Emergency Physicians’ Perceptions, Knowledge, and Attitudes Toward Family Presence During Resuscitation in the Emergency Department: A Multicenter Survey-Based Cross-Sectional Study
Asseil A Bossei, Hanan A Al Zahrani, Faisal A Bossei, Sufana M Saadi, Ahmed S Alsaedi, Abdulrahman Q Al Sulami, Emad H Al Asmari, Ahmad A Aalam, Imad M Khojah

TL;DR
This study explores emergency physicians' views on allowing family members to be present during resuscitation in Saudi Arabia, finding general support but highlighting the need for better policies and training.
Contribution
The study provides new insights into emergency physicians' perceptions and attitudes toward family presence during resuscitation in the western region of Saudi Arabia.
Findings
Most emergency physicians were unaware of family presence during resuscitation (FPDR) policies.
Younger, male, and more experienced physicians showed higher awareness of FPDR.
Nearly half of the participants supported implementing an FPDR policy.
Abstract
Background: Cardiac arrest remains a significant public health issue, with high incidence rates in both in-hospital and out-of-hospital settings. The practice of family presence during resuscitation (FPDR) has gained attention for its potential benefits to patients and their families. This study evaluates the perceptions, knowledge, and attitudes of emergency physicians (EPs) regarding FPDR in the emergency department (ED) and aims to inform policy development at King Abdulaziz University Hospital in Jeddah, Saudi Arabia. Methods: A multicenter cross-sectional study was conducted from January to April 2023, surveying EPs from multiple EDs across the western region of Saudi Arabia. Participants, certified in basic (BLS) or advanced life support (ALS), completed an anonymous online survey adapted from previous studies. Results: Our study surveyed 122 EPs, with 112 completing the survey.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
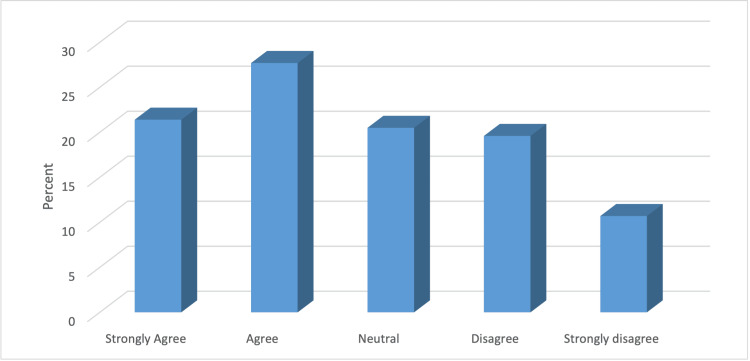 Figure 1
Figure 1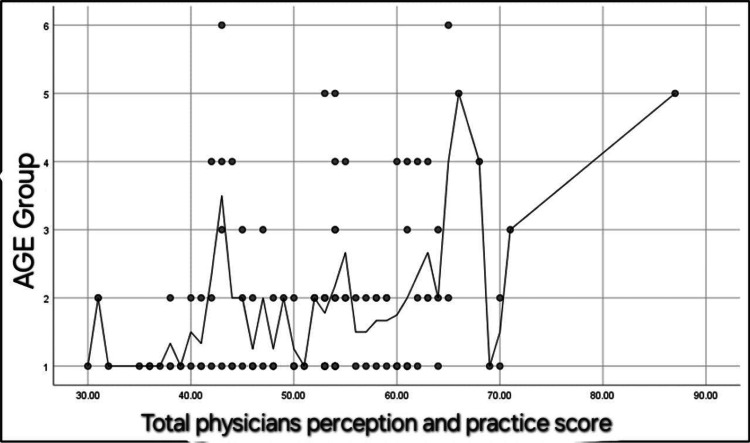 Figure 2
Figure 2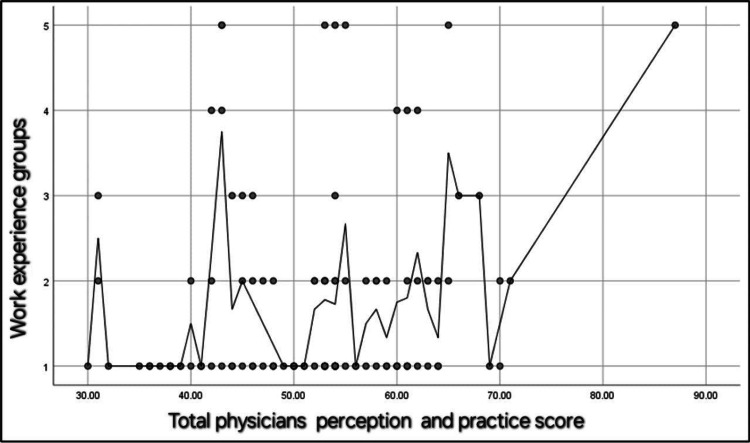 Figure 3
Figure 3| Variable | Are you aware of the family presence during resuscitation (FPDR) concept? | p-value | |
| No, n (%) | Yes, n (%) | ||
| Age (years) | 0.004 | ||
| 25-29 | 27 (75) | 28 (36.8) | |
| 30-34 | 6 (16.7) | 27 (35.5) | |
| 35-39 | 2 (5.6) | 6 (7.9) | |
| 40-44 | 0 (0.0) | 10 (13.2) | |
| 45-49 | 0 (0.0) | 4 (5.3) | |
| 50-55 | 1 (2.8) | 1 (1.3) | |
| Gender | 0.941 | ||
| Female | 14 (38.9) | 29 (38.2) | |
| Male | 22 (61.1) | 47 (61.8) | |
| Level of expertise | <0.001 | ||
| Residency PGY 1 | 0 (0.0) | 5 (6.6) | |
