Neonatal total gastrectomy as treatment for gastric rupture: Case report
Arturo Javier Cavazos Castro, Castro Anaya Harold, José Asz Sigall, María Elena Ortega Ramírez, Claudia Elitania Espinosa Guerrero, Horacio G. Carvajal

TL;DR
A 2-day-old baby survived a rare and severe stomach rupture treated with total stomach removal and a special intestinal connection, showing the importance of careful post-surgery care.
Contribution
This case report presents a rare neonatal total gastrectomy using a pouchless Roux-en-Y esophagojejunostomy for extensive gastric perforation.
Findings
The patient survived and achieved adequate nutritional status 2.9 years post-surgery.
Pouchless Roux-en-Y reconstruction was successfully used in this neonatal gastrectomy case.
Barotrauma, prematurity, low weight, and gastric ischemia were identified as risk factors for gastric perforation.
Abstract
Neonatal gastric perforation is an uncommon but life-threatening condition, rarely requiring gastrectomy. We report the case of a neonate requiring total gastrectomy secondary to suspected barotrauma leading to gastric perforation. A 2-day-old term male was referred to our institution in extremis following attempted resuscitation with makeshift positive airway pressure ventilation in the setting of respiratory distress. Exam was notable for a distended, peritonitic abdomen, and abdominal radiograph showed massive pneumoperitoneum. Exploratory laparotomy revealed an extensive anterior gastric perforation extending from the pylorus