Incidence, Demographics, and Service Utilization of Patients Referred for Renal Replacement Therapy at the Instituto Mexicano del Seguro Social (IMSS) Michoacán: A Retrospective Analysis
Christian Diaz de Leon Castañeda, Venice Chávez Valencia, Cleto Álvarez Aguilar, Virginia Robinson Fuentes

TL;DR
This study analyzes kidney disease treatment trends in Michoacán, Mexico, finding rising dialysis referrals and regional disparities in care.
Contribution
The study identifies regional variations in RRT incidence and service utilization within IMSS Michoacán, highlighting the need for infrastructure improvements.
Findings
RRT referral rates increased over time, with a 2021 state incidence of 28.42 per 100,000 population.
Patients in Zitácuaro and the region of interest were significantly younger at dialysis initiation.
HD service provision increased over time, but access inequalities persist across regions.
Abstract
Background: Chronic kidney disease (CKD) is a health condition with high tangible and intangible implications for patients, health systems, and society in Mexico. This study aims to analyze the incidence, demographics, and service utilization of patients referred for renal replacement therapy (RRT) involving peritoneal dialysis (PD) or hemodialysis (HD) in Care units of the Instituto Mexicano del Seguro Social (IMSS) in the state of Michoacán, Mexico. Methods: A database from IMSS Michoacán containing information from January 2007 to September 2023 was analyzed. Special analyses were performed by subdelegations of adscription of the patients and according to a "region of interest" comprising three municipalities in eastern Michoacán (Zinapecuaro, Hidalgo, and Maravatío). This analysis included incidence rates of patient referrals, mean age at dialysis initiation, and percentages of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
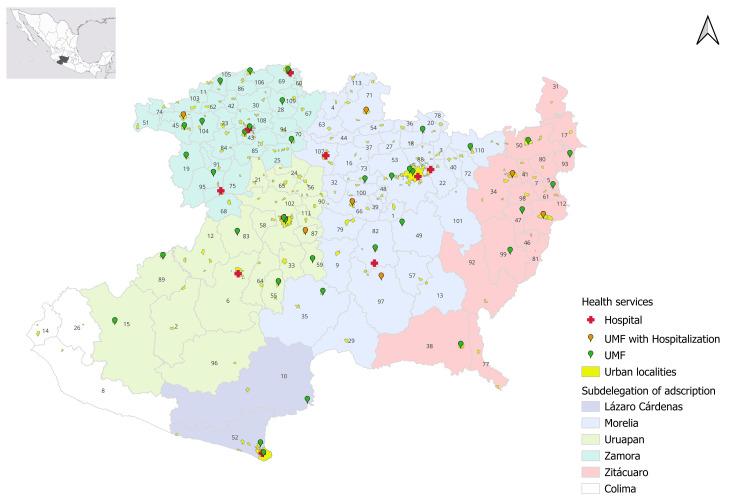 Figure 1
Figure 1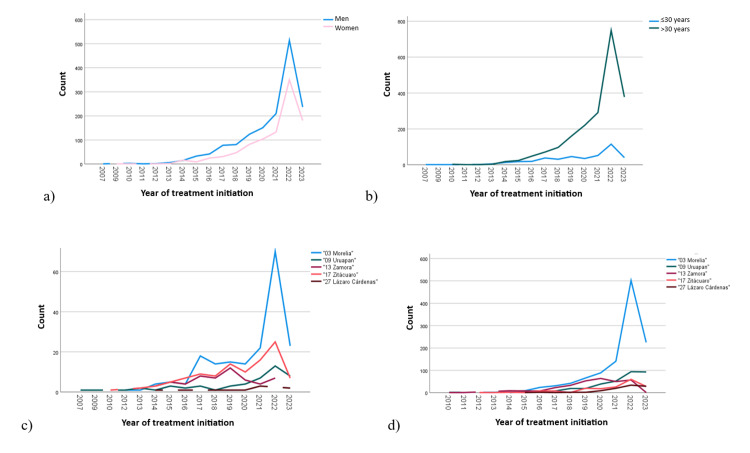 Figure 2
Figure 2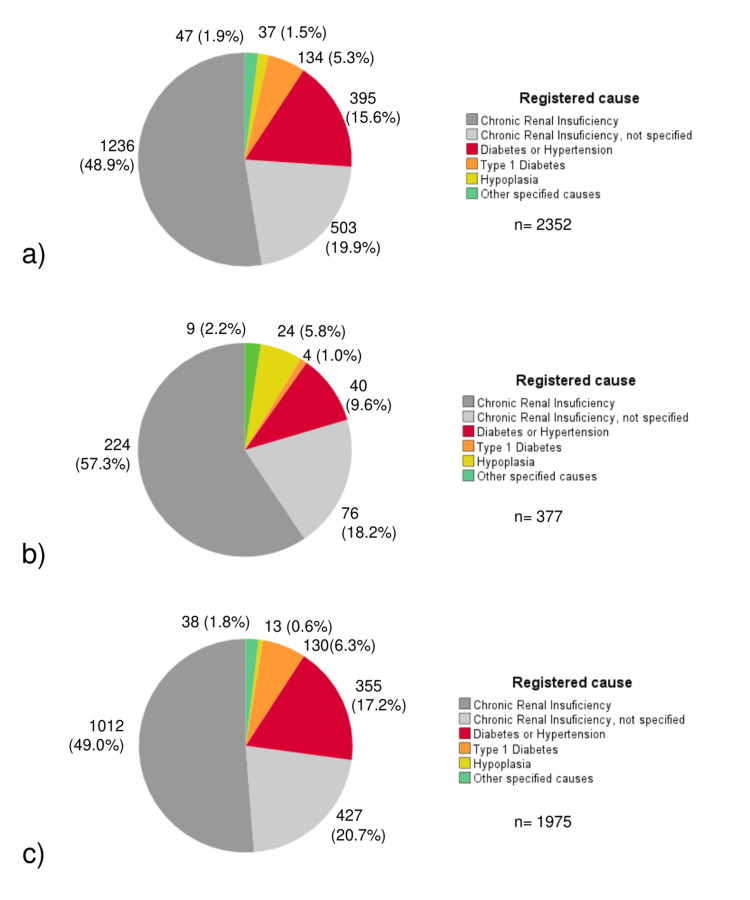 Figure 3
Figure 3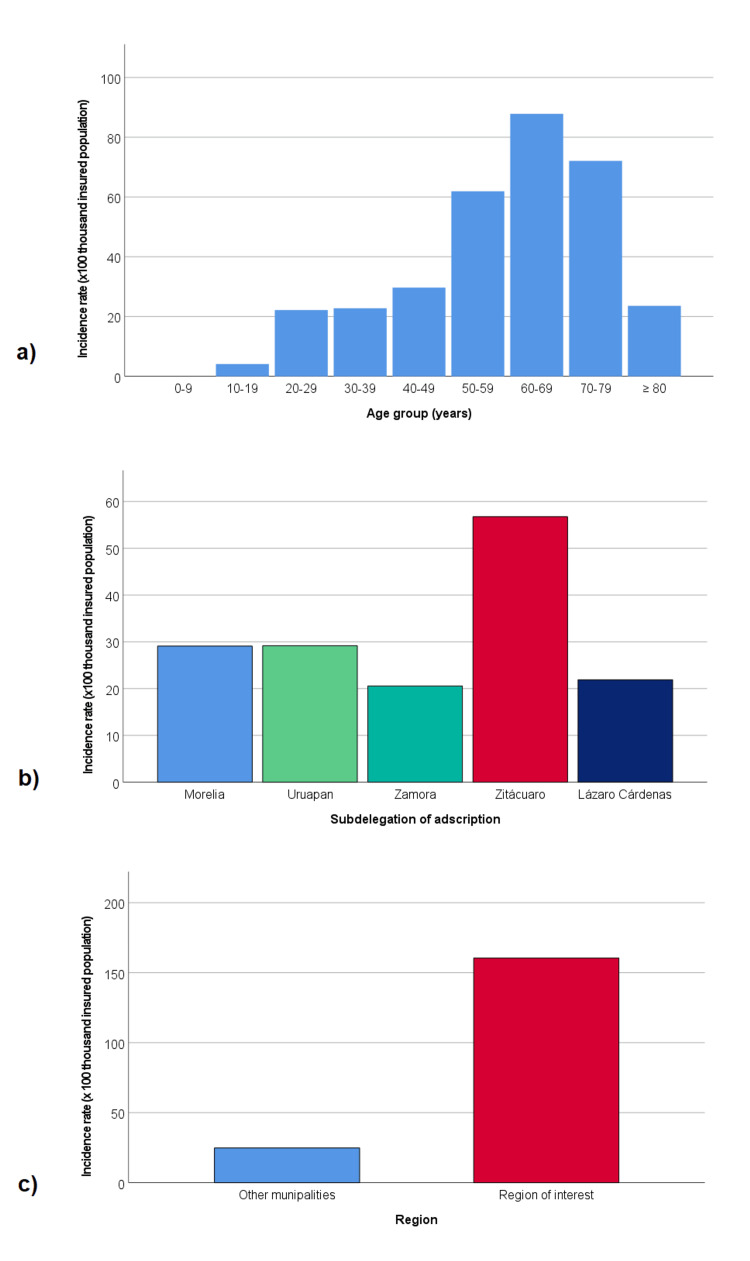 Figure 4
Figure 4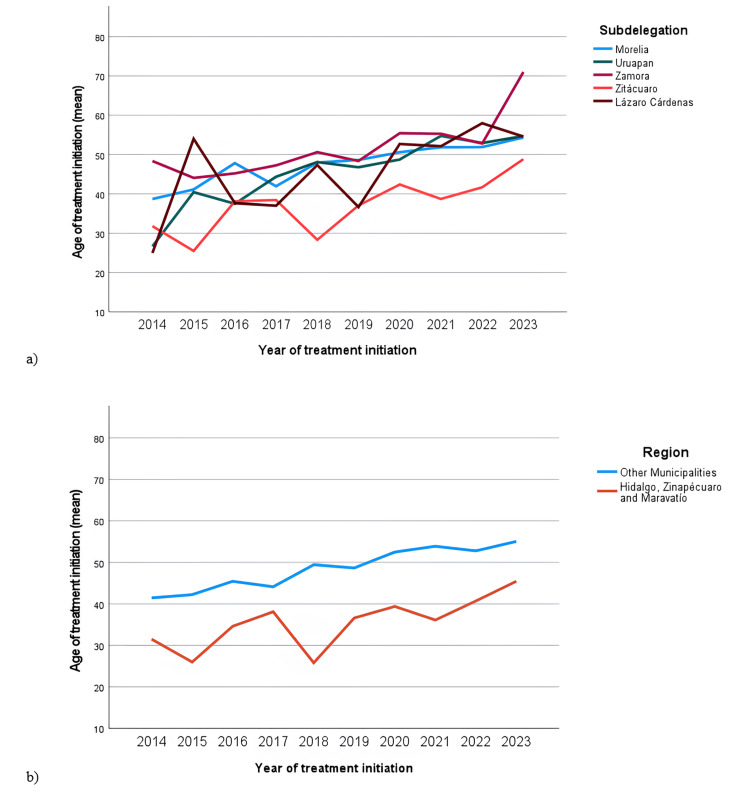 Figure 5
Figure 5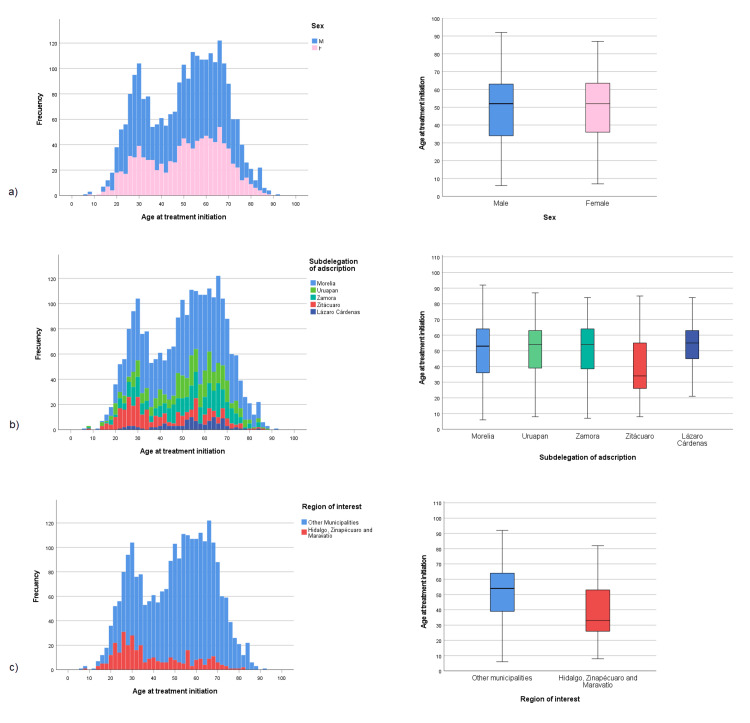 Figure 6
Figure 6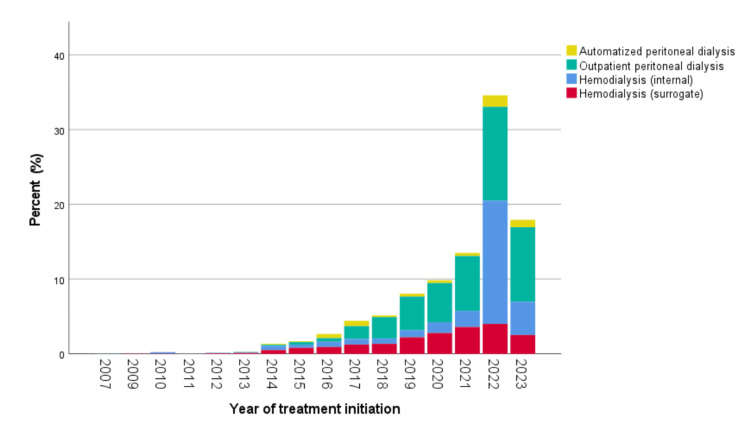 Figure 7
Figure 7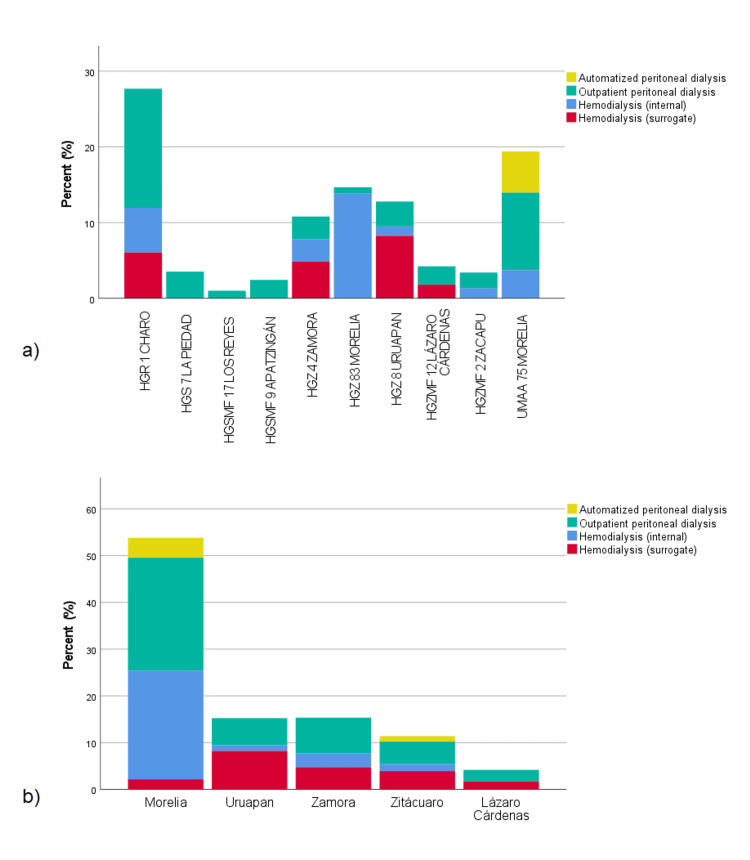 Figure 8
Figure 8| Variables | 2007 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | TOTAL | ||||||||||||||||
| Age (years) | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | < 30 | > 30 | |
| Foreigners, n | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 2 | 0 | 2 | 0 | 2 | 10 |
| Morelia, n | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 1 | 0 | 1 | 2 | 4 | 6 | 5 | 9 | 4 | 24 | 18 | 31 | 14 | 42 | 15 | 66 | 14 | 89 | 22 | 141 | 70 | 502 | 23 | 225 | 1330 |
| Uruapan, n | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 2 | 0 | 1 | 1 | 3 | 5 | 2 | 6 | 3 | 8 | 1 | 19 | 3 | 19 | 4 | 39 | 7 | 52 | 13 | 94 | 8 | 93 | 386 |
| Zamora, n | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 3 | 9 | 5 | 8 | 4 | 8 | 8 | 23 | 7 | 33 | 12 | 53 | 6 | 64 | 4 | 50 | 7 | 57 | 0 | 1 | 364 |
| Zitácuaro, n | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 2 | 1 | 3 | 2 | 5 | 1 | 7 | 8 | 9 | 8 | 8 | 1 | 14 | 20 | 10 | 18 | 16 | 26 | 25 | 60 | 7 | 28 | 281 |
| Lázaro Cárdenas, n | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 2 | 0 | 1 | 1 | 2 | 1 | 2 | 1 | 9 | 3 | 20 | 0 | 34 | 2 | 29 | 110 |
| TOTAL | 1 | 0 | 1 | 0 | 1 | 3 | 0 | 1 | 2 | 1 | 5 | 3 | 13 | 18 | 18 | 24 | 19 | 48 | 38 | 71 | 31 | 97 | 46 | 160 | 35 | 220 | 52 | 291 | 115 | 749 | 40 | 378 | 2481 |
| Categories | Michoacán population in 2020, n | IMSS Michoacán-affiliated population in 2020, n (%) | New cases admitted in 2021, n | Incidence rate in 2021 (per 100,000 insured individuals) | |
| Sex | Men | 2,306,341 | 584,464 (25.3) | 210 | 35.93 |
| Women | 2,442,505 | 622,581 (25.5) | 133 | 21.36 | |
| Age group (years) | 0-9 | 871,455 | 187,920 (21.6) | 0 | 0.00 |
| 10-19 | 834,612 | 194,596 (23.3) | 8 | 4.11 | |
| 20-29 | 757,999 | 194,039 (25.6) | 43 | 22.16 | |
| 30-39 | 663,710 | 179,870 (27.1) | 41 | 22.79 | |
| 40-49 | 569,843 | 151,597 (26.6) | 45 | 29.68 | |
| 50-59 | 445,998 | 122,739 (27.5) | 76 | 61.92 | |
| 60-69 | 318,853 | 96,758 (30.3) | 85 | 87.85 | |
