Radiotherapy for Large Mucosa-Associated Lymphoid Tissue Lymphoma of the Rectum: A Case Report
Yukihiko Yoshimatsu, Mai Anakura, Munenori Ide, Takuma Ishizaki, Hiroki Kiyohara

TL;DR
A rare case of large rectal MALT lymphoma was successfully treated with radiotherapy, showing no recurrence after 29 months.
Contribution
This case report presents radiotherapy as a potential definitive treatment for large rectal MALT lymphoma.
Findings
Radiotherapy at 39.6 Gy in 22 fractions resulted in complete metabolic response in a patient with large rectal MALT lymphoma.
The patient remained recurrence-free for 29 months post-treatment with no severe adverse events.
Radiotherapy is suggested as a viable treatment option for large rectal MALT lymphomas.
Abstract
Mucosa-associated lymphoid tissue (MALT) lymphomas may arise at various sites, but MALT lymphoma of the rectum is rare. Several treatment options are available for MALT lymphoma of the rectum; however, no standard treatment has been clearly defined. Herein, we report a case of large-sized MALT lymphoma of the rectum that was successfully treated with radiotherapy. The patient presented to the hospital with a complaint of bloody stools and, after a biopsy, was diagnosed with MALT lymphoma of the rectum. Before treatment, the tumor size was 50 × 62 × 70 mm. Radiotherapy was administered at a total dose of 39.6 Gy in 22 fractions, and the patient achieved a complete metabolic response two months after treatment. The patient was followed up for 29 months after radiotherapy, and no recurrence or severe adverse events were observed. This report demonstrates that radiotherapy may be a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
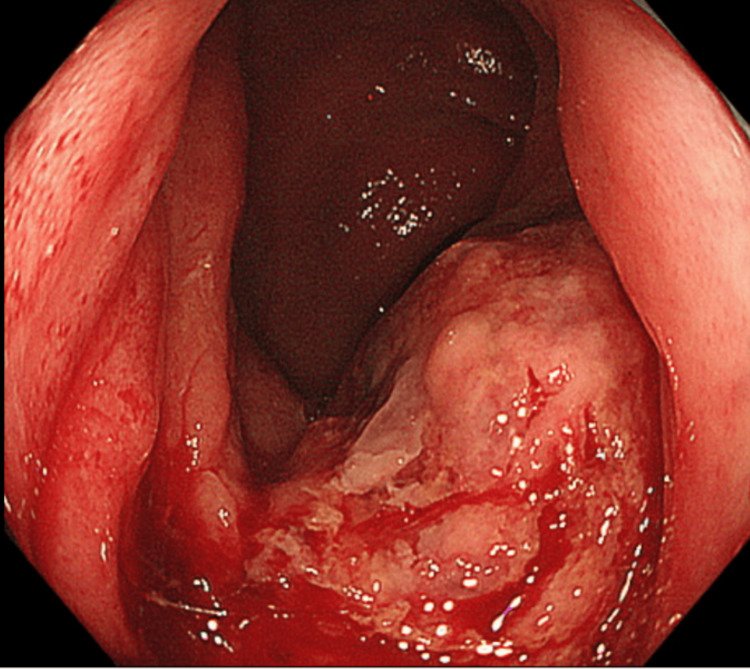 Figure 1
Figure 1 Figure 2
Figure 2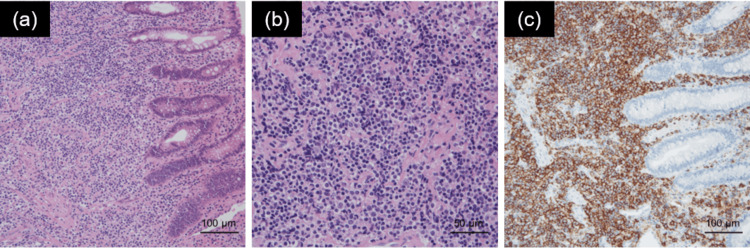 Figure 3
Figure 3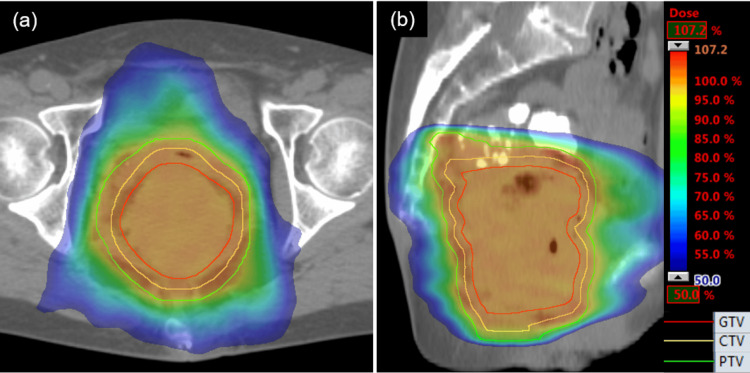 Figure 4
Figure 4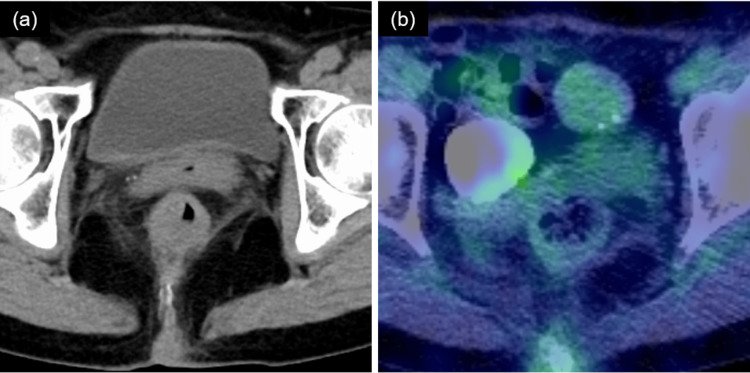 Figure 5
Figure 5| Year | First author (reference) | Age, years | n | Size, mm | Total dose, Gy | Fraction | Outcome | Follow-up, months | Late toxicities |