to the esophagogastric junction, along with gross ischemia of the posterior gastric wall. The patient underwent gastrectomy with pouchless retrocolic Roux-en-Y esophagojejunostomy reconstruction. He was kept NPO (nil per os) on total parenteral nutrition for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
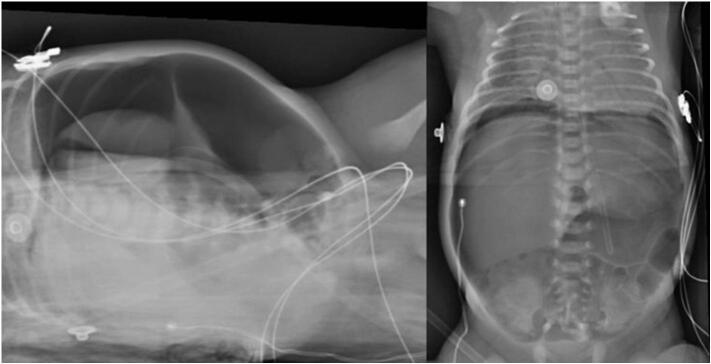 Figure 1
Figure 1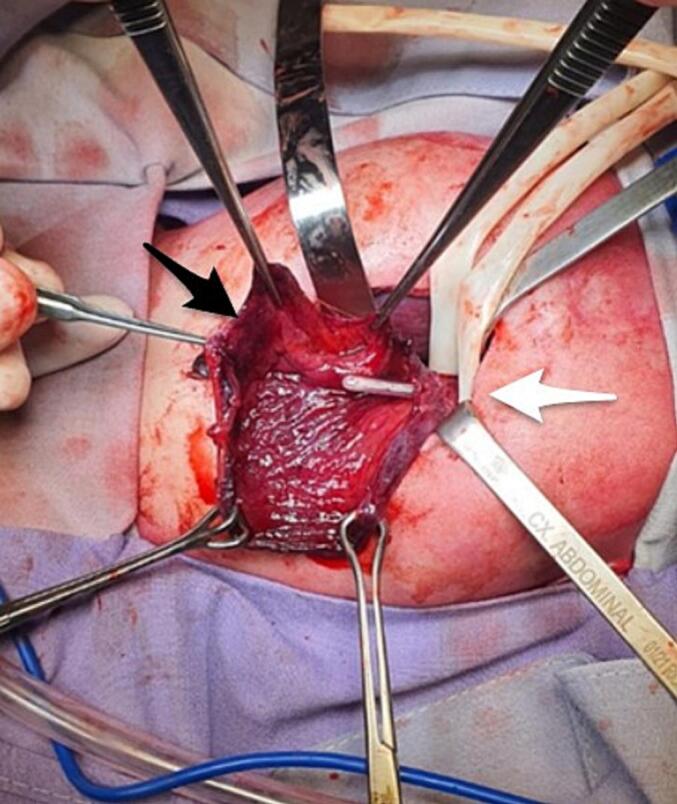 Figure 2
Figure 2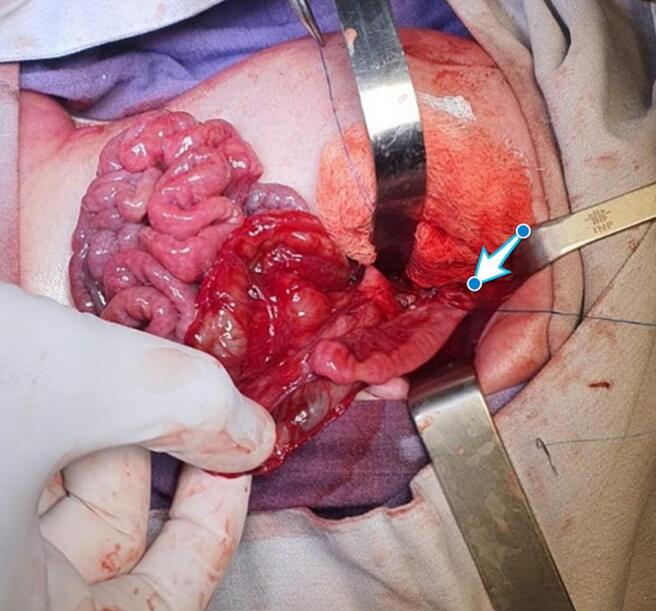 Figure 3
Figure 3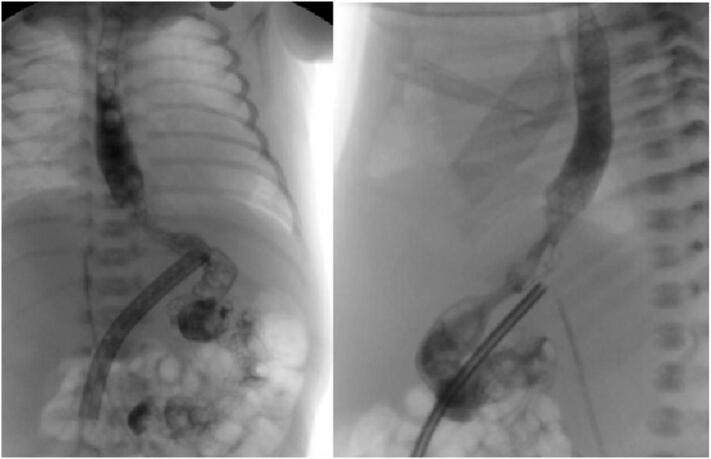 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Anomalies and Fetal Surgery · Esophageal and GI Pathology · Clinical Nutrition and Gastroenterology
Introduction
1
Neonatal gastric perforation is a rare but life-threatening entity, with a reported incidence of 1 in 5000 births and a mortality as high as 75 % [1,2]. Gastrectomy in the neonatal period is similarly extremely rare, with just a few isolated case reports. The majority of these reports performed a Hunt-Lawrence pouch esophagojejunostomy with the aim of providing a reservoir which theoretically diminishes the risk of dumping syndrome and improves postoperative weight gain [2,3].
We present the case of a 2-day-old boy transferred to our institution with an extensive gastric perforation, presumably related to barotrauma, which required gastrectomy with a pouchless Roux-en-Y esophagojejunostomy reconstruction, achieving adequate postoperative nutrition.
This manuscript was prepared following the SCARE guidelines [4].
