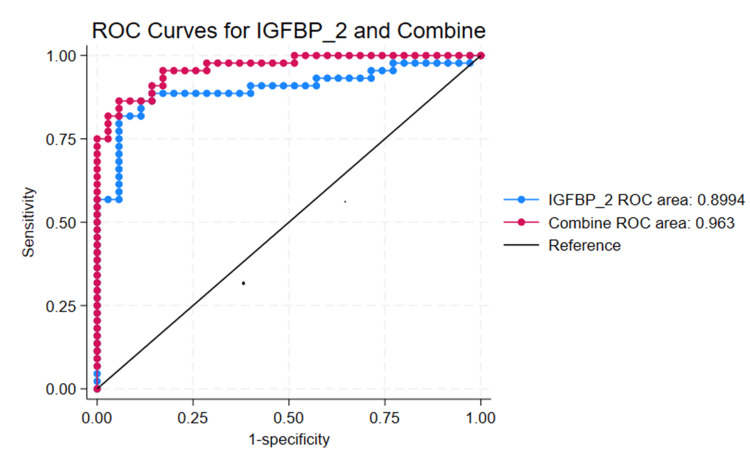 Figure 1
Figure 1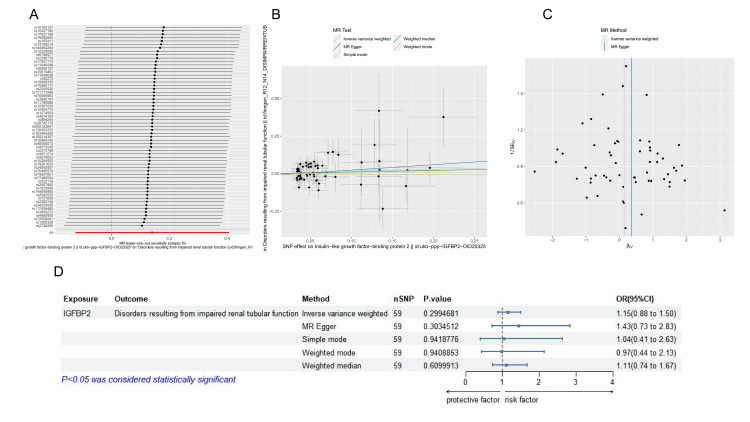 Figure 2
Figure 2| Variables | Without AKI (n = 35) | AKI (n = 44) | t/z | p-value |
| Gender (Male/Female)** | 22/13 | 22/22 | -1.136 | 0.2588 |
| Age (years)** | 59(49,69) | 57.5(47,66.5) | 0.716 | 0.3394 |
| White Blood Cells* | 15.48±0.81 | 17.33±1.14 | -1.2603 | 0.2114 |
| Neutrophil Percentage* | 89.29±0.77 | 89.25±0.92 | 0.0288 | 0.9711 |
| Platelets** | 191(136,241) | 189.6(127.5,234) | 0.143 | 0.8076 |
| Total Bilirubin* | 32.34±6.76 | 36.03±8.19 | -0.3361 | 0.7377 |
| Creatinine* | 85.79±10.38 | 109.43±8.60 | -2.0305 | 0.0783 |
| Bun* | 18.43±4.26 | 21.66±2.53 | -0.6559 | 0.5138 |
| Use of Vasopressors(Y/N)** | 14/21 | 35/9 | -3.575 | 0.0002 |
| Procalcitonin* | 12.63±3.94 | 10.35±3.65 | 0.4229 | 0.6736 |
| Interleukin 6* | 708.16±266.79 | 733.48±217.95 | -0.0742 | 0.9410 |
| Lactate* | 1.87±0.18 | 2.56±0.30 | -1.8548 | 0.0674 |
| Oxygenation Index* | 273.81±13.64 | 251.61±11.73 | 1.2391 | 0.2191 |
| IGFBP-2* | 501.50±38.45 | 1393.62±116.51 | -6.5976 | <0.0001 |
| Length of Hospital Stay* | 14.98±1.44 | 21.68±2.60 | -2.1031 | 0.0387 |
| SOFA Score* | 6.60±0.50 | 8.77±0.49 | -3.0817 | 0.0029 |
| APACHE II Score* | 16.40±0.72 | 19.93±0.89 | -2.9865 | 0.0038 |
| 28-Day Survival Rate* | 0.09±0.05 | 0.18±0.06 | -1.2217 | 0.2255 |
| Urinary Biomarkers | AUC | p value | Cut-off | Sensitivity (%) | Specificity (%) |
| IGFBP-2 | 0.8994 | 0.0374 | 709.004 | 88.64% | 85.71% |
| Combine | 0.9604 | 0.001 | -0.279 | 93.18% | 82.86% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Chronic Kidney Disease and Diabetes · Electrolyte and hormonal disorders
Introduction
Sepsis is a systemic, harmful immune response to infection that can lead to severe acute organ dysfunction caused by infection [1]. Sepsis-associated acute kidney injury (SA-AKI) is a common and serious complication among critically ill patients, resulting in increased morbidity and mortality. The mortality rate of sepsis patients with acute kidney injury (AKI) is significantly greater than that of sepsis patients without AKI [2,3]. The systemic inflammatory response induced by sepsis leads to the release of many inflammatory mediators, which damage renal tubular epithelial cells and interstitial cells. Microcirculation dysfunction and insufficient tissue perfusion further aggravate renal hypoxia, inducing apoptosis and autophagy. Moreover, oxidative stress and mitochondrial dysfunction are also key factors in this pathological process [4]. The increased mortality rate is partly due to the unclear pathogenesis of SA-AKI, the lack of highly sensitive and specific biomarkers for early diagnosis, and the absence of effective specific treatments [5]. However, targeted studies on early inflammatory storms have not been successful. Most sepsis research has focused on the inflammatory process, with