| 70-79 | 181,270 | 54,073 (29.8) | 39 | 72.12 | |
| ≥ 80 | 101,576 | 25,439 (25.0) | 6 | 23.59 | |
| Not specified | 3,500 | 14 (0.4) | - | - | |
| Subdelegation of adscription | Non-residents | - | - | 2 | |
| Morelia | 1,879,109 | 560,086 (29.8) | 163 | 29.10 | |
| Uruapan | 907,134 | 202,204 (22.3) | 59 | 29.18 | |
| Zamora | 1,016,491 | 262,478 (25.8) | 54 | 20.57 | |
| Zitácuaro | 683,306 | 74,009 (10.8) | 42 | 56.75 | |
| Lázaro Cárdenas | 216,335 | 105,046 (48.6) | 23 | 21.90 | |
| Region of interest | Non-residents | - | - | 2 | - |
| Region of interest | 264,028 | 30,530 (11.6) | 49 | 160.50 | |
| Other municipalities | 4,484,818 | 1,176,515 (26.2) | 292 | 24.82 | |
| TOTAL | - | 4,748,846 | 1,207,045 (25.42%) | 343 | 28.42 |
| Categories | Total, n | Sex, n (%) | Age at dialysis initiation | Age category at dialysis initiation, n (%) | |||||||||||
| F | M | Mean | SD | Min | Max | ≤ 30 years | > 30 years | ||||||||
| n | % | n | % | n | % | n | % | ||||||||
| Subdelegation of adscription | Morelia | 1330 | 538 | 40.5 | 792 | 59.5 | 51.28 | 16.86 | 6.92 | 92.58 | 191 | 14.4 | 1139 | 85.6 | |
| Uruapan | 386 | 146 | 37.8 | 240 | 62.2 | 51.89 | 16.26 | 8.00 | 87.67 | 50 | 13.0 | 336 | 87.0 | ||
| Zamora | 364 | 122 | 33.5 | 242 | 66.5 | 51.41 | 16.30 | 7.08 | 84.50 | 56 | 15.4 | 308 | 84.6 | ||
| Zitácuaro | 281 | 119 | 42.3 | 162 | 57.7 | 40.68 | 17.44 | 8.92 | 85.33 | 107 | 38.1 | 174 | 61.9 | ||
| Lázaro Cárdenas | 110 | 52 | 47.3 | 58 | 52.7 | 53.82 | 13.57 | 21.83 | 84.92 | 10 | 9.1 | 100 | 90.9 | ||
| Region of interest | Other municipalities | 2143 | 838 | 39.1 | 1305 | 60.9 | 51.95 | 16.38 | 6.92 | 92.58 | 284 | 13.3 | 1859 | 86.7 | |
| Region of interest | 328 | 139 | 42.4 | 189 | 57.6 | 39.50 | 16.82 | 8.92 | 82.58 | 130 | 39.6 | 198 | 60.4 | ||
| TOTAL | 2471 | 977 | 39.5 | 1494 | 60.5 | 50.30 | 17.00 | 6.92 | 92.58 | 417 | 16.8 | 2064 | 83.2 | ||
| Subdelegation | Adscription Unit | Total, n | Sex | Age at dialysis initiation | Age category at dialysis initiation, n (%) | ||||||||||||
| F | M | Mean | SD | Min | Max | ≤ 30 years | > 30 years | ||||||||||
| n | % | n | % | n | % | n | % | ||||||||||
| Morelia | HGSMF 24 Pedernales | 11 | 6 | 54.5 | 5 | 45.5 | 53.55 | 14.72 | 28.17 | 75.42 | 1 | 9.1 | 10 | 90.9 | |||
| HGZMF 2 Zacapu | 74 | 26 | 35.1 | 48 | 64.9 | 53.43 | 15.39 | 21.17 | 87.33 | 8 | 10.8 | 66 | 89.2 | ||||
| UMF 3 Quiroga | 13 | 8 | 61.5 | 5 | 38.5 | 53.55 | 17.19 | 25.83 | 83.17 | 1 | 7.7 | 12 | 92.3 | ||||
| UMF 42 Cuitzeo | 30 | 16 | 53.3 | 14 | 46.7 | 50.16 | 16.47 | 23.33 | 80.83 | 5 | 16.7 | 25 | 83.3 | ||||
| UMF 43 Churumuco | 1 | 1 | 100.0 | 0 | 0.0 | 50.58 | 50.58 | 50.58 | 0 | 0.0 | 1 | 100.0 | |||||
| UMF 46 La Huacana | 3 | 1 | 33.3 | 2 | 66.7 | 53.81 | 19.25 | 31.58 | 65.25 | 0 | 0.0 | 3 | 100.0 | ||||
| UMF 65 Villa Madero | 12 | 4 | 33.3 | 8 | 66.7 | 55.58 | 10.72 | 37.92 | 74.75 | 0 | 0.0 | 12 | 100.0 | ||||
| UMF 70 Zinapécuaro | 104 | 40 | 38.5 | 64 | 61.5 | 42.29 | 16.61 | 16.08 | 81.08 | 31 | 29.8 | 73 | 70.2 | ||||
| UMF 71 Morelia | 5 | 1 | 20.0 | 4 | 80.0 | 59.23 | 16.25 | 39.33 | 83.67 | 0 | 0.0 | 5 | 100.0 | ||||
| UMF 74 Tacámbaro | 28 | 13 | 46.4 | 15 | 53.6 | 49.57 | 17.32 | 16.58 | 79.17 | 5 | 17.9 | 23 | 82.1 | ||||
| UMF 80 Morelia | 335 | 131 | 39.1 | 204 | 60.9 | 54.88 | 16.14 | 6.92 | 86.50 | 28 | 8.4 | 307 | 91.6 | ||||
| UMF 84 Tacicuaro | 112 | 65 | 58.0 | 47 | 42.0 | 50.71 | 14.82 | 16.58 | 76.83 | 12 | 10.7 | 100 | 89.3 | ||||
| UMF 85 Tarímbaro | 181 | 68 | 37.6 | 113 | 62.4 | 47.64 | 16.32 | 14.92 | 78.25 | 35 | 19.3 | 146 | 80.7 | ||||
| UMF 75 -UMAA 254 Morelia | 282 | 103 | 36.5 | 179 | 63.5 | 52.15 | 17.61 | 15.92 | 92.58 | 38 | 13.5 | 244 | 86.5 | ||||
| UMFH 20 Pátzcuaro | 94 | 38 | 40.4 | 56 | 59.6 | 55.30 | 15.81 | 12.17 | 84.67 | 8 | 8.5 | 86 | 91.5 | ||||
| UMFH 25 Puruarán | 13 | 4 | 30.8 | 9 | 69.2 | 46.32 | 19.52 | 19.83 | 75.08 | 5 | 38.5 | 8 | 61.5 | ||||
| UMFH 64 Puruándiro | 32 | 13 | 40.6 | 19 | 59.4 | 40.69 | 18.89 | 20.25 | 76.33 | 14 | 43.8 | 18 | 56.3 | ||||
| Total | 1330 | 538 | 40.5 | 792 | 59.5 | 51.28 | 16.86 | 6.92 | 92.58 | 191 | 14.4 | 1139 | 85.6 | ||||
| Uruapan | HGSMF 9 Apatzingán | 104 | 43 | 41.3 | 61 | 58.7 | 50.18 | 17.43 | 13.08 | 84.42 | 18 | 17.3 | 86 | 82.7 | |||
| UMF 11 Nueva Italia | 23 | 9 | 39.1 | 14 | 60.9 | 50.13 | 17.20 | 19.58 | 82.42 | 4 | 17.4 | 19 | 82.6 | ||||