Case report
2
A 37-week term boy with adequate birth weight was born by cesarean section at a small outside hospital. At birth, with a weight of 3300 g, height of 50 cm. Despite initial APGAR score of 8/9 and Silverman-Andersen score of 2, he developed respiratory distress requiring supplemental oxygen. He continued to present worsening respiratory distress, prompting escalation with an artisanal hospital-made bubble continuous positive airway (CPAP) support system with a reported rate of 6 l/min and a positive pressure of 4 cmH_2_O. After two days of persistent respiratory distress despite positive pressure ventilation, he was transferred to our institution.
On arrival to the neonatal intensive care unit (NICU), the patient was hemodynamically unstable on pressor support. Physical exam was notable for respiratory distress and a distended, peritonitic abdomen. Laboratory tests showed hemoglobin 12 mg/dl, hematocrit 36 %, WBC 11.4 × 10^9^/l, and platelets 295 × 10^9^/l. Abdominal radiographs showed massive pneumoperitoneum (Fig. 1), meriting an urgent laparotomy. Intraoperative findings were notable for an anterior gastric perforation extending from the gastroesophageal junction to the pylorus, along with extensive ischemia of the posterior gastric wall (Fig. 2). He remained on epinephrine, milrinone, and vasopressin intraoperatively, with transfusion of 1 unit of packed red blood cells at 20 ml/kg. Given his surgical findings and hemodynamic instability, we decided to proceed with a total gastrectomy and retrocolic Roux-en-Y pouchless end-to-end esophagojejunostomy (Fig. 3). We created the esophagojejunal anastomosis using a single layer of 5–0 polypropylene interrupted stitches, and the jejunojejunal anastomosis with a single layer of 6–0 polyglycolic acid interrupted stitches. Analysis of the explanted stomach by pathology reported a complete loss of architecture of the anterior gastric wall due to a large perforation. On the posterior surface, a 1.5 × 1.5 cm perforation was identified, with irregular and friable edges as well as surrounding tissue ischemia.Fig. 1. Anteroposterior and Right lateral decubitus abdominal radiograph showing pneumoperitoneum.Fig. 1. Fig. 2Extensive anterior gastric perforation with necrotic borders and posterior gastric wall precluding primary repair. Black arrow shows the esophagogastric junction with NG tube. White arrow shows the pylorus.Fig. 2. Fig. 3Retrocolic pouchless Roux-en-Y esophagojejunostomy pointed by white arrow.Fig. 3
Following surgery, the patient was managed by a multidisciplinary team comprised of neonatologists, gastroenterologists, nutritionists, and pediatric surgeons. He returned to the NICU on milrinone, epinephrine, and norepinephrine support, which were slowly weaned over the following 3 days. He was kept NPO and supported on total parenteral nutrition with SMOFLipid for the first week after surgery. On postoperative day (POD) 7, he underwent an esophagram which showed adequate patency of the esophagojejunostomy with no contrast leak (Fig. 4). He subsequently started on a hypercaloric elemental formula via nasojejunal tube, which was gradually increased to a goal of 180 ml/kg/day and supplemented with vitamin B12, vitamin D, pancreatic enzymes, ferrous sulfate, and calcium.Fig. 4. Anteroposterior and left lateral esophagogram, visualizing adequate passage of contrast medium through the pouchless esophagojejunal anastomosis.Fig. 4
Following an uneventful postoperative course, the patient was discharged home on POD 45. Over the past 2 years and 9 months, he has been regularly followed in clinic by pediatric surgery, neonatology, and general pediatrics. His current nutritional regimen is comprised of a normal diet supplemented with elemental formula (32 oz per day), vitamin D (800 IU), zinc (30 mg), ferrous sulfate (60 mg), and pancreatic enzymes (100 mg per meal). Additionally, he receives vitamin B12 (1000 μg) injections monthly. At his most recent follow-up visit, the patient weighed 11.6 kg (10th percentile), with a height of 89 cm (9th percentile) and a weight-for-height ratio of 11.8 %. His latest laboratory exams reported a hemoglobin of 13 g/dl, hematocrit 39 %, serum protein 6.8 g/dl, albumin 4.6 g/dl, prealbumin 21 mg/dl, transferrin 331 mg/dl, vitamin D levels 41 ng/ml, vitamin B12 levels 84 pg/dl, and iron 84 μg/dl.