less attention given to anti-inflammatory pathways [6]. The insulin-like growth factor (IGF) regulatory pathway is evolutionarily conserved and regulates the growth of almost all organs in the body [7]. In this study, we investigated the ability of insulin-like growth factor-binding protein-2 (IGFBP-2) in the IGF pathway to predict kidney injury caused by sepsis, enabling early detection and intervention. Furthermore, IGFBP-2 has various functions independent of the IGF pathway. This protein can be transported into cells, bind to proteins such as p21, and enter the nucleus to regulate gene expression [8,9].
Previous studies have shown that IGFBP-2 acts as an oncogene and plays an important role in the study of various cancers, promoting processes such as cell proliferation, invasion, and migration [10]. The immune environment in tumors is crucial for tumor development, and IGFBP-2 has shown immunosuppressive effects in glioblastoma [11]. In pancreatic ductal adenocarcinoma cells, IGFBP-2 stimulates the expression of IL-10 [12]. These findings suggest that IGFBP-2 is also involved in immune processes. Some studies have shown that IGFBP-2 levels are correlated with disease severity and prognosis, and patients with higher plasma IGFBP-2 levels have a greater probability of requiring dialysis as the disease progresses [13]. Studies on male rats with acute kidney injury have shown high expression of IGFBP-2 in their renal tissues [14]. Additionally, patients with lupus nephritis, diabetic nephropathy, and chronic kidney disease have been shown to have elevated serum IGFBP-2 levels [8,15]. Therefore, this study aimed to explore the relationship between plasma IGFBP-2 levels and the occurrence of SA-AKI in patients and to investigate whether plasma IGFBP-2 levels can predict the development of SA-AKI.
This study aimed to explore whether plasma IGFBP-2 levels can predict the occurrence of septic kidney injury in critically ill patients by analysing the relationship between plasma IGFBP-2 levels and the development of sepsis-induced kidney injury within 48 hours.
Materials and methods
Study design and participants
This study collected data from January 2024 to January 2025. Plasma samples were obtained from 80 sepsis patients admitted to the intensive care unit (ICU) of the First Affiliated Hospital of Xinjiang Medical University, Ürümqi, China. The patient population consisted of individuals of Asian ethnicity. The study was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (Ethics approval number: K202309-12), and informed consent was obtained from the patients or their family members. Eligibility screening was conducted, and 80 adult sepsis patients with normal renal function who were admitted to the ICU within 24 hours due to sepsis were prospectively included. The development of acute kidney injury (AKI) was tracked over a three-day period in the ICU.