| UMF 52 Nuevo Urecho | 2 | 0 | 0.0 | 2 | 100.0 | 47.83 | 26.16 | 29.33 | 66.33 | 1 | 50.0 | 1 | 50.0 | ||||
| UMF 57 Tancítaro | 9 | 2 | 22.2 | 7 | 77.8 | 48.40 | 11.59 | 23.08 | 59.42 | 1 | 11.1 | 8 | 88.9 | ||||
| UMF 58 Tepalcatepec | 2 | 0 | 0.0 | 2 | 100.0 | 72.08 | 3.42 | 69.67 | 74.50 | 0 | 0.0 | 2 | 100.0 | ||||
| UMF 73 Uruapan | 2 | 2 | 100.0 | 0 | 0.0 | 71.33 | 0.94 | 70.67 | 72.00 | 0 | 0.0 | 2 | 100.0 | ||||
| UMF 76 Uruapan | 78 | 25 | 32.1 | 53 | 67.9 | 53.32 | 15.39 | 19.42 | 85.00 | 9 | 11.5 | 69 | 88.5 | ||||
| UMF 81 Uruapan | 151 | 62 | 41.1 | 89 | 58.9 | 52.49 | 15.52 | 8.00 | 87.67 | 14 | 9.3 | 137 | 90.7 | ||||
| UMFH 26 Taretán | 15 | 3 | 20.0 | 12 | 80.0 | 50.31 | 19.75 | 15.75 | 77.25 | 3 | 20.0 | 12 | 80.0 | ||||
| Total | 386 | 146 | 37.8 | 240 | 62.2 | 51.89 | 16.26 | 8.00 | 87.67 | 50 | 13.0 | 336 | 87.0 | ||||
| Zamora | HGSMF 17 Los Reyes | 35 | 13 | 37.1 | 22 | 62.9 | 53.97 | 15.11 | 22.00 | 79.50 | 4 | 11.4 | 31 | 88.6 | |||
| UMF 13 Cotija | 7 | 3 | 42.9 | 4 | 57.1 | 52.67 | 17.24 | 26.33 | 70.58 | 1 | 14.3 | 6 | 85.7 | ||||
| UMF 21 Jacona | 32 | 10 | 31.3 | 22 | 68.8 | 53.50 | 17.54 | 22.33 | 83.83 | 4 | 12.5 | 28 | 87.5 | ||||
| UMF 28 Sta. Clara | 6 | 1 | 16.7 | 5 | 83.3 | 36.04 | 16.43 | 22.00 | 62.75 | 4 | 66.7 | 2 | 33.3 | ||||
| UMF 54 Purépero | 3 | 0 | 0.0 | 3 | 100.0 | 52.53 | 22.45 | 27.75 | 71.50 | 1 | 33.3 | 2 | 66.7 | ||||
| UMF 6 Jiquilpan | 8 | 4 | 50.0 | 4 | 50.0 | 48.34 | 13.32 | 29.83 | 65.08 | 1 | 12.5 | 7 | 87.5 | ||||
| UMF 68 Vista Hermosa | 5 | 0 | 0.0 | 5 | 100.0 | 51.53 | 20.76 | 29.08 | 75.58 | 1 | 20.0 | 4 | 80.0 | ||||
| UMF 72 Yurécuaro | 21 | 5 | 23.8 | 16 | 76.2 | 42.58 | 15.02 | 18.92 | 83.08 | 5 | 23.8 | 16 | 76.2 | ||||
| UMF 77 La Piedad | 95 | 32 | 33.7 | 63 | 66.3 | 49.09 | 16.69 | 17.17 | 77.92 | 19 | 20.0 | 76 | 80.0 | ||||
| UMF 82 Zamora | 126 | 45 | 35.7 | 81 | 64.3 | 54.54 | 15.44 | 7.08 | 84.50 | 11 | 8.7 | 115 | 91.3 | ||||
| UMFH 5 Sahuayo | 26 | 9 | 34.6 | 17 | 65.4 | 49.75 | 15.86 | 18.83 | 68.17 | 5 | 19.2 | 21 | 80.8 | ||||
| Total | 364 | 122 | 33.5 | 242 | 66.5 | 51.41 | 16.30 | 7.08 | 84.50 | 56 | 15.4 | 308 | 84.6 | ||||
| Zitácuaro | UMF 10 Jungapeo | 9 | 2 | 22.2 | 7 | 77.8 | 50.36 | 16.13 | 29.17 | 76.67 | 1 | 11.1 | 8 | 88.9 | |||
| UMF 37 Mineral Angangeo | 11 | 4 | 36.4 | 7 | 63.6 | 58.21 | 13.00 | 38.42 | 76.67 | 0 | 0.0 | 11 | 100.0 | ||||
| UMF 48 Huetamo | 9 | 1 | 11.1 | 8 | 88.9 | 46.68 | 11.66 | 30.83 | 68.42 | 0 | 0.0 | 9 | 100.0 | ||||
| UMF 50 Maravatío | 45 | 15 | 33.3 | 30 | 66.7 | 37.97 | 16.40 | 13.42 | 72.83 | 23 | 51.1 | 22 | 48.9 | ||||
| UMF 61 Tuzantla | 3 | 0 | 0.0 | 3 | 100.0 | 45.89 | 15.29 | 28.33 | 56.25 | 1 | 33.3 | 2 | 66.7 | ||||
| UMF 79 Tlalpujahua | 8 | 3 | 37.5 | 5 | 62.5 | 41.97 | 19.84 | 15.42 | 69.00 | 3 | 37.5 | 5 | 62.5 | ||||
| UMFH 18 Zitácuaro | 17 | 10 | 58.8 | 7 | 41.2 | 52.08 | 19.23 | 21.58 | 85.33 | 3 | 17.6 | 14 | 82.4 | ||||
| UMFH 19 Cd. Hidalgo | 179 | 84 | 46.9 | 95 | 53.1 | 38.27 | 16.94 | 8.92 | 82.58 | 76 | 42.5 | 103 | 57.5 | ||||
| Total | 281 | 119 | 42.3 | 162 | 57.7 | 40.68 | 17.44 | 8.92 | 85.33 | 107 | 38.1 | 174 | 61.9 | ||||
| Lázaro Cárdenas | HGZMF 12 Lázaro Cárdenas | 26 | 16 | 61.5 | 10 | 38.5 | 56.68 | 13.10 | 23.92 | 76.42 | 2 | 7.7 | 24 | 92.3 | |||
| UMF 23 Infiernillo | 2 | 0 | 0.0 | 2 | 100.0 | 44.79 | 19.62 | 30.92 | 58.67 | 0 | 0.0 | 2 | 100.0 | ||||
| UMF 27 La Mira | 13 | 5 | 38.5 | 8 | 61.5 | 58.98 | 11.80 | 27.17 | 73.58 | 1 | 7.7 | 12 | 92.3 | ||||
| UMF 31 Guacamayas | 29 | 16 | 55.2 | 13 | 44.8 | 52.77 | 11.49 | 21.83 | 78.17 | 1 | 3.4 | 28 | 96.6 | ||||
| UMF 78 Lázaro Cárdenas | 40 | 15 | 37.5 | 25 | 62.5 | 51.50 | 15.25 | 24.42 | 84.92 | 6 | 15.0 | 34 | 85.0 | ||||
| Total | 110 | 52 | 47.3 | 58 | 52.7 | 53.82 | 13.57 | 21.83 | 84.92 | 10 | 9.1 | 100 | 90.9 | ||||
| TOTAL | 2471 | 977 | 39.5 | 1494 | 60.5 | 50.30 | 17.00 | 6.92 | 92.58 | 417 | 16.8 | 2064 | 83.2 | ||||
| Care Unit | Total, n | Sex | Age at dialysis initiation (years) | Age category at dialysis initiation | |||||||||||||
| F | M | Mean | SD | Min | Max | Age ≤ 30 years | Age > 30 years | ||||||||||
| n | % | n | % | n | % | n | % | ||||||||||
| HGR 1 Charo | 687 | 284 | 41.3 | 403 | 58.7 | 47.01 | 17.93 | 8.92 | 87.83 | 167 | 24.2 | 524 | 75.8 | ||||