| Residency PGY 2 | 10 (27.8) | 5 (6.6) | |
| Residency PGY 3 | 5 (13.9) | 8 (10.5) | |
| Residency PGY 4 | 14 (38.9) | 9 (11.8) | |
| Senior registrar | 2 (5.6) | 14 (18.4) | |
| Specialist/registrar | 2 (5.6) | 19 (25) | |
| Consultant | 3 (8.3) | 16 (21.1) | |
| Work experience (years) | 0.01 | ||
| 1-4 | 30 (83.3) | 36 (47.4) | |
| 5-8 | 3 (8.3) | 24 (31.6) | |
| 8-11 | 1 (2.8) | 6 (7.9) | |
| 12-15 | 1 (2.8) | 4 (5.3) | |
| >15 | 1 (2.8) | 6 (7.9) | |
| Number of cardiopulmonary resuscitation (CPR) cases you lead per month | 0.008 | ||
| 1-5 | 18 (50) | 43 (56.6) | |
| 6-10 | 6 (16.7) | 19 (25) | |
| 11-15 | 1 (2.8) | 6 (7.9) | |
| 16-20 | 0 (0.0) | 2 (2.6) | |
| >20 | 0 (0.0) | 2 (2.6) | |
| None per month | 11 (30.6) | 4 (5.3) | |
| I don't know | No | Yes | |
| Are you aware of the family presence during resuscitation (FPDR) concept? | 0 | 36 (32.1) | 76 (67.9) |
| Have you participated in CPR during which a family member was present? | 0 | 39 (34.8) | 73 (65.2) |
| Do you have a written policy in your department/hospital allowing FPDR? | 76 (67.9) | 32 (28.6) | 4 (3.6) |
| Do you have a written policy in your department/hospital prohibiting FPDR? | 73 (65.2) | 32 (28.6) | 7 (6.3) |
| Are you aware of the family presence during resuscitation (FPDR) concept? | χ2 | df | Effect size | p-value | ||
| Variable | No | Yes | Value (significance) | |||
| n, (%) | n, (%) | |||||
| Age (years) | ||||||
| 25-29 | 27 (75) | 28 (36.8) | 17.3 | 5 | 0.007 (0.94) | 0.004 |
| 30-34 | 6 (16.7) | 27 (35.5) | ||||
| 35-39 | 2 (5.6) | 6 (7.9) | ||||
| 40-44 | 0 (0.0) | 10 (13.2) | ||||
| 45-49 | 0 (0.0) | 4 (5.3) | ||||
| 50-55 | 1 (2.8) | 1 (1.3) | ||||
| Gender | ||||||
| Female | 14 (38.9) | 29 (38.2) | 0.006 | 1 | 0.39 (0.004) | 0.941 |
| Male | 22 (61.1) | 47 (61.8) | ||||
| Level of expertise | ||||||
| Residency PGY 1 | 0 (0.0) | 5 (6.6) | 29.59 | 6 | 0.51 (<0.001) | <0.001 |
| Residency PGY 2 | 10 (27.8) | 5 (6.6) | ||||
| Residency PGY 3 | 5 (13.9) | 8 (10.5) | ||||
| Residency PGY 4 | 14 (38.9) | 9 (11.8) | ||||
| Senior registrar | 2 (5.6) | 14 (18.4) | ||||
| Specialist/registrar | 2 (5.6) | 19 (25) | ||||
| Consultant | 3 (8.3) | 16 (21.1) | ||||
| Work experience (years) | ||||||
| 1-4 | 30 (83.3) | 36 (47.4) | 13.22 | 4 | 0.34 (0.01) | 0.01 |
| 5-8 | 3 (8.3) | 24 (31.6) | ||||
| 8-11 | 1 (2.8) | 6 (7.9) | ||||
| 12-15 | 1 (2.8) | 4 (5.3) | ||||
| >15 | 1 (2.8) | 6 (7.9) | ||||
| Number of cardiopulmonary resuscitation (CPR) cases you lead per month | ||||||
| 1-5 | 18 (50) | 43 (56.6) | 15.54 | 5 | 0.37 (0.008) | 0.008 |
| 6-10 | 6 (16.7) | 19 (25) | ||||
| 11-15 | 1 (2.8) | 6 (7.9) | ||||
| 16-20 | 0 (0.0) | 2 (2.6) | ||||