All participants met the diagnostic criteria for Sepsis-3 [16], which included a positive or suspected infection and a sequential organ failure assessment (SOFA) score of 2 or higher. The exclusion criteria included age <18 years, pregnancy or breastfeeding, preexisting kidney disease (e.g., nephrotic syndrome, lupus nephritis, interstitial nephritis, or end-stage renal disease), history of kidney transplantation, malignancy or hematologic diseases, obstructive urinary tract diseases, or a life expectancy of less than 48 hours.
Patients were divided into two groups on the basis of the presence of AKI: the sepsis non-AKI group and the sepsis AKI group. Sepsis patients without AKI were defined as those who did not develop AKI within the first seven days of sepsis, while sepsis AKI patients were defined as those who experienced a sudden and sustained decline in renal function within three days of admission, with an absolute increase in serum creatinine ≥0.3 mg/dL (or ≥26.5 µmol/L), a 1.5-fold increase in serum creatinine from baseline within the past seven days, or a urine output <0.5 mL/kg/h for six hours.
All patients underwent routine medical history recording in the ICU, acute physiology and chronic health evaluation (APACHE II) score, SOFA score, routine laboratory assessments, and plasma IGFBP-2 enzyme-linked immunosorbent assay (ELISA) on the day of ICU admission. Renal artery Doppler and abdominal ultrasound examinations were performed on the day of ICU admission.
Samples and laboratory analysis
Blood samples were obtained within 24 hours of participants enrolling in the study. Plasma was processed within 30 minutes of collection, and samples were stored at -80°C to avoid repeated freeze-thaw cycles. IGFBP-2 levels were determined using an ELISA. Serum samples were diluted 1:200 following the manufacturer's guidelines (Elabscience, Wuhan, China), and standard working solutions were prepared. Standards, blanks, and samples were placed in separate wells. Subsequently, 100 μL of either standard solution, blanks, or diluted serum samples was added to the appropriate wells and incubated at 37°C for 90 minutes. Following this, additional steps such as adding biotinylated antibody working solution, enzyme-conjugated working solution, substrate solution, and stop solution were carried out as per the manufacturer's instructions. Once the reaction was completed, the optical density (OD) of each well was read at 450 nm using a microplate reader.
Clinical data collection
All clinical data, including demographic data (age, sex, SOFA score, and APACHE II score), serum creatinine levels, routine blood parameters, length of stay, use of renal replacement therapy (RRT), and 28-day mortality rate, were extracted from the medical records.
MR analysis
Design of the Mendelian Randomization (MR) Method
MR analysis must satisfy three key assumptions. The first assumption is that genetic variants are significantly associated with exposure. The second assumption is that the genetic variation used as an instrumental variable (IV) for exposure is not correlated with other confounding factors. The third assumption is that the genetic variants affect the outcome only through the exposure and not through other pathways. Our MR analysis adhered rigorously to the principles outlined in the 2023 STROBE-MR Guidelines by Burgess et al. [17]. This study uses an MR design with a two-sample design to explore the causal relationship between serum IGFBP-2 and sepsis-induced kidney injury.
Exposure and Outcome Data Sources
Our data were obtained from publicly accessible genome-wide association study (GWAS) databases [18]. The exposure variable, IGFBP-2, was extracted from the IEU open GWAS project (https://gwas.mrcieu.ac.uk), specifically from study ID ebi-a-GCST90085740, which included a total of 400 participants and 5,188,525 single-nucleotide polymorphisms (SNPs). The outcome variable, tubular damage, was sourced from the FINNGEN database, encompassing a sample size of 340,209 individuals, with the study ID FinnGen R12 N14 DISIMPAIRRENTUB. FINNGEN is a significant GWAS resource that analyzes genomic and health data from around 500,000 participants in Finland [19]. Any samples with missing data will be omitted from this study.