| HGS 7 La Piedad | 94 | 33 | 35.1 | 61 | 64.9 | 49.34 | 16.29 | 17.17 | 83.08 | 18 | 19.1 | 76 | 80.9 | ||||
| HGSMF 17 Los Reyes | 27 | 10 | 37.0 | 17 | 63.0 | 51.71 | 14.99 | 22.00 | 74.42 | 3 | 11.1 | 24 | 88.9 | ||||
| HGSMF 9 Apatzingán | 63 | 31 | 49.2 | 32 | 50.8 | 51.15 | 16.92 | 13.08 | 79.33 | 8 | 12.7 | 55 | 87.3 | ||||
| HGZ 4 Zamora | 241 | 79 | 32.8 | 162 | 67.2 | 52.12 | 16.39 | 7.08 | 84.50 | 34 | 14.0 | 208 | 86.0 | ||||
| HGZ 8 Uruapan | 325 | 116 | 35.7 | 209 | 64.3 | 52.11 | 16.13 | 8.00 | 87.67 | 42 | 12.9 | 283 | 87.1 | ||||
| HGZ 83 Morelia | 382 | 157 | 41.1 | 225 | 58.9 | 52.11 | 16.81 | 16.58 | 87.58 | 41 | 10.7 | 343 | 89.3 | ||||
| HGZMF 12 Lázaro Cárdenas | 110 | 52 | 47.3 | 58 | 52.7 | 53.80 | 13.51 | 21.83 | 84.92 | 10 | 9.0 | 101 | 91.0 | ||||
| HGZMF 2 Zacapu | 89 | 34 | 38.2 | 55 | 61.8 | 51.36 | 15.98 | 20.25 | 78.58 | 14 | 15.4 | 77 | 84.6 | ||||
| UMF 75 -UMAA 254 Morelia | 453 | 181 | 40.0 | 272 | 60.0 | 50.45 | 17.22 | 6.92 | 92.58 | 80 | 17.7 | 373 | 82.3 | ||||
| TOTAL | 2471 | 977 | 39.5 | 1494 | 60.5 | 50.30 | 17.00 | 6.92 | 92.58 | 417 | 16.8 | 2064 | 83.2 | ||||
| Service | 2007-2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | TOTALa | ||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | |
| Automated Peritoneal Dialysis | 7 | 7.7 | 15 | 22.4 | 18 | 16.5 | 6 | 4.7 | 10 | 4.9 | 10 | 3.9 | 11 | 3.2 | 32 | 3.7 | 20 | 4.8 | 129 | 5.2 |
| Continuous Ambulatory Peritoneal Dialysis | 16 | 17.6 | 12 | 17.9 | 42 | 38.5 | 73 | 57.0 | 114 | 55.3 | 135 | 52.9 | 191 | 55.7 | 310 | 35.9 | 223 | 53.3 | 1116 | 45.0 |
| Internal Hemodialysisb | 31 | 34.1 | 16 | 23.9 | 19 | 17.4 | 17 | 13.3 | 25 | 12.1 | 38 | 14.9 | 52 | 15.2 | 426 | 49.3 | 113 | 27.0 | 737 | 29.7 |
| Subrogated Hemodialysis | 37 | 40.7 | 24 | 35.8 | 30 | 27.5 | 32 | 25.0 | 57 | 27.7 | 72 | 28.2 | 89 | 25.9 | 96 | 11.1 | 62 | 14.8 | 499 | 20.1 |
| TOTAL | 91 | 100 | 67 | 100 | 109 | 100 | 128 | 100 | 206 | 100 | 255 | 100 | 343 | 100 | 864 | 100 | 418 | 100 | 2481 | 100.0 |
| Service | Automated peritoneal dialysis | Continuous ambulatory peritoneal dialysis | Internal hemodialysis | Subcontracted hemodialysis | TOTAL | |||||
| n | % (row) | n | % (row) | n | % (row) | n | % (row) | n | % (column) | |
| by Care Unit | ||||||||||
| HGR 1 Charo | 0 | 0.0 | 404 | 56.5 | 153 | 21.4 | 158 | 22.1 | 715 | 28.3 |
| HGS 7 La Piedad | 0 | 0.0 | 94 | 100.0 | 0 | 0.0 | 0 | 0.0 | 94 | 3.7 |
| HGSMF 17 Los Reyes | 0 | 0.0 | 27 | 100.0 | 0 | 0.0 | 0 | 0.0 | 27 | 1.1 |
| HGSMF 9 Apatzingán | 0 | 0.0 | 63 | 100.0 | 0 | 0.0 | 0 | 0.0 | 63 | 2.5 |
| HGZ 4 Zamora | 0 | 0.0 | 80 | 31.4 | 64 | 25.1 | 111 | 43.5 | 255 | 10.1 |
| HGZ 8 Uruapan | 0 | 0.0 | 86 | 26.1 | 33 | 10.0 | 211 | 63.9 | 330 | 13.1 |
| HGZ 83 Morelia | 0 | 0.0 | 15 | 3.9 | 369 | 96.1 | 0 | 0.0 | 384 | 15.2 |
| HGZMF 12 Lázaro Cárdenas | 0 | 0.0 | 65 | 57.5 | 0 | 0.0 | 48 | 42.5 | 113 | 4.5 |
| HGZMF 2 Zacapu | 0 | 0.0 | 56 | 61.5 | 35 | 38.5 | 0 | 0.0 | 91 | 3.6 |
| UMF 75 - UMAA 254 Morelia | 130 | 28.6 | 230 | 50.7 | 94 | 20.7 | 0 | 0.0 | 454 | 18.0 |
| by Subdelegation of Adscription | ||||||||||
| Foreigners | 1 | 7.1 | 3 | 21.4 | 4 | 28.6 | 6 | 42.9 | 14 | 0.6 |
| Morelia | 103 | 7.7 | 576 | 43.0 | 606 | 45.2 | 56 | 4.2 | 1341 | 53.1 |
| Uruapan | 0 | 0.0 | 148 | 37.9 | 34 | 8.7 | 209 | 53.5 | 391 | 15.5 |
| Zamora | 0 | 0.0 | 202 | 53.9 | 65 | 17.3 | 108 | 28.8 | 375 | 14.8 |
| Zitácuaro | 26 | 8.8 | 126 | 42.9 | 39 | 13.3 | 103 | 35.0 | 294 | 11.6 |
| Lázaro Cárdenas | 0 | 0.0 | 65 | 58.6 | 0 | 0.0 | 46 | 41.4 | 111 | 4.4 |
| TOTAL | 130 | 5.1 | 1120 | 44.3 | 748 | 29.6 | 528 | 20.9 | 2526 | 100.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDialysis and Renal Disease Management · Healthcare Systems and Reforms · Pharmaceutical Practices and Patient Outcomes
Introduction
Chronic kidney disease (CKD) is a condition that progressively impairs kidney function. The etiology of CKD includes intrinsic causes such as genetic factors, sex, and age, and extrinsic causes such as poor lifestyle, diet quality, chronic diseases including diabetes and hypertension, exposure to exogenous substances including medications, consumption of alcohol and tobacco, drugs of abuse, industrial food additives, and exposure to environmental agents including heavy metals, pesticides, and chemicals encountered during occupational exposure [1].
