Urinary Tract Infection Caused by Lactococcus garvieae in a 75-Year-Old Male Patient With a Complex Medical History
Baker Edrees, Muhammad Ali Khalid, Munir Shah, Rida Ghani

TL;DR
A 75-year-old man with a complex medical history was successfully treated for a rare urinary tract infection caused by Lactococcus garvieae.
Contribution
This case report highlights the clinical management and awareness of Lactococcus garvieae as a rare human pathogen.
Findings
Lactococcus garvieae caused a urinary tract infection in a 75-year-old male with pyohydronephrosis.
Successful treatment involved intravenous ampicillin/sulbactam followed by oral linezolid.
The report emphasizes the need for increased awareness of L. garvieae as a potential human pathogen.
Abstract
Lactococcus garvieae, a Gram-positive bacterium traditionally associated with infections in fish, has been increasingly recognized as a rare pathogen in human infections, including urinary tract infections (UTIs). We present a case of a 75-year-old male patient with pyohydronephrosis and a complex medical history who was diagnosed with a UTI caused by L. garvieae. The patient was successfully treated with a combination of intravenous ampicillin/sulbactam followed by oral linezolid, resulting in the resolution of symptoms. This report also compares this case with other documented cases of L. garvieae infections, highlighting its pathogenic mechanisms, clinical manifestations, treatment strategies, and the need for heightened awareness of this pathogen.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
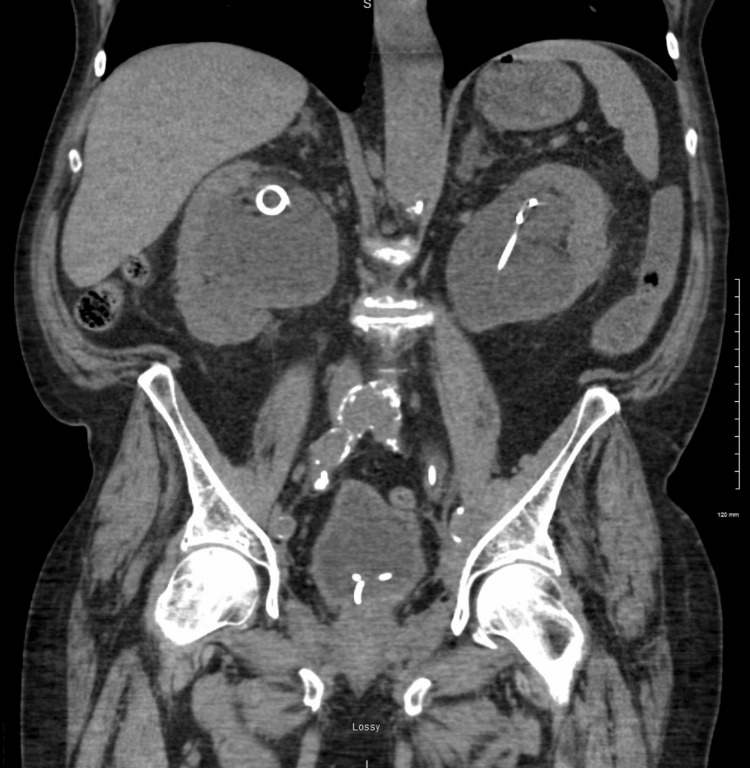 Figure 1
Figure 1| Urine content | Results | Normal (range if applicable) |
| Urine color | Straw color | Yellow |
| Urine clarity | Turbid | Clear |
| Urine pH | 6 | 5.0-8.0 |
| Urine specific gravity | 1.025 | 1.005-1.030 |
| Urine protein (mg/dL/24 hrs) | 100 (H) | None seen |
| Urine glucose (mg/dL) | None seen | None seen |
| Urine ketones (mg/dL) | None seen | None seen |
| Urine blood (mg/dL) | Large (A) | None seen |
| Urine nitrate (mg/dL) | None seen | None seen |
| Urine urobilinogen (E.U./dL) | 0.2 (A) | None seen |
| Urine bilirubin (mg/dL) | None seen | None seen |
| Urine leukocyte esterase (mg/dL) | Large (A) | None seen |
| Urine RBCs per HPF | 6-10 (A) | 0-2 |
| Urine WBCs per HPF | Tntc (A) | 0-5 |
| Urine squamous epithelial cells per HPF | None seen | 0-5 |
| Urine transition epithelial cells per HPF | 0-5 | None seen |
| Calcium oxalate crystals per HPF | Few (A) | None seen |
| Amorphous crystals per HPF | Few (A) | None seen |
| Urine bacteria per HPF | Many (A) | None seen |
| Hyaline casts per LPF | None seen | None seen |
| Urine mucus per LPF | Present (A) | None seen |
| Sample location | Final culture result |
| Urine, clean catch |
|
| Urine, Kidney tap right | Alpha hemolytic strep, not Gram positive type D |
| Urine, Kidney tap left | Alpha hemolytic strep, not Gram positive type D |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Bacterial Identification and Susceptibility Testing · Antimicrobial Resistance in Staphylococcus
Introduction
Lactococcus garvieae is a Gram-positive coccus primarily known as a pathogen in fish, particularly in farmed aquatic organisms (aquaculture). However, in recent years, *L. garvieae *has been increasingly implicated in human infections, including endocarditis, biliary tract infections, and urinary tract infections (UTIs), and often in individuals with underlying health conditions or immunocompromised states [1-9]. UTIs caused by L. garvieae are particularly rare, with only a few cases documented in the literature. This report presents a case of a UTI caused by L. garvieae in an elderly male patient with a complex medical history, underscoring the importance of recognizing this pathogen in atypical presentations.