IV Selection
We identified SNPs with a significance threshold of p < 10^-5^ to serve as IVs for the exposure [20]. These SNPs were confirmed to be independent, ensuring they were not in linkage disequilibrium (LD), with R^2^ < 0.001 and an LD distance greater than 10,000 kb. The extracted data for exposure and outcome were merged and harmonized to align the SNP effects on both the exposure and outcome with the same allele. Additionally, we calculated the R^2^ and F-statistics for the selected SNPs, with F-statistics above 10 indicating a strong association. The F-statistic was calculated using the formula: F = R^2^(N-K-1)/(1-R^2^), where R^2^ is the variance in exposure explained by the selected SNPs and N is the number of genetic samples for the phenotype.
MR and Sensitivity Analysis
The main analytical approach employed in this study was the standard inverse variance weighting (IVW) method. To further evaluate the causal relationship between the exposure and outcome, supplementary analyses were conducted using the MR-Egger, weighted median, and maximum likelihood methods. The MR analysis was carried out using R software (version 4.3.1; R Development Core Team, Vienna, Austria), incorporating two-sample MR (version 0.5.7), and MRPRESSO (version 1.0; https://github.com/rondolab/MR-PRESSO). A p-value of less than 0.05 was considered to indicate statistical significance.
To enhance the robustness of the results, we performed sensitivity analyses. We assessed heterogeneity using Cochran's Q test and evaluated horizontal pleiotropy through the MR-Egger intercept test. Scatter plots and funnel plots were utilized to visualize the results, aiding in the identification of outliers and pleiotropy. To ascertain the direction of causality and reduce bias from reverse causality, we employed the Steiger test [21].
Statistical analysis
Statistical analyses were performed via STATA 18 software (StataCorp LLC, College Station, TX) and Statistical Product and Service Solutions (SPSS, version 25; IBM SPSS Statistics for Windows, Armonk, NY). Data that were normally distributed are presented as the mean ± standard deviation (SD), whereas nonnormally distributed data are presented as the interquartile range (IQR). For normally distributed data, t-tests were used, whereas nonparametric tests were used for nonnormally distributed data. Simple linear regression was used for correlation analysis. Receiver operating characteristic (ROC) curve analysis was used to evaluate sensitivity and specificity. A p-value of < 0.05 was considered statistically significant.
Results
Baseline characteristics of the study population
A total of 79 sepsis patients were included in this study, 35 of whom were in the non-AKI group and 44 in the AKI group. The 79 sepsis patients were divided into two groups on the basis of whether SA-AKI occurred: the SA-AKI group and the non-SA-AKI group. The baseline data for the two groups are shown in Table 1. No significant differences were observed between the two groups in terms of age, sex, or 28-day prognosis. In terms of routine examinations, no significant differences were found between the groups. However, the plasma IGFBP-2 concentrations differed significantly (p < 0.05). There was also a significant difference between the two groups in the use of vasopressors within 48 hours (p < 0.05), likely because patients using vasopressors required increased blood pressure to maintain organ perfusion, suggesting worse organ perfusion and a statistically significant probability of SA-AKI. Additionally, significant differences were observed in the APACHE II score and SOFA score (p < 0.05). The length of hospital stays also differed significantly between the two groups, but the 28-day survival rate did not significantly differ.
**Table 1: Characteristics of the patients with sepsis at baseline.Abbreviations: AKI, Acute Kidney Injury; IGFBP-2, Insulin-Like Growth Factor-Binding Protein-2; Sequential Organ Failure Assessment (SOFA) Score, ranging from 0 to 24, with higher scores indicating more severe organ dysfunction; APACHE II, Acute Physiology and Chronic Health Evaluation II; p < 0.05, statistically significantMean ± SD, Median (Q1, Q3)*The variable data follow a normal distribution using the t-test.The variable data do not follow a normal distribution using the rank-sum test.