CKD can progress to end-stage renal disease (ESRD), leading to multiple complications for the patient, including the accumulation of toxins in the body, which causes damage to various organs and tissues, and impaired electrolyte and mineral excretion, which can increase blood pressure and lead to its associated complications. Renal damage can manifest directly through histological changes in renal biopsy or indirectly through albuminuria, abnormalities in urine sediment, or imaging techniques; however, serum creatinine or C cystatin are often the most common biomarkers detected in primary care [2]. Various international guidelines, including the 2024 Kidney Disease Improving Global Outcomes (KDIGO) guidelines, have confirmed the definition of CKD (regardless of clinical diagnosis) as the presence of an estimated glomerular filtration rate (eGFR) below 60 ml/minute/1.73 m² and/or kidney damage for at least three months [3].
Creatinine clearance is often used to calculate the glomerular filtration rate (GFR) to determine the progression of CKD. Five stages of CKD progression have been proposed based on GFR levels: Stage 1 with normal or high GFR (GFR > 90 mL/minute), Stage 2 mild CKD (GFR = 60-89 mL/minute), Stage 3A moderate CKD (GFR = 45-59 mL/minute), Stage 3B moderate CKD (GFR = 30-44 mL/minute), Stage 4 severe CKD (GFR = 15-29 mL/minute), and Stage 5 end-stage CKD (GFR < 15 mL/minute) [3]. The latter is characterized by the need for renal replacement therapy (RRT), either through peritoneal dialysis (PD), hemodialysis (HD), or kidney transplantation. The treatment of CKD patients is interdisciplinary, as it is essential to manage various aspects of the patient's care such as diet, physical activity, avoiding risk factors, and controlling chronic diseases if present.
In countries undergoing demographic and epidemiological transition, the aging population and the high prevalence of metabolic diseases such as type 2 diabetes (T2D) and arterial hypertension (AHT) also lead to a high prevalence of CKD, particularly in the adult population [4]. Moreover, CKD carries significant economic implications for the patient, healthcare services, and society, with the economic burden increasing as the disease progresses. Early CKD onset leads to lost years of productive life, years of life lost due to premature death, and more years lived with disability.
In addition to the genetic and metabolic diseases mentioned, the presence of behavioral risk factors such as an obesogenic lifestyle and substance abuse (alcohol, tobacco, or drugs), as well as exposure to environmental factors, can exacerbate the problem, leading to earlier onset of CKD and potentially faster progression in individuals with these risk factors. Therefore, it is necessary to monitor the incidence and prevalence of the disease nationally and regionally, as well as the potential behavioral and environmental risk factors involved.
In Mexico, demographic and epidemiological transitions have led to a high prevalence of non-communicable chronic diseases (NCDs). The international Global Burden of Disease (GBD) project has highlighted the CKD problem in Mexico. A growing epidemiological trend has been identified, and by 2019, Mexico ranked third in Latin America for mortality and disability-adjusted life years (DALYs) lost due to CKD [5]. Additionally, in 2020, a national prevalence of 9.29% was determined, including causes such as T2D (1.42%), type 1 diabetes (0.05%), hypertension (0.41%), glomerulonephritis (0.19%), and other unspecified causes (7.22%) [6]. It is worth noting that idiopathic CKD has been frequently classified in Mexico [7-10].
A recent publication estimated the average annual per capita cost of RRT for social security institutions in Mexico, including the Instituto Mexicano del Seguro Social (IMSS) and the Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado (ISSSTE), both of which serve the formal employed population in the private and public sectors. In the first year of treatment, the annual dialysis, hemodialysis, and kidney transplantation costs were 465,500, 783,800, and 799,400 Mexican pesos (23,900, 40,300, and 41,100 USD, considering an exchange rate of 1 Mexican peso = 0.05141 USD), respectively [11].