Discussion
3
The current case report highlights the importance of prompt surgical treatment and multidisciplinary postoperative care in the case of suspected neonatal gastric perforation. The suspected etiology of this patient's gastric perforation was barotrauma secondary to the use of an artisanal bubble CPAP for respiratory support. Although the extent of his injury and resulting tissue necrosis precluded primary repair of the gastric perforation, he experienced a relatively benign postoperative course following total gastrectomy with pouchless Roux-en-Y esophagojejunostomy. Multidisciplinary care by a team comprised of neonatologists, gastroenterologists, nutritionists, and pediatric surgeons was essential for adequately resuscitating this patient and optimizing his nutritional support.
Spontaneous neonatal gastric perforation is a rare, life-threatening condition with a reported incidence of 1:5000 live births and a mortality rate ranging from 9 to 68 % [1,[5], [6], [7]]. Gastric perforations are observed in male neonates four times more often compared to females [5,8], and both prematurity and low birth weight have been associated with greater risk of perforation and associated mortality [1,2,[5], [6], [7],9]. It usually occurs between the second and seventh days of age [1,2,6]. The majority of cases are idiopathic, accounting for 47 % of cases in a systematic review of 51 articles on neonatal gastric perforation [1]. The most cause for non-idiopathic gastric perforation is iatrogenic, including secondary to barotrauma as suspected in our patient, followed by underlying gastrointestinal pathologies, such as necrotizing enterocolitis, small bowel obstruction, esophageal atresia or tracheoesophageal fistula [1].
The pathophysiology behind the increased risk of gastric perforation in prematurity and low birth weight is thought to be due to defects of the gastric muscle walls, including immature tissues, and a lack of intestinal pacemaker cells and C-kit mast cells [1,10]. Significant gastric distension, as seen with positive pressure ventilation, can cause mucosal ischemia, necrosis, and resulting perforation. Gastric ischemia can also be caused by hypotension, hypoxia, vasculopathy, thrombosis, and congenital heart disease. Similarly, medications such as corticosteroids, indomethacin, or ibuprofen can injure gastric mucosa, potentially resulting in perforation. Immature gastric peristalsis, frequently present at birth, favors an increase in gastric pressures, while gastric atony and pyloric spasm may lead to punctiform perforations of the gastric wall [2,4,11,12]. In the case of our patient, the suspected mechanism behind the extensive gastric ischemia and perforation was the use of the artisanal hospital-made bubble CPAP.
Most neonates with gastric perforation present with abrupt abdominal distension and nonspecific symptoms, such as lethargy, fever, intolerance to feeds, and respiratory distress. Physical exam is limited to abdominal induration and pain on abdominal palpation [5,10]. Massive pneumoperitoneum on abdominal radiographs, suggestive of gastric perforation, is a commonly seen imaging finding in these patients [7]. The location of the gastric perforation can vary, though most are found on the greater curvature (37–73 %) and the anterior wall [5,7]. Likewise, the size of the perforation can vary widely, although those measuring 1.5 cm or greater have been associated with increased mortality [3,5,6,13].