Diagnostic predictive value of IGFBP-2 for SA-AKI
To evaluate the predictive value of IGFBP-2 for diagnosing SA-AKI, a ROC curve analysis was conducted (Figure 1). Univariate ROC curve analysis revealed that IGFBP-2 alone predicted SA-AKI with an AUC of 0.8994, a cut-off value of 709.004, a sensitivity of 88.64%, and a specificity of 85.71% (Table 2). We subsequently combined the statistically significant features from Table 1 for joint prediction, and the results revealed that combining the IGFBP-2 score with the APACHE II score, the SOFA score, and the use of vasopressors improved the prediction of SA-AKI, with an AUC of 0.9604, a sensitivity of 93.18%, and a specificity of 82.86% (Table 2).
Correlation between plasma IGFBP-2 and septic kidney injury in sepsis patients and the ROC curve for IGFBP-2 in the prediction of SA-AKI.This study investigated the ROC curves for IGFBP-2 and the combined prediction of IGFBP-2 with the APACHE II score, SOFA score, and use of vasopressors for diagnosing SA-AKI and AKI in sepsis patients (sepsis AKI group, n = 35; SA-AKI group, n = 44; IGFBP-2, AUC = 0.8994; combined, AUC = 0.9604).Abbreviations: AKI, Acute Kidney Injury; IGFBP-2, Insulin-Like Growth Factor-Binding Protein-2; SA-AKI, Sepsis-Associated Acute Kidney Injury; Sequential Organ Failure Assessment (SOFA) Score, ranging from 0 to 24, with higher scores indicating more severe organ dysfunction; APACHE II, Acute Physiology and Chronic Health Evaluation II; ROC, Receiver Operating Characteristic
MR analysis
The causal relationship between IGFBP-2 and tubular damage remains unclear. To explore this relationship, MR analysis was conducted. Following predefined screening criteria, 59 SNPs were selected to analyze the causal relationship between IGFBP-2 and tubular damage(Supplementary Table S1). Notably, all the statistical values exceeded 10, indicating that there was no weak instrumental variable bias.
The results from the IVW method, MR-Egger method, weighted median method, and maximum likelihood method were consistent. In the IVW analysis, no causal relationship was found between IGFBP-2 and tubular damage (OR: 1.1507, 95% CI: 0.88-1.50, p = 0.2995).
In the sensitivity analysis, Cochran's Q test revealed no significant heterogeneity (p < 0.05). Various methods, including MR-Egger regression, MR-PRESSO, and funnel plot analysis, revealed that horizontal pleiotropy did not significantly affect the occurrence of SA-AKI through pathways other than the exposure itself (p > 0.05). Furthermore, the leave-one-out analysis additionally ruled out any causal links between exposure driven by individual SNPs and the outcome. We also conducted a reverse MR analysis (Figure 2) using increased kidney injury as the exposure and IGFBP-2 levels as the outcome. The results were not statistically significant (Supplementary Table S2).
MR analysis correlation graph.(A) Forest plot of MR leave-one-out analysis for significant IVW estimates. (B) Scatter plot showing the impact of SNPs on IGFBP-2 and their effect on tubular damage. (C) Funnel plot for the correlation between IGFBP-2 and tubular damage. (D) Forest plot for MR analysis of the effect of IGFBP-2 on tubular damage, including sensitivity analysis, Steiger test, and F-statistic regression results. MR, Mendelian Randomization; SNP, Single-Nucleotide Polymorphism; IGFBP-2, Insulin-Like Growth Factor-Binding Protein-2; IVW, Inverse Variance Weighting
Discussion
The risk of SA-AKI in sepsis patients is high and uneven over time. This necessitates the use of early biomarkers to provide early diagnosis and prognostic information [22]. Currently, serum creatinine (SCr) is commonly used in clinical practice to determine whether SA-AKI has occurred, but it is only a marker of renal insufficiency [23]. An increase in the SCr level is not directly related to renal tubular damage but reflects impaired filtration function, and many factors can lead to an increase in the SCr level [24]. During acute changes in kidney function, the SCr level does not immediately reflect the extent of kidney damage. SCr may not change until approximately 50% of kidney function is lost, and it reflects only renal function once it reaches a stable state, which may take several days [25]. This delay in changes makes early diagnosis and intervention difficult. In male acute kidney injury rat models, the IGFBP-2 protein is highly expressed in kidney tissues [14]. Moreover, patients with lupus nephritis, diabetic nephropathy, and chronic kidney disease have been shown to have elevated serum IGFBP-2 levels [5,12]. Therefore, IGFBP-2 is a potential new biomarker for predicting SA-AKI.