Diagnosis of an infection with L. garvieae involves microbiological culture and identification. Blood cultures are essential for detecting bacteremia or endocarditis. The bacterium can be identified using biochemical tests, such as catalase and oxidase tests, and confirmed by molecular methods like 16S rRNA gene sequencing or Matrix-Assisted Laser Desorption Ionization - Time of Flight (MALDI-TOF) mass spectrometry [4]. Depending on the susceptibility profiles, treatment typically involves antibiotics such as the penicillin family, vancomycin or gentamicin [4-9]. For instance, L. garvieae isolates from bovine mastitis were found to be susceptible to penicillin, ampicillin, amoxicillin-clavulanic acid, imipenem, ceftiofur, enrofloxacin, and marbofloxacin [7]. All isolates had virulence genes coding for collagenase, fibronectin-binding protein, glyceraldehyde-3-phosphate dehydrogenase, superoxide dismutase, and nicotinamide adenine dinucleotide + hydrogen (NADH) oxidase. Most isolates had lsaD and mdtA antimicrobial resistance genes [4-7].
L. garvieae is thus a versatile pathogen with a broad host range. It causes various diseases in aquatic, bovine, and human hosts. Its diagnosis and treatment require specific microbiological and antibiotic susceptibility testing. This case highlights the differential diagnosis of L. garvieae in patients with suspected complex UTI and underscores the need to consider screening for this pathogen when primary differentials are ruled out. Given its genomic features, including virulence and resistance genes, L. garvieae may contribute significantly to pathogenicity.
Case presentation
A 75-year-old male patient with a past medical history of chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), sick sinus syndrome, urethral strictures secondary to prostate cancer radiation therapy (requiring periodic J-stent replacement), and a history of rectal adenocarcinoma (current status post-resection) presented to the emergency department. He complained of 10/10 constant, sharp pain localized to the hypogastric region, which was associated with vomiting and fever. The patient denied any urinary symptoms. However, his symptoms had persisted for several days, prompting medical evaluation. A CT scan of the abdomen and the pelvis revealed bilateral hydroureteronephrosis [Figure 1]. A Foley catheter was placed, and the patient received a single dose of ceftriaxone in the emergency department.
CT scan showing severe bilateral hydroureteronephrosis and the presence of ureter stents
The patient was admitted. He was afebrile and hemodynamically stable. Urinalysis showed the presence of red blood cells (RBCs) and white blood cells (WBCs), and was positive for esterase [Table 1].
The urine culture grew bacteria consistent with L. garvieae [Table 2].
The patient was diagnosed with pyohydronephrosis, a suppurative kidney infection secondary to obstruction, and was started on a four-week course of intravenous ampicillin-sulbactam (Unasyn), followed by four weeks of oral linezolid (Zyvox) to specifically target *L. garvieae. *Throughout the admission, the patient remained afebrile and hemodynamically stable. A urinary voiding trial was successful, allowing for the removal of the Foley catheter to prevent further complications. The patient responded well to treatment, demonstrating significant clinical improvement. There was symptom resolution by day four and progressive resolution of hydroureteronephrosis.
Discussion
This case highlights several key aspects of *L. garvieae *as an emerging pathogen in human infections. Its pathogenesis in UTIs involves its ability to adhere to uroepithelial cells, form a capsule, and produce extracellular enzymes such as proteases and hemolysins [10]. These virulent factors contribute to the bacterium’s ability to cause tissue damage and evade the host immune response [10]. In this patient, urethral strictures and periodic stent replacements likely created an environment conducive to bacterial colonization and infection. The ability of L. garvieae to form a capsule may have played a significant role in the persistence of the infection, particularly in the presence of indwelling devices such as J stents. While such UTIs are rare, a literature review reveals a few documented cases that provide valuable insights into this pathogen's clinical presentation and management.
A case by Amarasinghe et al. [4] reported *L. garvieae *bacteremia associated with adenocarcinoma, illustrating its opportunistic nature in immunocompromised patients. Bacteremia developed following a suspected breach of mucosal barriers [4], emphasizing the need for vigilance in managing these infections in patients with cancer. This is particularly relevant to our case, given the patient’s history of rectal adenocarcinoma and ureteral stent placement, which may have contributed to the mucosal barrier disruption.