Several publications have explored the CKD problem in Mexico to varying degrees [12,13]. The GBD study has also allowed for a regional understanding of the problem by state, based on prevalence, incidence, or disease burden indicators such as years of life lost due to premature death (YLL), where it was determined that Veracruz, Tabasco, State of Mexico, Mexico City, Tlaxcala, and Puebla topped the list in 2021 [14]. Additionally, more specific analyses have been conducted for particular regions of the country where high incidence rates have been identified, potentially associated with various factors such as environmental, social, socio-economic, cultural, biological, or genetic factors, with a focus on idiopathic CKD and research on incidence and risk factors in children, adolescents, and young adults. Some of these regional studies have been conducted in Veracruz, Jalisco, Aguascalientes, and San Luis Potosí from different approaches [15-20]. Moreover, other regions of the country have been identified where high mortality rates among children and adolescents due to CKD have been reported, but more extensive analyses have not been published [21]. Recently, there has been growing interest in research in certain municipalities in the eastern region of Michoacán, mainly because a high incidence of CKD has been observed in young people without metabolic diseases; however, research on adults remains important. A recent study explored the prevalence of CKD among IMSS beneficiaries in the state of Michoacán; however, it only explored metabolic risk factors and did not examine differences in prevalence or incidence by geographic region [22].
This study aims to analyze the incidence, demographics, and service utilization among IMSS beneficiaries in Michoacán who are referred for RRT involving PD or HD. Specifically, the main research hypotheses are: (i) Incidence of patient referrals to RRT might be higher in certain IMSS Michoacán subdelegations of adscription or regions, (ii) Age at dialysis initiation might be lower in certain IMSS Michoacán subdelegations of adscription or regions, and (iii) Provision of dialysis services might be different in the IMSS Michoacán subdelegations of adscription.
Materials and methods
This was a study conducted at Universidad Michoacana de San Nicolás de Hidalgo (UMSNH), Morelia, Mexico, based on data from a database created by the IMSS Michoacán. The study was approved and agreed upon via a collaboration agreement between UMSNH and IMSS, signed in July 2024 (registration number: UMSNH/DVSS/63/2004).
According to the latest national census conducted in 2020, the population of the state of Michoacán was 4,748,846 [23]. The state of Michoacán is comprised of 113 municipalities. The IMSS is the social security system accessible to workers with formal employment. According to the 2020 national census, the IMSS covered 1,207,045 inhabitants in Michoacán, representing 25.42% of the population [23]. In Michoacán, IMSS services at the primary care level are provided through five subdelegations: Morelia, Uruapan, Zamora, Zitácuaro, and Lázaro Cárdenas, each with their respective primary care services named Unidades de Medicina Familiar (UMF) [24]. Additionally, at the second and third levels of healthcare, the IMSS in Michoacán has different kinds of service provision schemes: Regional General Hospital (HGR), General Zone Hospital (HGZ), General Subzone Hospital (HGS), General Zone Hospital with Family Medicine (HGZMF), General Subzone Hospital with Family Medicine (HGSMF), Ambulatory Care Medical Unit (UMAA), and UMF with Hospitalization (UMFH) [25].
A map was created to show the location of the IMSS subdelegations in Michoacán and the location of health services. The location of health services was obtained from the database "Catalog of Unique Health Establishment Codes-CLUES" for 2023 [26]. The open-source program QGIS ver. 3.34 was used [27]. Figure 1 shows the generated map.
Health services at IMSS Michoacán, Mexico. Municipalities: 1. Acuitzio, 2. Aguililla, 3. Álvaro Obregón, 4. Angamacutiro, 5. Angangueo, 6. Apatzingán, 7. Aporo, 8. Aquila, 9. Ario, 10. Arteaga, 11. Briseñas, 12. Buenavista, 13. Carácuaro, 14. Coahuayana, 15. Coalcomán de VázquezPallares, 16. Coeneo, 17. Contepec, 18. Copándaro, 19. Cotija, 20. Cuitzeo, 21. Charapan, 22. Charo, 23. Chavinda, 24. Cherán, 25. Chilchota, 26. Chinicuila, 27. Chucándiro, 28. Churintzio, 29. Churumuco, 30. Ecuandureo, 31. Epitacio Huerta, 32. Erongarícuaro, 33. Gabriel Zamora, 34. Hidalgo, 35. La Huacana, 36. Huandacareo, 37. Huaniqueo, 38. Huetamo, 39. Huiramba, 40. Indaparapeo, 41. Irimbo, 42. Ixtlan, 43. Jacona, 44. Jiménez, 45. Jiquilpan, 46. Juárez, 47. Jungapeo, 48. Lagunillas, 49. Madero, 50. Maravatío, 51. Marcos Castellanos, 52. Lázaro Cárdenas, 53. Morelia, 54. Morelos, 55. Múgica, 56. Nahuatzen, 57. Nocupétaro, 58. Nuevo Parangaricutiro, 59. Nuevo Urecho, 60. Numarán, 61. Ocampo, 62. Pajacuarán, 63. Panindícuaro, 64. Parácuaro, 65. Paracho, 66. Pátzcuaro, 67. Penjamillo, 68. Peribán, 69. La Piedad, 70. Purépero, 71. Puruándiro, 72. Querándaro, 73. Quiroga, 74. Cojumatlán de Regules, 75. LosReyes, 76. Sahuayo, 77. San Lucas, 78. Santa Ana Maya, 79. Salvador Escalante, 80. Senguio, 81. Susupuato, 82. Tacámbaro, 83. Tancítaro, 84. Tangamandapio, 85. Tangancácuaro, 86. Tanhuato, 87. Taretán, 88. Tarímbaro, 89. Tepalcatepec, 90. Tingambato, 91. Tinguindín, 92. Tiquicheo de Nicolás Romero, 93. Tlalpujahua, 94. Tlazazalca, 95. Tocumbo, 96. Tumbiscatío, 97. Turicato, 98. Tuxpan, 99. Tuzantla, 100. Tzintzuntzan, 101. Tzitzio, 102. Uruapan, 103. Venustiano Carranza, 104. Villamar, 105. Vista Hermosa, 106. Yurécuaro, 107. Zacapu, 108. Zamora, 109. Zináparo, 110. Zinapécuaro, 111. Ziracuaretiro, 112. Zitácuaro, 113. José Sixto VerduzcoIMSS: Instituto Mexicano del Seguro Social
Database of CKD patients
A database of IMSS beneficiaries in Michoacán who were referred to peritoneal dialysis and hemodialysis services was obtained. This database was generated by implementing an electronic patient registration system. The data to be analyzed was taken from January 2007 to September 2023.
Data analysis
The database was analyzed using IBM SPSS Statistics for Windows, Version 25.0 (Released 2017; IBM Corp., Armonk, New York, United States). All the patients registered in the database were included in the analysis because all were referred to RRT services, regardless of the diagnosis registered in the database (no inclusion/exclusion criteria for patients were used). Regarding the data cleaning process, duplicate registers of patients were eliminated using patients' personal identification numbers, so only the first register was used. No imputation techniques were employed, and the descriptive analysis of particular variables was performed only on the patients with information about that variable.
First, a trend analysis was conducted on the number of new cases recorded in the database over time. General trend graphs and descriptive tables were obtained. An analysis by sex, age group (<30 years and >30 years), and the patient's subdelegation of adscription, i.e., the administration to which the UMF where they receive care belongs (primary care level), was included. A cut-off of 30 years was proposed to establish two age groups, as it is considered unlikely that chronic non-communicable diseases (CNCDs) of metabolic origin (diabetes, hypertension) would be determined as the cause below this age.
The second analysis conducted was a description of the causes recorded in the database, for which pie charts were created for the total number of patients entered into the database, as well as for those under 30 years of age and over 30 years of age. The frequency of cases recorded with CNCDs of metabolic origin, such as type 1 diabetes (T1D), T2D, and arterial hypertension (AHT), as well as those recorded simply as "Chronic Kidney Disease," was analyzed. A table was also created to describe the causes recorded in the database.
The third analysis was a calculation of the incidence rates of patients referred to PD/HD services in 2021 since recent information about population and IMSS affiliations were available from the previous census conducted in 2020 [23]. These incidence rates were calculated by sex, age group, Subdelegation of adscription of the patients, and a region of interest composed of three municipalities in the state of Michoacán (Zinapécuaro, Maravatío, and Hidalgo).
The fourth analysis involved calculating the age at dialysis initiation as an indicator that may reflect the presence or exposure to different risks that may influence the development and progression of CKD to the need for RRT. Descriptive graphs such as histograms and boxplots were created, as well as descriptive tables including the analysis of the influence of sex and the geographical location of patients, which was obtained through the subdelegation of adscription to which the UMF they attended belonged. This analysis was performed for the total number of patients entered into the database. The tables reported the frequency of patients in two age categories (<30 years and >30 years). This analysis was also performed by the Care unit that attended to the patients. Additionally, an analysis was conducted to compare the age at dialysis initiation in municipalities in the eastern part of Michoacán with other municipalities in the state. Differences in means (DM) were calculated to compare these groups.
Finally, the absolute and relative frequency of patients who were in different types of service was obtained: automated peritoneal dialysis, continuous ambulatory peritoneal dialysis, in-house hemodialysis, and outsourced hemodialysis, analyzing by the Care unit attended by the patients and by the subdelegation of adscription to which the primary care clinic to which they are affiliated belonged.
Descriptive statistics was employed in all the analyses performed since data came from the total RRT-referred patients insured to the IMSS Michoacán in the study period. The approach of the study was to describe the data available.
Results
The database included 2,526 patients, of which 2,484 (98.3%) were still active in the IMSS healthcare services when downloaded (September 2023). This means they had not been removed for various reasons (such as changing institutions, migration, loss of eligibility, transplantation, or death). Of the patients included, 1,531 (60.6%) were men, and 995 (39.4%) were women. Information on the age at dialysis initiation was available for 2,471 patients, the overall mean age at dialysis initiation was 50.30 (±16.97 SD) years, 417 were under 30 years old (16.8%), and 2,064 (83.2%) were over 30 years of age. A more detailed analysis will be presented in a later section.