Initial conservative treatment with peritoneal drainage may be useful in critically unstable neonates, although surgery is almost always required. Primary repair of the perforation is preferred in patients with punctiform perforations, while those with larger perforations may require debridement of any necrotic tissue and gastrorrhaphy or partial gastrectomy [6,7]. There are few reported cases of neonatal perforation requiring a total gastrectomy [2,3]. The options for reconstruction after gastrectomy in neonates are mostly extrapolated from the adult gastric cancer population, and are classified according to whether they preserve the continuity of the duodenum or not [14,15].Preserving duodenal continuity is ideal, as it regulates intestinal motility and stimulates many cells with hormonal, paracrine and neurocrine effects that help in the digestion of the food. Duodenal preservation may be accomplished by a Roux-en-Y double-tract esophagojejunostomy or an esophagojejunostomy with functional jejunal interposition (Longmire procedure) [14,15]. Among the few reported cases of neonates who underwent gastrectomy, several repair techniques, including colonic interposition, delayed Hunt-Lawrence pouch, and jejunostomy, have been described [2,3,15].
When choosing a reconstructive procedure without duodenal passage, the most important consideration is to prevent biliary reflux into the esophagus. This is accomplished by a Roux-en-Y esophagojejunostomy, which may or may not be accompanied by the creation of a jejunal pouch. The jejunal pouch was designed to replace the stomach and increase the reservoir capacity of the jejunal substituent (Hunt-Lawrence procedure), decreasing the risk of dumping syndrome and biliary regurgitation while facilitating digestion [[16], [17], [18]]. The creation of a jejunal pouch, however, is not risk-free, as ischemia may occur in the upper acute angle when rotating the jejunum to create the pouch or in the case of a shortened jejunum or mesentery [16,18]. In the case of our patient, a gastrectomy was warranted due to the extensive anterior gastric perforation, surrounding tissue necrosis, and posterior wall ischemia. Given the small size of the unused jejunum and his intraoperative hemodynamic lability, we not to construct a jejunal pouch for the esophagojejunostomy. Gastrectomy should be avoided when possible to prevent nutritional deficiencies, dumping syndrome, reflux esophagitis, and failure to thrive. The pouchless esophagojejunal reconstruction can be a viable surgical strategy when pouch creation is not feasible or is technically challenging due to factors such as hemodynamic instability or a very small intestine. In such cases, a pouchless reconstruction can be a viable surgical option, leading to good outcomes, including adequate growth and nutritional status thanks to a multidisciplinary approach.
Patients who undergo gastrectomy are at an increased risk of severe nutritional deficiencies and failure to thrive. Gastrectomy results in the loss of digestive enzymes, reduced stimulation of pancreatic and biliary secretions, inappropriate mixing of food with pancreatic enzymes and bile, increased bowel motility, and excessive bacterial colonization. These patients may also develop anemia, primarily due to the malabsorption of several nutrients. Microcytic anemia may result from iron malabsorption, as the absence of gastric acid impedes the reduction of ferric iron (Fe^3+^) to ferrous iron (Fe^2+^) which is more readily absorbed in the duodenum. Conversely, macrocytic anemia stems from the absence of parietal cells, found mainly in the fundus and body of the stomach, which leads to intrinsic factor deficiency and consequently malabsorption of vitamin B12 in the ileum. The lack of gastric acid favors bacterial overgrowth, which damages the gastrointestinal epithelium and deconjugates bile acids, leading to fat malabsorption. Meanwhile, accelerated gastrointestinal transit reduces calcium absorption, and the presence of steatorrhea produces insoluble calcium soaps, leading to bone metabolism disorders. Accelerated transit also alters the glucose uptake, as well as the absorption of lipids and proteins [14,16].
To reduce the risk of these complications, our patient was managed by a multidisciplinary team composed of neonatologists, gastroenterologists, nutritionists, and pediatric surgeons. He was fed with a hypercaloric formula supplemented with vitamins B12 and D, pancreatic enzymes, ferrous sulfate, and calcium during the postoperative period, and has been followed in each specialty's respective outpatient clinic. Thanks to this multidisciplinary approach, the patient has been able to achieve an adequate nutritional status for his age without nutritional deficiencies.