Colussi et al. documented the first human UTI caused by Lactococcus petauri, another species within the Lactococcus genus [5]. This report expands the clinical spectrum of Lactococcus species as human pathogens. It suggests vigilance in identifying these unusual pathogens, especially in patients with recurrent or refractory UTIs [5]. In contrast, Malek et al. described a case of infective endocarditis caused by L. garvieae, highlighting the bacterium’s potential to cause severe systemic infections beyond the urinary tract [7]. The case involved a patient with a history of mitral prosthetic valve, suggesting that L. garvieae may preferentially infect individuals with preexisting cardiac conditions. This case emphasizes the importance of considering it as a potential cause of infection in patients with complex medical histories, like our patient who had multiple comorbidities [7].
Tariq et al. reported a similar case involving a 74-year-old female patient with recurrent UTIs who presented with fever and dysuria [8]. Urine cultures confirmed L. garvieae, and the patient was successfully treated with ampicillin. In our case, the patient had underlying urinary tract abnormalities, which likely contributed to the infection [8]. Additionally, Woolery reported an acute lower UTI caused by L. garvieae in a patient without significant predisposing factors [9]. This case is notable as it suggests that L. garvieae can cause UTIs even in individuals without the complex medical histories observed in other cases. In this case, the successful treatment with ceftriaxone further underscores the need for antibiotic susceptibility testing in guiding treatment [9].
These comparative cases emphasize the importance of recognizing *L. garvieae *as an emerging human pathogen, particularly in patients with complex medical histories, immunosuppression, or urinary tract abnormalities. The diversity in clinical manifestations and outcomes observed in these cases highlight the need for early recognition, appropriate culture, sensitivity testing, and targeted antibiotic therapy in managing infections by the Lactococcus genus.
Conclusions
This case of a UTI caused by L. garvieae in a 75-year-old male patient with a complex medical history adds to the growing evidence of it being an emerging human pathogen. Given its rarity in human infections, clinicians should maintain a high index of suspicion in UTIs with atypical presentations or multiple predisposing factors. The successful outcome in this case underscores the importance of timely diagnosis and targeted antibiotic therapy. L. garvieae should be included in the differential diagnosis of UTIs, particularly in patients with complex medical histories and indwelling devices. Its ability to form biofilms may contribute to the persistent infections, necessitating prolonged or targeted antibiotic regimens. Early culture and sensitivity testing are crucial for guiding effective treatment. Future research should further elucidate the pathogenic role of Lactococcus species and establish management guidelines for these rare infections.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Urinary tract sepsis caused by Lactococcus garvieae Clinical Microbiology Newsletter Dylewski J 3031362014 https://doi.org/10.1016/j.clinmicnews.2014.01.007
- 2Infective endocarditis with Lactococcus garvieae in Japan: a case report J Med Case Rep Watanabe Y Naito T Kikuchi K 35652011 https://doi.org/10.1186/1752-1947-5-3562182768510.1186/1752-1947-5-356PMC 3170869 · doi ↗ · pubmed ↗
- 3First report of human acute acalculous cholecystitis caused by the fish pathogen Lactococcus garvieae J Clin Microbiol Kim JH Go J Cho CR Kim JI Lee MS Park SC 712714512013 https://doi.org/10.1128/jcm.02369-122324137610.1128/JCM.02369-12PMC 3553880 · doi ↗ · pubmed ↗
- 4A curious case of Lactococcus garvieae bacteremia associated with adenocarcinoma ID Cases Amarasinghe SN Fontenot AL Husan A Khan MW 029202210.1016/j.idcr.2022.e 01557 PMC 927024835818444 · doi ↗ · pubmed ↗
- 5First report of human urinary tract infection caused by Lactococcus petauri Microorganisms Colussi S Pastorino P Prearo M 25831120233789424110.3390/microorganisms 11102583 PMC 10609302 · doi ↗ · pubmed ↗
- 6The zoonotic potential of Lactococcus garvieae: an overview on microbiology, epidemiology, virulence factors and relationship with its presence in foods Res Vet Sci Gibello A Galán-Sánchez F Blanco MM Rodríguez-Iglesias M Domínguez L Fernández-Garayzábal JF 597010920162789287510.1016/j.rvsc.2016.09.010 · doi ↗ · pubmed ↗
- 7Lactococcus garvieae, an unusual pathogen in infective endocarditis: case report and review of the literature BMC Infect Dis Malek A De la Hoz A Gomez-Villegas SI Nowbakht C Arias CA 3011920193094390610.1186/s 12879-019-3912-8PMC 6446321 · doi ↗ · pubmed ↗
- 8Urinary tract infection caused by the novel pathogen, Lactococcus garvieae: a case report Cureus Tariq EF Irshad Y Khalil HB Khakwani AS Khan UA 0122020 https://doi.org/10.7759/cureus.946210.7759/cureus.9462 PMC 745539232874793 · doi ↗ · pubmed ↗