Trends in patient referrals
The trends in the registration of new patients referred for PD and HD are shown in Figure 2. The graphs show a growing trend in registered cases, suggesting an increase in prevalence and incidence each year. Figure 2a illustrates a higher incidence in men and shows a significant increase in cases registered in 2022. Figure 2b indicates a higher incidence of patients over 30 years of age. Figures 2c-2d break down the incidence of new cases by subdelegation of adscription, highlighting the subdelegations of Morelia and Zitácuaro for patients under 30 years of age and the subdelegations of Morelia and Uruapan for those over 30 years of age.
Evolution of patients referrals to RRT services (2007-2023) (a) by sex, (b) by age group, (c) by subdelegation of adscription for patients under 30 years of age, and (d) by subdelegation of adscription for patients over 30 years of ageRRT: renal replacement therapy
Table 1 describes the incidence of new cases by subdelegation of adscription. In some cases, the year they began operations can be observed due to recent service openings; for example, in the "HGZ 8 Uruapan," which started registering new patients in 2022.
Analysis of registered causes for patients in the database
Figure 3 shows the frequencies of registered causes of all the referred patients recorded in the database with complete data (n=2352) (Figure 3a), as well as for patients under 30 years of age (n=377, 16.0%) (Figure 3b) and over 30 years of age (n=1,975, 84.0%) (Figure 3c). The majority of causes registered in the database were only as “Chronic Renal Insuficiency" (CRI) or “Chronic Renal Insuficiency, not specified" (CRIns). It stands out that for patients aged under 30 years, there is a major frequency of registration as “CRI” or “CRIns” and hypoplasia, but a minor frequency of causes like “diabetes and hypertension” and “type 1 diabetes”, compared with patients over 30 years.
Pie chart of the causes of CKD recorded in the database for the referred patients (2007-2023). (a) Total sample (n=2352), (b) Subjects under 30 years of age (n=377), and (c) Subjects over 30 years of age (n=1975)CKD: chronic kidney disease
Analysis of the incidence of patients referred for PD/HD in 2021
Table 2 shows the incidence of new cases referred to PD/HD by sex, age group, subdelegation of adscription, and region for 2021. The overall rate for this year and the state of Michoacán was 28.42 cases per 100,000 insured persons. Men had a higher incidence rate than women (35.93 and 21.36 cases per 100,000 insured persons, respectively). The incidence rate by age group increased with age, peaking in the 60-69 age group, after which it began to decrease.
In the analysis of incidence by subdelegation of adscription, the Zitácuaro subdelegation stands out with the highest incidence (56.75 cases per 100,000 insured persons), followed by the Morelia subdelegation (29.10 cases per 100,000 insured persons), Uruapan subdelegation (29.18 cases per 100,000 insured persons), Lázaro Cárdenas subdelegation (21.90 cases per 100,000 insured persons), and Zamora subdelegation (20.57 cases per 100,000 insured persons). The special analysis for the region of interest, which includes the municipalities of Hidalgo, Zinapecuaro, and Maravatio, showed a rate of 160.50 cases per 100,000 insured persons, significantly higher than the rate for the rest of the municipalities in the state of Michoacán, which was 24.82 cases per 100,000 insured persons. Figure 4 shows a graphic representation of the main Incidence rate 2021 results.
Incidence rate of patient referrals to RRT services (2021) (x 100,000 insured population) (a) by age group, (b) by subdelegation of adscription, and (c) by regionRRT: renal replacement therapy
Analysis of the age at dialysis initiation
Figure 5 summarizes the trends in the age at dialysis initiation (mean) of the patients referred to PD/HD from 2014 to 2023. Table 3 shows the description of all the cases referred to PD/HD and registered in the database (2007-2023) by subdelegation of adscription and region of interest, detailing sex and age at dialysis initiation, as well as the cases of patients under 30 years of age. As mentioned before, information on the age at dialysis initiation was available for 2471 patients, of which 1494 were men (60.5%) and 977 were women (39.5%). The overall mean age at dialysis initiation was 50.30 (±16.97 SD) years. Regarding age groups, 417 were under 30 years of age (16.8%), and 2064 were over 30 years of age (83.2%).
Trends of age at dialysis initiation (mean) (2014-2023) (a) by subdelegation of adscription and (b) by region of interest
Figure 6 shows histograms and box plots describing the age at dialysis initiation for patients referred to PD/HD, considering sex, subdelegation of adscription, and region of the state. Age at dialysis initiation histograms showed bimodal patterns.
Distribution of age at dialysis initiation for the total number of patients registered (2007-2023) (n=2471) (a) by sex, (b) by subdelegation of adscription, (c) by region of interest
The age at dialysis initiation by demographic characteristics is graphically shown in Figure 6a. The histograms and box plots showed that the distribution is very similar between men and women. For men, the mean age was 49.61±17.22 years (n=1498), while for women, the mean age was 50.20±16.67 years (n=983), with a mean difference of 0.59 years. This result shows that men, in addition to having a higher incidence, start PD/HD treatment slightly earlier than women.
Regarding the age at dialysis initiation in different subdelegations of adscription, demographic characteristics are shown in Table 4 and graphically in Figure 6b. The mean age for the Morelia subdelegation was 51.28±16.86 years (n=1330), for the Uruapan subdelegation it was 51.89±16.26 years (n=386), for the Zamora subdelegation, the mean age was 51.41±16.30 years (n=364), for Zitácuaro subdelegation, it was 40.68±17.44 years (n=281), and for Lázaro Cárdenas subdelegation, it was 53.82±13.57 years (n=110). The results for the Zitácuaro subdelegation are particularly noteworthy, as patients from this subdelegation started treatment at a younger age compared to other subdelegations. With regard to the region of interest, the mean age at dialysis initiation was 39.50±16.82 (n=328), while for the rest of the municipalities, it was 51.95±16.38 (n=2143), with a mean difference of 12.45 years (Table 3).
Table 4 presents the breakdown of demographic characteristics of patients for each primary healthcare clinic (UMF) of each subdelegation of description. Table 5 presents a summary of demographic characteristics of patients by Care unit.
Provision of PD/HD services
In Table 6 and Figure 7, the evolution of dialysis services at the moment of referral is shown.
Evolution of the provision of dialysis services during the study period (2014-2023).
Table 7 presents the absolute and relative frequencies of service provision to patients included in the database at the time of their referral by the Care unit during the entire study period. Currently, there are 10 Care units available for PD and HD. The three units with the highest patient attendance are HGR 1 Charo (n=715, 28.3%), UMAA 75 Morelia (n=454, 18.0%), and HGZ 83 Morelia (n=384, 15.2%). Regarding the services provided within IMSS healthcare facilities, the most significant is continuous ambulatory peritoneal dialysis (n=1120, 44.3%), followed by internal hemodialysis (n=748, 29.6%) and automated peritoneal dialysis (n=130, 5.1%); the remaining HD services were outsourced (n=528, 20.9%). Analyzing the service provision in each Care unit, all of them provide continuous ambulatory peritoneal dialysis, but only six out of 10 units offer internal hemodialysis services (HGR 1, HGZ 4, HGZ 8, HGZ 83, HGZMF 2, and UMAA 75). Automated PD is only offered at UMAA 75, and outsourced hemodialysis has been implemented in four Care units (HGR 1, HGZ 4, HGZ 8, HGZMF 12).
Table 7 presents the service provision by subdelegation of adscription also. Analyzing this information, only patients from two subdelegations (Morelia and Zitacuaro) had access to automated PD. Another interesting fact is that patients from subdelegations of Uruapan, Zamora, Zitácuaro, and Lazaro Cárdenas had minor proportions of patients referred to internal HD, compared to the subdelegation of Morelia, so they use subcontracted services.
Figure 8 presents a graphical representation of the previously mentioned results.
Provision of dialysis services, (a) by Care unit and (b) by subdelegation of adscription (2014-2023)
Discussion
Trends in RRT referral incidence
The database analysis allowed us to identify significant trends in the incidence of new cases of patients referred to RRT services at IMSS Michoacán. Generally, a growing trend has been observed since 2014, possibly due to various factors, including environmental aspects and epidemiological transitions. It should be mentioned that improved patient registration following the implementation of the database could be an important factor too. It is worth mentioning that this upward trend is also related to the increasing epidemiological trend of CKD that has been reported for the country in previous studies, including the analyses from the GBD project [14].
Additionally, the trend graphs (Figure 2) showed a more significant increase in patient referrals to RRT during the COVID-19 pandemic, suggesting a possible association between this disease and CKD progression. Notably, this increased incidence was also observed nationwide in a study that analyzed CKD incidence trends up to 2021 [14]. As in this study, the literature has reported an association between COVID-19 and CKD progression, leading to increased demand for RRT [28-30]. It is worth noting that the subdelegation with the most significant increase in new admissions was the Morelia subdelegation, where the Regional General Hospital 1 "Charo" is located, which is the most important medical referral center in the state of Michoacán, having the most extensive infrastructure.