| 2001 | Tsang [ | NA | 1 | NA | 35 | NA | CR | >48 | None |
| 2008 | Yamashita [ | NA | 1 | NA | 30 | 20 | CR | NA | NA |
| 2008 | Kobayashi [ | 26 | 1 | 100 | 40 | NA | CR | 24 | NA |
| 2008 | Foo [ | 60 | 1 | NA | 45 | 25 | CR | 41 | None |
| 2012 | Okamura [ | 56-65 | 3 | 10-20 | 30 | 20 | CR | 13-75 | NA |
| 2012 | Akasaka [ | 57 | 1 | >30 | 30 | NA | CR | 9 | NA |
| 2017 | Hatayama [ | 28 | 1 | NA | 30.6 | 17 | CR | 9 | None |
| 2017 | Hayakawa [ | 74 | 1 | ≤3 | 30 | 15 | CR | 60 | NA |
| 2020 | Watanabe [ | 38-89 | 4※ | NA | 30 | 15-20 | CR | >60 | None |
| 2022 | Katano [ | 50-67 | 3 | 10-30 | 30 | 15 | CR | 56-59 | None |
| 2023 | Zhang [ | 29 | 1 | NA | 30 | 15 | CR | 3 | NA |
| 2025 | Present case | 76 | 1 | 70 | 39.6 | 22 | CR | 29 | None |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · Colorectal and Anal Carcinomas · Viral-associated cancers and disorders
Introduction
According to the 2022 World Health Organization (WHO) classification, mucosa-associated lymphoid tissue (MALT) lymphoma is classified as a marginal zone lymphoma (MZL) [1]. It arises from MALT, such as the gastrointestinal tract (especially the stomach), ocular appendages, lungs, salivary glands, thyroid, and breast, with the highest frequency in the stomach [2]. Primary lymphomas of the colorectum are rare and account for only 0.2% of all colorectal malignancies [3]. MALT lymphomas of the colorectum account for 1.6% of all MALT lymphomas [4].
Treatment options for primary MALT lymphomas of the gastrointestinal tract excluding the stomach include Helicobacter pylori eradication therapy, surgery, endoscopic mucosal resection (EMR), chemotherapy, radiotherapy, and observation [5]. However, a standard treatment has not been established, and the optimal prescribed doses for radiotherapy have not been clearly defined. Here, we report a case of large-sized MALT lymphoma of the rectum that was successfully treated with radiotherapy.