| >20 | 0 (0.0) | 2 (2.6) | ||||
| None per month | 11 (30.6) | 4 (5.3) | ||||
| Variable | Total physicians' perception and practice score (mean ± SD) | p-value |
| Are you aware of the family presence during resuscitation (FPDR) concept? | 0.002 | |
| No | 47.3 ± 8.88 | |
| Yes | 53.86 ± 10.02 | |
| Have you participated in CPR during which a family member was present? | 0.006 | |
| No | 48.15 ± 8.62 | |
| Yes | 53.68 ± 10.37 | |
| Do you have a written policy in your department/hospital allowing FPDR? | 0.912 | |
| I don't know | 51.44 ± 9.65 | |
| No | 52.71 ± 11.3 | |
| Yes | 50 ± 10.8 | |
| Do you have a written policy in your department/hospital prohibiting FPDR? | 0.006 | |
| I don't know | 51.56 ± 10.5 | |
| No | 54.46 ± 8.13 | |
| Yes | 41.42 ± 7.8 | |
| Study | Number of participants | Findings |
| Demir [ | 144 | No benefits were noted for family presence during resuscitation. The majority (82.6%) did not support it, with the most common concerns being that family members would interfere with the team’s activities (56.3%) and that resuscitation could be too traumatic for families (43.6%). |
| Gold et al. [ | 521 | Half of the participants believed that family presence during resuscitation was beneficial for parents, with two-thirds indicating that parents would want the option. However, a key barrier identified was the potential for family presence to intimidate the resident physician. |
| Booth et al. [ | 162 | Participants highlighted several benefits of family presence during resuscitation, including helping family members accept that everything possible was done (48%), facilitating acceptance of death (48%), and aiding in the grieving process (38%). However, barriers such as concerns about family members becoming distressed and interfering with the resuscitation, fear of litigation, lack of space, and insufficient chaperones were also identified. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFamily and Patient Care in Intensive Care Units · Grief, Bereavement, and Mental Health · Family and Disability Support Research
Introduction
Cardiac arrest is a critical medical emergency with profound implications not only for patient survival but also for the psychological well-being of their relatives [1]. Family members who witness resuscitation efforts often experience intense emotional distress, which can manifest as anxiety, post-traumatic stress, or a sense of exclusion from the decision-making process. However, studies suggest that allowing family presence during cardiopulmonary resuscitation (CPR) may provide emotional closure, improve understanding of the patient’s condition, and foster trust in medical teams.