Conclusion
4
Neonatal gastric perforation is a rare and severe condition with high morbidity and mortality, particularly in preterm and low-birthweight infants. To our knowledge, this case represents the first reported neonatal total gastrectomy due to suspected barotrauma reconstructed with a pouchless Roux-en-Y esophagojejunostomy. Despite the challenges, multidisciplinary postoperative care enabled a successful recovery with adequate growth and nutrition. Our experience suggests that pouchless esophagojejunal reconstruction can be a viable option leading to good outcomes when pouch creation is not feasible or technically challenging due to anatomic factors or hemodynamic instability.
CRediT authorship contribution statement
- Harold Castro Anaya– Data collection and analysis
- Arturo Javier Cavazos Castro – Data collection, analysis and writing paper
- María Elena Ortega Ramírez– Study concept
- José Asz Sigall – Study concept, interpretation
- Claudia Elitania Espinosa Guerrero – Data collection and analysis
- Horacio G. Carvajal – Analysis and writing paper.
Informed consent
Parental consent for minors: Written informed consent was obtained from the patient's parents for publication and any accompanying images.
Ethical approval
This case report is exempt from ethical approval by our institution. The ethics committee at our institution, does not review case reports that do not involve prospective intervention or significant risk to the patient. Due to this case report is a retrospective, single case with anonymized data, it was not considered to be reviewed.
Guarantor
Arturo Javier Cavazos Castro is the guarantor of the work.
Authorship
All authors attest that they meet the current ICMJE criteria for Authorship.
Funding
This research did not receive any specific grants from funding agencies in the public, commercial, or non-profit sectors.
Declaration of competing interest
The authors declare that they have no competing economic interests or known personal relationships that could have influenced the work reported in this document.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Iacusso C.Boscarelli A.Fusaro F.Bagolan P.Morini F.Pathogenetic and prognostic factors for neonatal gastric perforation: personal experience and systematic review of the literature Front. Pediatr.620186110.3389/fped.2018.0006129670869 PMC 5893822 · doi ↗ · pubmed ↗
- 2Theodorou C.M.Chen P.Vanover M.A.Saadai P.Brown E.G.Haas K.B.Total gastrectomy with delayed Hunt-Lawrence pouch reconstruction for neonatal gastric perforation presenting with hematemesis J Pediatr Surg Case Rep 63202010168610.1016/j.epsc.2020.101686 PMC 765462333184604 · doi ↗ · pubmed ↗
- 3Durham M.M.Ricketts R.R.Neonatal gastric perforation and necrosis with Hunt-Lawrence Pouch reconstruction J. Pediatr. Surg.34199964965110.1016/S 0022-3468(99)90097-010235346 · doi ↗ · pubmed ↗
- 4Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int J Surg Lond Engl.10952023113610.1097/JS 9.0000000000000373 PMC 1038940137013953 · doi ↗ · pubmed ↗
- 5Babayigit A.Ozaydın S.Cetinkaya M.Sander S.Neonatal gastric perforations in very low birth weight infants: a single center experience and review of the literature Pediatr. Surg. Int.342018798410.1007/s 00383-017-4205-129079904 · doi ↗ · pubmed ↗
- 6Yang C.-Y.Lien R.Fu R.-H.Chu S.-M.Hsu J.-F.Lai J.-Y.Prognostic factors and concomitant anomalies in neonatal gastric perforation J. Pediatr. Surg.5020151278128210.1016/j.jpedsurg.2015.04.00725957026 · doi ↗ · pubmed ↗
- 7Reams G.B.Dunaway J.B.Walls W.L.Neonatal gastric perforation with survival Pediatrics 3119639710210.1542/peds.31.1.9713973417 · doi ↗ · pubmed ↗
- 8Lin C.-M.Lee H.-C.Kao H.-A.Hung H.-Y.Hsu C.-H.Yeung C.-Y.Neonatal gastric perforation: report of 15 cases and review of the literature Pediatr. Neonatol.492008657010.1016/S 1875-9572(08)60015-718947001 · doi ↗ · pubmed ↗