Case presentation
The patient was a 76-year-old woman who was aware of bloody stools that she had left untreated for one year. At that time, the patient was not aware of B-symptoms. She then went to a local hospital and underwent lower gastrointestinal endoscopy, which revealed a friable 4 cm protruding submucosal tumor on the posterior wall of the lower rectum, 1 cm from the anal verge (Figure 1). The patient was referred to our institution with the suspicion of a malignant tumor. Contrast-enhanced computed tomography (CT) revealed circumferential wall thickening from the lower rectum to the anal canal, and the tumor size was 50 × 62 × 70 mm (Figure 2). Lower gastrointestinal endoscopic and transanal tumor biopsies were performed. Histopathological examination revealed the proliferation of medium- to large-sized bright cytoplasmic lymphocytes, CD20 positivity, no obvious lymphoepithelial lesions, poor monoclonality of kappa and lambda light chain expression, and a low Ki-67 labeling index of 20% (Figure 3). On 18F-fluorodeoxyglucose (FDG)-positron emission tomography (PET)/CT, FDG accumulation was observed with a maximum standardized uptake value (SUVmax) of 20.5 in the tumor on the rectum (Figure 2) and no obvious abnormal accumulation in other parts of the body. Based on these findings, the patient was diagnosed with stage I localized primary MALT lymphoma of the rectum (Lugano classification).
Colonoscopy image before radiotherapy showing an elevated tumor on the posterior wall of the lower rectum, 1 cm from the anal verge.
Images before radiotherapy. (a) Axial view of CT. (b) Sagittal view of CT. (c) Axial view of FDG-PET/CT. SUVmax: 20.5.CT: computed tomography; FDG-PET/CT: 18F-fluorodeoxyglucose-positron emission tomography/CT; SUVmax: maximum standardized uptake value
Pathological findings in the biopsy specimen. (a, b) Proliferation of medium- to large-sized bright cytoplasmic lymphocytes on hematoxylin-eosin staining. (c) CD20-positive specimen. Original magnification: ×200 (a), ×400 (b), and ×200 (c).
Therefore, we decided to treat the patient with radiotherapy. The gross tumor volume (GTV) was delineated using enhanced CT images taken consecutively with the treatment-planning CT. Clinical target volume (CTV) was delineated to the entire rectal mucosal area, including the GTV. The planning target volume (PTV) was delineated by adding a 5-mm margin to the CTV. We used Varian's Clinac iX for treatment. Irradiation was conducted using volumetric modulated arc therapy (VMAT) with a total dose of 39.6 Gy delivered in 22 fractions five times a week (Figure 4). During each irradiation session for image-guided radiation therapy, the spatial reproducibility of the three-dimensional position of the center of irradiation at the time of treatment planning and at the time of irradiation had been confirmed to be within 5 mm by cone-beam CT images in the treatment room. An additional treatment plan CT was performed at the 14th irradiation session, and the tumor size was reduced to 38 × 41 × 63 mm. Consequently, the patient received treatment with a revised plan in the last six sessions.
Images of dose distribution. (a) Axial view of CT. (b) Sagittal view of CT.CT: computed tomography; GTV: gross tumor volume; CTV: clinical target volume; PTV: planning target volume
The bloody stools stopped at 25.2 Gy and did not recur. Adverse events were evaluated using the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. At the end of the treatment, the patient had grade 1 dermatitis, which improved three weeks after irradiation. No other acute adverse events were observed. There were no abnormalities in defecation after treatment. FDG-PET/CT at two months after treatment showed a decrease in SUVmax to 2.5, diagnosed as a complete metabolic response. CT at 20 months after treatment showed no apparent relapse (Figure 5). At the 29-month follow-up after irradiation, the patient was alive with no adverse events.
Images after radiotherapy. (a) Axial view of CT. (b) Axial view of FDG-PET/CT. SUVmax: 2.5.CT: computed tomography; FDG-PET/CT: 18F-fluorodeoxyglucose-positron emission tomography/CT; SUVmax: maximum standardized uptake value
Discussion
Several treatment options are available for MALT lymphoma of the rectum, including Helicobacter pylori eradication therapy, surgery, EMR, chemotherapy, and observation. Radiotherapy is one such therapy, and its effectiveness has been reported in several studies (Table 1) [6-17]. The optimal dose has not been established; however, in these reports, radiotherapy was administered at 30-40 Gy, and in many cases, complete remission was achieved.