Cardiovascular diseases continue to be a major cause of mortality worldwide, prompting the adoption of machine learning approaches and other innovative techniques to improve both clinical and psychological outcomes [2]. Cardiac arrest, in particular, represents one of the most pressing public health concerns, with high incidence rates in both in- and out-of-hospital settings. While a significant proportion of cardiac arrests occur outside of medical facilities, the burden of in-hospital cardiac arrest (IHCA) is substantial. Recent studies report that approximately 300,000 IHCAs occur annually in the United States (US), underscoring the critical need for effective resuscitation strategies and family-inclusive policies in emergency settings [1,3]. Additionally, emerging evidence highlights the role of advanced hemodynamic monitoring techniques, such as perfusion index and end-tidal carbon dioxide levels, in improving resuscitation outcomes and guiding CPR interventions [3]. Despite ongoing debates, the practice of permitting family presence during resuscitation (FPDR) remains controversial among emergency medicine (EM) physicians. Factors such as provider discomfort, concerns over medicolegal risks, and potential disruptions to the resuscitation process contribute to varying attitudes toward this practice.
CPR is a crucial emergency procedure that significantly enhances the prognosis of many patients. Statistics from the National Registry of Cardiopulmonary Resuscitation reveal that only 9%-11% of CPRs performed in hospital settings take place within the emergency department (ED) [4]. In-hospital CPR is typically carried out by either a multidisciplinary advanced life support (ALS) team or a basic life support (BLS) team. These teams are responsible for maintaining clear airways, providing adequate rescue breaths, administering chest compressions, and delivering early defibrillation to patients in cardiac arrest [4,5].
The American Heart Association, along with other global organizations, highlights and advocates for the concept of FPDR, defined as "the presence of one or more family members or significant others in a location that enables visible or physical contact with the patient during invasive procedures or CPR" [6]. This practice has garnered significant attention due to its potential benefits for both the patient and their family, including emotional closure, improved trust in medical teams, and reduced psychological distress among relatives. Additionally, FPDR aligns with patient-centered care principles, emphasizing the importance of transparency and family involvement in critical medical interventions. Advocates of FPDR argue that allowing family members to be present during such critical moments can provide emotional support to both the patient and their loved ones by fostering a sense of familiarity and comfort in a highly stressful situation [6,7]. Family presence has been associated with reduced psychological distress, as it allows relatives to witness medical efforts firsthand, promoting transparency and trust in healthcare providers. Additionally, previous research suggests that FPDR may lower the incidence of post-traumatic stress disorder (PTSD), anxiety, and depression among family members of resuscitated patients. A review by Clark et al. found that relatives who were allowed to witness CPR had a significantly lower rate of PTSD symptoms three months post-resuscitation compared to those who were not present [7].
Additionally, it offers family members the opportunity to witness the medical efforts being made, which can aid in their understanding and acceptance of the patient's condition and the outcomes of the resuscitative efforts [8,9]. Research suggests that FPDR can also support the grieving process by providing a sense of closure and understanding, as family members can witness firsthand the heroic efforts made to save their loved one [9]. Despite these potential benefits, FPDR remains a topic of debate within the medical community, with concerns about its impact on healthcare providers' performance, the potential for increased stress or interference, and the appropriateness of such practices in all clinical situations [8,9]. In Saudi Arabia, cultural norms and limited FPDR policies may shape physician perspectives uniquely.
This study aims to evaluate the perceptions, knowledge, and attitudes of EPs regarding FPDR in the ED.
Materials and methods
Study design and population
This is a multicenter, cross-sectional study that examines EPs' perceptions and attitudes toward FPDR in ED CPR cases in the western region of Saudi Arabia, conducted from January to April 2023. The study population included EPs working full-time at local EDs across the western region, spanning all residency and career levels, from residents to consultants/attendings. The study included licensed healthcare professionals, specifically emergency medicine physicians and nurses, who held a valid BLS or ALS certification at the time of enrollment and provided informed consent. Exclusion criteria encompassed individuals without a valid BLS or ALS certification, those with expired or unverified certifications, participants with incomplete data, and individuals who declined to participate.