The mechanisms underlying SA-AKI include insufficient renal perfusion, renal vasoconstriction, inflammation, oxidative stress, and nephrotoxicity [26]. Renal Doppler ultrasound can detect impaired blood flow in large and microvascular vessels through these pathways [27]. We designed this study to detect serum IGFBP-2 levels as an early predictor of SA-AKI in critically ill sepsis patients. Our study revealed that sepsis patients with higher plasma IGFBP-2 levels have a significantly greater probability of developing SA-AKI than do those with lower IGFBP-2 levels. The diagnostic AUC of IGFBP-2 for SA-AKI in this study was 0.8994, with a cut-off value of 709.004, a sensitivity of 88.64%, and a specificity of 85.71%. When the APACHE II score, SOFA score, and use of vasopressors were combined, the prediction performance for SA-AKI improved, with an AUC of 0.9604, sensitivity of 93.18%, and specificity of 82.86%. These results indicate that IGFBP-2 is a promising biomarker for predicting SA-AKI. A meta-analysis has summarized the existing biomarkers for predicting SA-AKI, among which C-C motif chemokine ligand 14 (CCL14) and tissue inhibitor of metalloproteinase-2 and insulin-like growth factor-binding protein-7 (TIMP-2 and IGFBP-7) are currently the biomarkers with better predictive performance. The predictive performance was 0.8558 for CCL14 and 0.7563 for TIMP-2 and IGFBP-7 [28]. In this study, IGFBP-2 appeared to perform better; however, this may be due to the higher SOFA scores of the patients selected in this study, as the sample included more critically ill patients.
Our study demonstrated that measuring plasma IGFBP-2 levels in newly admitted patients can effectively predict the occurrence of SA-AKI, suggesting that IGFBP-2 plays a key role in the pathophysiology of SA-AKI. Previous studies have shown that plasma IGFBP-2 levels are positively correlated with dialysis requirements, disease severity, and mortality [13]. Currently, reliable laboratory biomarkers for the early diagnosis of septic kidney injury are still lacking. In these cases, IGFBP-2 may be useful in predicting the risk of severe septic kidney injury. Septicemia due to sepsis does not seem to alter plasma IGFBP-2 levels, and sheep injected with lipopolysaccharide maintained normal IGFBP-2 levels throughout the nine-hour observation period [26]. In humans, IGFBP-2 levels increase by 50% above baseline three hours after endotoxin administration and remain elevated for the next two hours [29]. Therefore, the increase in IGFBP-2 is more related to the progression of sepsis itself than to infection.
To explore the deeper causal relationship between IGFBP-2 and SA-AKI, we performed an MR analysis. The sensitivity analysis using four different MR methods revealed that plasma IGFBP-2 levels do not have a direct causal relationship with the occurrence of SA-AKI. The MR results suggest that plasma IGFBP-2 levels do not have a direct causal effect on septic kidney injury, which does not align with our initial hypothesis. However, as shown in Figure 2(B), IGFBP-2 is a risk factor for acute kidney injury rather than a protective factor, which is consistent with the trend observed in our previous studies [17]. Some studies have suggested that the severity of sepsis itself may influence the expression of plasma IGFBP-2. This result may be because more severe infections and septic shock increase the likelihood of SA-AKI. However, this does not affect the ability of plasma IGFBP-2 levels to predict the occurrence of SA-AKI. While there is no deeper causal relationship, plasma IGFBP-2 levels remain a good predictor of SA-AKI development on the basis of the results of this study. IGFBP-2 may have a complex mechanism in the process of SA-AKI in sepsis patients, but these mechanisms are not yet well understood. However, further studies are needed to clarify these mechanisms.