MALT lymphoma of the rectum is often observed in small sizes [18], and surgery or EMR is indicated in such cases [5]. Reports of large tumors, such as those in the present case, are rare. Kobayashi et al. reported a patient treated with radiotherapy for MALT lymphoma of the rectum with a tumor size of 100 mm that achieved complete remission after a total dose of 40 Gy [8]. Furthermore, Isobe et al. stated that in their multicenter phase II study for stage IE MALT lymphoma not originating in the stomach, they adopted 36 Gy in 20 fractions for tumors <6 cm and 39.6 Gy in 22 fractions for those ≥6 cm in size; local control and progression-free survival rates were 97.3% and 91.9% at three years, respectively [19]. In addition, the tumor was large and located 1 cm from the anal verge in the present case. If surgery had been performed, surgery would have required a total rectal resection with colostomy as a curative treatment, and the quality of life in this patient would have declined. From the above, we selected radiotherapy owing to the tumor size of >6 cm, with a total dose of 39.6 Gy in 22 fractions, for this patient.
No studies have described the need for changes in treatment plans according to tumor shrinkage during the treatment period. In the present case, we modified our treatment plan once the tumor shrank and changed the plan at the 17th treatment session. We believe that re-planning should be considered for large tumors, as seen in the present case.
MALT lymphoma is classified as an MZL. Histological transformation to large B-cell lymphomas is reported in MZL. The five- and 10-year cumulative incidence of histological transformation was 2.7% and 3.6% [20]. In the present case, the patient had not relapsed at the 29-month follow-up after irradiation. The patient should be followed up with attention to the possibility of histological transformation occurring at recurrence in the future.
Conclusions
There are no clearly defined treatment strategies for MALT lymphomas of the rectum. We treated the patient with radiotherapy as a definitive treatment for large-sized MALT lymphoma of the rectum. The tumor was well controlled, with no severe adverse events during the 29-month follow-up period. This suggests that radiotherapy is an effective treatment option for large-sized MALT lymphomas of the rectum.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms Leukemia Alaggio R Amador C Anagnostopoulos I 172017483620223573282910.1038/s 41375-022-01620-2PMC 9214472 · doi ↗ · pubmed ↗
- 2Survival of patients with marginal zone lymphoma: analysis of the Surveillance, Epidemiology, and End Results database Cancer Olszewski AJ Castillo JJ 62963811920132289360510.1002/cncr.27773 · doi ↗ · pubmed ↗
- 3Primary colorectal lymphomas: review of the literature Surg Oncol Dionigi G Annoni M Rovera F 07116200710.1016/j.suronc.2007.10.02118024019 · doi ↗ · pubmed ↗
- 4Eleven-year experience of low grade lymphoma in Korea (based on REAL classification)Yonsei Med J Hahn JS Kim YS Lee YC Yang WI Lee SY Suh CO 7577704420031458409010.3349/ymj.2003.44.5.757 · doi ↗ · pubmed ↗
- 5Clinical features, treatment and outcomes of colorectal mucosa-associated lymphoid tissue (MALT) lymphoma: literature reviews published in English between 1993 and 2017 Cancer Manag Res Won JH Kim SM Kim JW Park JH Kim JY 857785871120193157201110.2147/CMAR.S 214197 PMC 6759223 · doi ↗ · pubmed ↗
- 6Stage I and II MALT lymphoma: results of treatment with radiotherapy Int J Radiat Oncol Biol Phys Tsang RW Gospodarowicz MK Pintilie M Bezjak A Wells W Hodgson DC Crump M 125812645020011148333710.1016/s 0360-3016(01)01549-8 · doi ↗ · pubmed ↗
- 7Radiotherapy for 41 patients with stages I and II MALT lymphoma: a retrospective study Radiother Oncol Yamashita H Nakagawa K Asari T Murakami N Igaki H Ohtomo K 4124178720081842391410.1016/j.radonc.2008.03.012 · doi ↗ · pubmed ↗
- 8Successful radiotherapy in a patient with primary rectal mucosa-associated lymphoid tissue lymphoma without the API 2-MALT 1 fusion gene: a case report and review of the literature Leuk Res Kobayashi T Takahashi N Hagiwara Y 1731753220081757052310.1016/j.leukres.2007.04.017 · doi ↗ · pubmed ↗