Data collection
An anonymous, self-administered online survey was distributed via Google Forms over a one-month period to emergency medicine (EM) physicians and nurses working in hospitals in the western region of Saudi Arabia. Eligible participants were identified based on their active practice in emergency medicine, verified through hospital staff records and professional medical associations. The invitations were sent through official hospital email lists, professional networks, and direct outreach via medical organizations. The survey questions were adapted from previous studies [7]. Given the high reliability and validity ratings of the questionnaires by Tomlinson et al. [6] and Kianmehr et al. [10], items from these studies were incorporated into this survey. A Cronbach’s alpha reliability coefficient was calculated using IBM SPSS Statistics for Windows, Version 26.0 (Released 2019; IBM Corp., Armonk, NY, US) based on the 18 standardized items in the questionnaire, yielding a value of 0.789, which indicates acceptable reliability.
The questionnaire was divided into three sections. The first section collected demographic data, including age, gender, level of expertise, work experience, hospital type, and the number of CPR cases led per month. The second section consisted of four questions regarding the participants’ knowledge and experience of FPDR. The third section included 18 items assessing participants' perceptions and practices regarding FPDR. These items were measured using a five-point Likert scale, with scores ranging from 1 (strongly disagree) to 5 (strongly agree). Reverse-coded questions were scored from 1 to 5. The total score for EPs' perception and practice of FPDR ranged from 18 to 90, with 18 indicating the lowest knowledge score and 90 the highest knowledge score. The questionnaire is provided as a supplementary file (Appendix 1) to enhance transparency and facilitate future research replication.
Ethical approval
Ethical approval for the study was obtained from the Research Ethics Committee of King Abdulaziz University Hospital, Jeddah, Saudi Arabia (NCBE registration number: HA-02-J-008). To ensure adequate statistical power, the sample size was initially calculated to be 168 ED physicians, based on a medium effect size (Cohen's d = 0.5) observed in previous studies examining healthcare providers' perceptions of FPDR. Additionally, for a finite population of 250, with a 95% confidence interval (p = 0.5) and a margin of error of 5%, the final required sample size was estimated to be 152 participants [11]. However, we successfully collected data from 112 participants. A post hoc power analysis confirmed that our sample size provides sufficient statistical power to detect meaningful effects, indicating that further data collection was unnecessary.
Data analysis
Data analysis was conducted using IBM SPSS Statistics for Windows, Version 26.0 (Released 2019; IBM Corp., Armonk, NY, US). To examine correlations between variables, qualitative data were quantified as numerical values and percentages and analyzed using the chi-squared test (χ^2^). Quantitative data were expressed as means and standard deviations (mean ± SD). Non-parametric variables were assessed using the Mann-Whitney and Kruskal-Wallis tests. Spearman's rank correlation test was used for analyzing relationships between variables, with statistical significance set at p < 0.05.
Results
Demographic Data
Our study surveyed 122 EPs, of whom 112 completed the survey. Ten were excluded as they did not meet the inclusion criteria. Table 1 presents the participants' demographic characteristics, showing that 55 (49.1%) of the surveyed EM physicians were aged 25-29 years; of these, 69 (61.6%) were men, 23 (20.5%) were in residency PGY 4, and 66 (58.9%) had 1-4 years of work experience. Forty-three (38.4%) worked at academic hospitals, and 61 (54.5%) led 1-5 CPR cases per month.
Outcomes
Most EM physicians (n = 76, 67.9%) were aware of the FPDR concept. Additionally, 73 (65.2%) had participated in CPR with a family member present. Of the 24 hospitals, only four (3.6%) had a written policy in their department/hospital allowing FPDR, while seven (6.3%) had a policy prohibiting it. Regarding policy support, 55 (49.1%) agreed or strongly agreed with implementing a policy allowing FPDR in their institution. Awareness of the FPDR concept was significantly higher among men, specialists/registrars, those with 1-4 years of work experience, and those leading 1-5 CPR cases per month (p < 0.05) (Table 2 and Figure 1).