In this study, MR was performed using a strict genome-wide significance threshold (p < 10^-5^) for SNP selection [20]. The genetic sample libraries used in the study were selected from different populations to minimize confounding factors in genetic studies. Recent studies have shown that septic kidney injury may differ among various ethnic groups, highlighting the importance of diverse populations in research [30]. We also acknowledge other limitations. First, the GWAS sample size was relatively small, which reduced the power to detect causal biomarkers for proteins. In theory, with an increased sample size, more pathogenic protein biomarkers can be identified. Second, our study did not clarify the potential biological mechanisms linking these biomarkers to SA-AKI. Finally, although our study revealed that IGFBP-2 is a predictive biomarker, its clinical benefits (e.g., AUC, nomogram, and decision curve analysis) need external validation.
Our study also exhibits certain limitations as follows:
Lack of direct reflection of renal IGFBP-2: We measured IGFBP-2 levels in the blood, but the kidney may not be the sole source of IGFBP-2. Patients may develop oliguria or anuria after admission, making it difficult to consistently collect urine samples, which prevents urine from being used as the primary study specimen. Renal tissue biopsy, being an invasive procedure, could cause unnecessary harm to patients and was therefore not included in the study protocol.
Single-center design and limited sample size: The single-center design and limited sample size of this study may have introduced potential bias, particularly considering the presence of various comorbidities among the enrolled patients. This may limit the generalizability of our findings. We emphasize the need for larger sample sizes and multi-center studies to validate our results.
Representativeness of population ancestry: Our study faced challenges regarding the representativeness of population ancestry. The MR analysis primarily involved individuals of European ancestry, while the cohort study focused on an Asian population. We recommend further validation in multi-center studies involving diverse ancestral populations to enhance the broader applicability of our conclusions.
Conclusions
IGFBP-2 levels can predict the occurrence of SA-AKI in sepsis patients. However, the results of MR suggest that there is no direct causal relationship between plasma IGFBP-2 levels and septic kidney injury. These results also emphasize the need for further pathophysiological studies and randomized controlled trials to confirm these observations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012 Intensive Care Med Dellinger RP Levy MM Rhodes A 1652283920132336162510.1007/s 00134-012-2769-8PMC 7095153 · doi ↗ · pubmed ↗
- 2Septic acute kidney injury in critically ill patients: clinical characteristics and outcomes Clin J Am Soc Nephrol Bagshaw SM Uchino S Bellomo R 431439220071769944810.2215/CJN.03681106 · doi ↗ · pubmed ↗
- 3Sepsis associated acute kidney injury BMJ Poston JT Koyner JL 0364201910.1136/bmj.k 4891 PMC 689047230626586 · doi ↗ · pubmed ↗
- 4Sepsis-associated acute kidney injury: pathophysiology and treatment modalities Cureus Aguilar MG Al Hussen HA Gandhi PD 016202410.7759/cureus.75992 PMC 1174306039834999 · doi ↗ · pubmed ↗
- 5First post-operative urinary kidney injury biomarkers and association with the duration of AKI in the TRIBE-AKI cohort P Lo S One Coca SG Nadkarni GN Garg AX 011201610.1371/journal.pone.0161098 PMC 499020427537050 · doi ↗ · pubmed ↗
- 6Pro-resolving molecules-new approaches to treat sepsis?Int J Mol Sci Buechler C Pohl R Aslanidis C 4761820172824148010.3390/ijms 18030476 PMC 5372492 · doi ↗ · pubmed ↗
- 7The role of insulin-like growth factor-I and its binding proteins in glucose homeostasis and type 2 diabetes Diabetes Metab Res Rev Rajpathak SN Gunter MJ Wylie-Rosett J 3122520091914558710.1002/dmrr.919PMC 4153414 · doi ↗ · pubmed ↗
- 8Insulin-like growth factor binding proteins in kidney disease Front Pharmacol Wang S Chi K Wu D Hong Q 8071191220213500274010.3389/fphar.2021.807119 PMC 8728008 · doi ↗ · pubmed ↗