Percentage distribution of EM physicians according to their support in implementing a policy that allows FPDR in their institution.
The mean score of physicians' perception and practice was significantly higher among male physicians (p < 0.05) (Table 3). No significant relationship was found between the mean total score and other demographics or work data (p > 0.05). However, Table 4 shows that the mean score of physicians’ perception and practice was significantly higher among physicians aware of the FPDR concept (p < 0.05). Similarly, the mean total score was significantly higher among those who had participated in CPR with a family member present (p < 0.05). A significantly higher mean total score was also observed among those without a written policy prohibiting FPDR in their department/hospital (p < 0.05).
Additionally, there was a significant positive correlation between the total physicians' perception and practice score and their age (r = 0.29, p = 0.002) (Figure 2). A significant positive correlation was also found between the total physicians' perception and practice score and their work experience in years (r = 0.18, p = 0.04) (Figure 3).
Spearman's correlation between the total physicians' perception and practice score and their age.N.B.: r =0.29, p = 0.002).Age groups: (1) 25-29 years old, (2) 30-34 years old, (3) 35-39 years old, (4) 40-44 years old, (5) 45-49 years old, (6) 50-55 years old.
Spearman's correlation between the total physicians' perception and practice score and their work experiences in years.N.B.: r =0.18, p = 0.04.Work experience groups: (1) 1-4 years of experience, (2) 5-8 years of experience, (3) 8-11 years of experience, (4) 12-15 years of experience, (5) more than 15 years of experience.
Discussion
Qualitative and survey-based studies have shown that FPDR positively impacts families' psychological well-being [12-14], prompting numerous professional organizations to recommend policies supporting FPDR [15-17]. Despite these endorsements, many healthcare professionals continue to oppose FPDR, citing potential disruptions to resuscitation efforts and risks to patient safety [18].
Our cross-sectional study revealed that EM physicians' perceptions, knowledge, and attitudes toward FPDR in the ED were predominantly positive and statistically significant. This finding contrasts with the study by Al Bshabshe et al. [19], where physicians largely opposed FPDR. This discrepancy may be attributed to various cultural, institutional, and educational differences between the study populations. Furthermore, our data indicated a positive correlation between age and experience on physicians' perceptions of FPDR, as illustrated in Figure 2 and Figure 3. This suggests that more experienced and older physicians might have developed a greater appreciation for the benefits of FPDR over time. A literature review of related studies was conducted and is summarized in Table 5. Demir [20] found that 82.6% of the participants did not support FPDR. However, in our study, 67.9% of the participants were aware of and supported FPDR.
A significant majority of EM physicians (67.9%) demonstrated awareness of FPDR. The findings revealed that up to 72% of respondents supported implementing a family facilitator role to enhance the practice of FPDR. Soleimanpour et al. reported that 35.7% of respondents favored allowing family presence during CPR, while 42.2% were against it [23]. Despite this awareness, there exists an antagonistic policy toward FPDR in many hospitals. Specifically, only 6.3% of the respondents reported a written policy in their department or hospital explicitly prohibiting FPDR. Conversely, there appears to be a significant lack of knowledge regarding written policies supporting FPDR, with only 3.6% of respondents indicating such a policy existed. This lack of formal policies may contribute to uncertainty and inconsistency in the application of FPDR practices across institutions.
Age has often been considered a factor influencing attitudes toward family presence during CPR. While a previous cross-sectional study found no correlation between age and acceptance of this practice [23], our study revealed a significant relationship, suggesting a potential change in attitudes or differing population dynamics.
Approximately 65.2% have been in a resuscitation attempt with a family member present. However, other studies conducted on nurses revealed that more than half of the nurses have never been in a resuscitation attempt with a family member present [24,25].
Notably, 49.1% of participants agreed or strongly agreed on the importance of implementing a policy allowing FPDR in their institution. Implementing such policies could standardize the practice, provide clear guidelines, and potentially improve patient and family outcomes during resuscitation efforts [26-28].
Additionally, our study underscored the importance of having dedicated and trained personnel to accompany family members during CPR. This recommendation aligns with the European Resuscitation Council Guidelines of 2021 [29], which advocate for the presence of a designated healthcare professional to provide explanation and comfort to family members present during resuscitation. This approach ensures that family members receive the necessary support and information during critical moments, which can help mitigate the emotional impact of witnessing a resuscitation.
Furthermore, the presence of trained personnel can facilitate better communication and reduce the potential for misunderstandings or conflicts during resuscitation efforts. It also allows the medical team to focus on the resuscitation process, knowing that the family members are being supported and informed by a dedicated professional. This holistic approach to resuscitation not only benefits the family members but also enhances the overall quality of care provided in the ED. The inconclusive findings of the meta-analysis of da Silva Barreto [30] highlight the complexity of FPDR, necessitating careful consideration when integrating it into routine practice.
Strengths and limitations
Although the study contributes to a better understanding of the barriers to widespread acceptance of FPDR, larger multicenter studies need to be conducted to clearly demonstrate the extent and significance of regional and cultural variations in physicians' perceptions, knowledge, and attitudes toward this critical practice issue in emergency medicine departments. There is also a need to study the perspectives of other healthcare providers toward FPDR. Additionally, self-reported measures (questionnaires) in public surveys that collect data are more susceptible to response and recall biases.
Conclusions
The majority of EPs in the western region of Saudi Arabia are acquainted with the concept of FPDR and generally hold a favorable attitude toward this practice. However, some physicians have expressed reservations about FPDR, citing concerns regarding potential negative impacts on performance or medicolegal issues. These areas warrant further investigation for a more comprehensive understanding. Finally, effective implementation of FPDR policies necessitates consideration of numerous variables to enhance outcomes for patients, their families, and healthcare providers alike.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Psychological and behavioral dimensions in cardiac arrest survivors and their families: a state-of-the-art review Neurotherapeutics Agarwal S Wagner MK Mion M 022202510.1016/j.neurot.2024.e 00509 PMC 1184035239709245 · doi ↗ · pubmed ↗
- 2Emergence of artificial intelligence and machine learning models in sudden cardiac arrest: a comprehensive review of predictive performance and clinical decision support Cardiol Rev Jain H Marsool MD Odat RM 202410.1097/CRD.000000000000070838836621 · doi ↗ · pubmed ↗
- 3Comparative analysis of perfusion index and end-tidal carbon dioxide in cardiac arrest patients: implications for hemodynamic monitoring and resuscitation outcomes Cureus Dogan B Kudu E DanışF Ince EO Karaca MA Erbil B 015202310.7759/cureus.50818 PMC 1079722138249229 · doi ↗ · pubmed ↗
- 4Cardiopulmonary resuscitation for in-hospital events in the emergency department: a comparison of adult and pediatric outcomes and care processes Resuscitation Donoghue AJ Abella BS Merchant R Praestgaard A Topjian A Berg R Nadkarni V 941009220152593932310.1016/j.resuscitation.2015.04.027PMC 4788967 · doi ↗ · pubmed ↗
- 5Cardiac arrest in the emergency department: a report from the National Registry of Cardiopulmonary Resuscitation Resuscitation Kayser RG Ornato JP Peberdy MA 1511607820081850818410.1016/j.resuscitation.2008.03.007 · doi ↗ · pubmed ↗
- 6Family presence during adult resuscitation. A survey of emergency department registered nurses and staff attitudes Adv Emerg Nurs J Tomlinson KR Golden IJ Mallory JL Comer L 4658322010 https://journals.lww.com/aenjournal/abstract/2010/01000/family_presence_during_adult_resuscitation__a.8.aspx
- 7Family presence during cardiopulmonary resuscitation Crit Care Nurs Clin North Am Clark AP Aldridge MD Guzzetta CE 23321720051574939810.1016/j.ccell.2004.09.004 · doi ↗ · pubmed ↗
- 8Family presence during invasive procedures and resuscitations in the emergency department: a critical review and suggestions for future research Ann Emerg Med Boudreaux ED Francis JL Loyacano T 1932054020021214049910.1067/mem.2002.124899 · doi ↗ · pubmed ↗