Incidence rate of RRT referrals
For 2021, the incidence rate of patient admissions to RRT was estimated at 28.42 per 100,000 IMSS beneficiaries in Michoacán. In the same year, the GBD study estimated a CKD incidence rate for Michoacán at 436.1 per 100,000 population [6]. Assuming the same rate for IMSS beneficiaries in 2022, it would be determined that around 6.5% of new CKD-diagnosed patients progressed to RRT that same year. The incidence rate of admission to RRT was higher in men than women, which also aligns with the CKD incidence rate identified in previous studies, including the GBD. Regarding age, a growing trend in the incidence rate was observed as age groups increased, which seems reasonable, as the likelihood of requiring RRT increases with age, although this trend appears to decline.
Regarding the calculation of the incidence of admission to RRT by age group in the same year (2021), the high incidence in those under 20 years stands out, where there is a lower probability of being related to non-communicable diseases such as T2D and hypertension. Grouping the results obtained for those under 20 years of age, eight new cases were recorded, corresponding to an RRT admission incidence rate of 4.11 per 100,000 population. In the same year and for this age group, the GBD reported a CKD incidence in Michoacán of 53.25 per 100,000 population (15th place nationally) and a mortality rate of 1.39 per 100,000 population (6th place nationally) [6].
Regarding the calculation of the incidence of admission to RRT by the patient's subdelegation of adscription, the highest rate was for the Zitácuaro subdelegation (56.75 per 100,000 population), nearly double the rate obtained for the Morelia subdelegation (29.10 per 100,000 population). Additionally, the analysis conducted for the Eastern Michoacán region, which included the municipalities of Hidalgo, Zinapécuaro, and Maravatío, showed an incidence rate 6.46 times higher compared to the rest of the municipalities in the state of Michoacán. It is worth mentioning that these municipalities were grouped because they surround an area of interest, and the subdelegation analysis separates these municipalities as they belong to different subdelegations (the municipalities of Hidalgo and Maravatío belong to the Zitácuaro subdelegation, while the municipality of Zinapécuaro belongs to the Morelia subdelegation).
CKD causes recorded in the database
Regarding the results found concerning the causes of CKD at the time of patients' admission to RRT services, it stands out a high frequency of registrations as “Chronic Renal Insufficiency” or “Chronic Renal Insufficiency, not specified”. This relies on the electronic medical record (EMR) implemented, where medical staff can only enter one diagnosis instead of specifying a primary diagnosis, secondary diagnosis, and associations with other diseases. So, this registration could reflect various different etiologies, including non-communicable diseases and unknown causes (CKD of unknown etiology). The registration of particular etiologies showed non-communicable diseases such as diabetes and hypertension in both, those under 30 years of age and in those over 30 years of age; however, as expected, this was more significant in the latter group.
Age at dialysis initiation
One of this study's most important contributions is the analysis of the patients' age at dialysis initiation. The trend analysis for this variable (Figure 5) showed differences between patients' subdelegation of adscription and an increasing trend for this variable; this trend could be attributed to the epidemiological transition, which implies the impact of NCDs on renal impairment for the population. The distribution of this variable clearly showed a bimodal pattern (Figure 6), meaning it can be approximately divided into two different groups, with 40 years appearing to be the cut-off point. This analysis revealed no sex-related differences, but more importantly, this study found a difference concerning the subdelegation from which the patients originated, identifying Zitacuaro as the subdelegation where patients begin RRT at a younger age.
Furthermore, a special analysis comparing the age at dialysis initiation in patients from Care units located in the municipalities of Hidalgo, Zinapecuaro, and Maravatio with those from units in other municipalities showed that patients from Hidalgo, Zinapecuaro, and Maravatio had a noticeably younger age at dialysis initiation, averaging 12.44 years younger (Figure 5 and Figure 6).
RRT service provision
Another analysis described the type of RRT provided to patients during the analysis period. Table 4 and Figure 7 show the evolution in service provision, highlighting the increasing trend in hemodialysis service provision, even peaking in 2022, possibly related to the COVID-19 pandemic. This trend of increased hemodialysis provision has been documented across different institutions within the health system and may be due to better access to the necessary biomedical equipment. However, there is still much to be done to improve access to this service [31].
The comparative analysis of service provision by Care unit (Table 5 and Figure 8a) highlighted the lack of services in some units, such as automated PD, which is only provided at UMF 75 - UMAA 254 in Morelia, and internal (intramural) HD, which is not provided in four Care units (HGS 7 La Piedad, HGSMF 17 Los Reyes, HGSMF 9 Apatzingán, and HGZMF 12 Lázaro Cárdenas). Additionally, there is a high frequency of service outsourcing in four Care units (HGR 1 Charo, HGZ 4 Zamora, HGZ 8 Uruapan, and HGZMF 12 Lázaro Cárdenas). Furthermore, 46.3% (n=1169) of patients were treated in Care units located in the state capital (HGR 1 Charo and UMF 75 - UMAA 254 Morelia), highlighting the lack of infrastructure in the Care units in other municipalities of the state.
Analyzing RRT service provision by subdelegation of adscription (Table 5 and Figure 8b), the high frequency of services provided to the population affiliated with the Morelia subdelegation (53.1%) stands out, with a low frequency of outsourced services (4.2%). However, for the population affiliated with other subdelegations, low frequencies of HD services and very high frequencies of outsourced services (28.8-53.5%) were observed. This indicates the low availability of infrastructure for Hd in other subdelegations, which may pose a more significant burden on patients, as they must travel from their place of origin to receive this service.
Strengths and limitations of the study
The strengths of this study include the proposal to use the indicator of age at dialysis initiation, as this indicator could globally reflect the population's exposure to various risk factors, both individual (biological and behavioral) and environmental, occupational, and socioeconomic, which can jointly influence CKD development. Additionally, the analysis of the geographical location of municipalities and subdelegations of the institution helped identify the IMSS health service delivery system.
The study's limitations include that it was based solely on a retrospective analysis based on the database provided by IMSS's RRT services, which limits it to the information available in this database, which the implemented EMR system may constrain. Also, a time series analysis could have been a better analysis to have a statistical model that could generate predictive information, but we consider this could be a future analytic approach.
Public health implications
This study has several implications. From an epidemiological perspective, further study is needed to explore the risk factors associated with CKD incidence and referral to RRT. While studies have explored metabolic risk factors [22], the impact of environmental, socioeconomic, and occupational factors remains underexplored. Notably, other studies in Mexico have found an association between agricultural work and CKD incidence [17], making this an important area of research in Michoacán. Exposure to metals and chemicals also presents a significant research opportunity. Additionally, there is a need to establish an observatory to analyze this issue on a regional level in Michoacán, particularly in the eastern region of the state, assessing CKD prevalence and incidence from various causes, including those with unknown etiology.
From a biomedical perspective, expanding research on the causes of CKD incidence in the area of interest is crucial. This may require obtaining percutaneous renal biopsies from native kidneys, as done in another state [15]. Furthermore, incorporating genomic studies of affected patients is essential to identify potential gene associations with CKD incidence.
From a health systems perspective, it is essential to strengthen the infrastructure for HD within the institution to minimize the need for outsourced services, which have been documented to incur higher costs [32]. A holistic approach to patient management in PD is necessary, emphasizing enhancing kidney transplantation, which remains the most cost-effective and quality-of-life-improving therapy in the long term. Moreover, the lack of infrastructure can impose additional burdens on patients, requiring them to travel from their place of origin, incur transportation costs, and spend time commuting, thereby increasing the burden on primary caregivers. Also, regarding the previously mentioned problem in the EMR, this presents an opportunity to improve this patient registration and tracking system.
Conclusions
The analysis conducted in this study identifies that there is an increasing trend in RRT referrals at the IMSS Michoacán that could be associated with the epidemiological transition phenomenon in Mexico. A more important issue in the incidence of RRT referrals and age at treatment initiation was identified for a particular subdelegation of adscription and region of interest in this institution. Moreover, the need to strengthen HD service infrastructure is identified to improve accessibility for insured patients living in various municipalities in Michoacán, Mexico. Future research should investigate environmental, behavioral, and occupational risk factors, especially in the region of interest, to understand the earlier onset of CKD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chronic kidney disease Nat Rev Dis Primers Romagnani P Remuzzi G Glassock R 17088320172916847510.1038/nrdp.2017.88 · doi ↗ · pubmed ↗
- 2Consensus document for the detection and management of chronic kidney disease Nefrologia Martínez-Castelao A Górriz JL Segura-de la Morena J 2432623420142465820110.3265/Nefrologia.pre 2014.Feb.12455 · doi ↗ · pubmed ↗
- 3KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease Kidney Int 03141052024 https://www.kidney-international.org/article/S 0085-2538%2823%2900766-4/fulltext 10.1016/j.kint.2023.10.01838490803 · doi ↗ · pubmed ↗
- 4Chronic kidney disease in the older adult patient with diabetes J Clin Med Ravender R Roumelioti ME Schmidt DW Unruh ML Argyropoulos C 3481320243825648210.3390/jcm 13020348 PMC 10816477 · doi ↗ · pubmed ↗
- 5Quantification of the burden of chronic kidney disease in Latin America: an invisible epidemic [Article in Spanish]Rev Panam Salud Publica Rosas-Valdez FU Aguirre-Vázquez AF Agudelo-Botero M 048202410.26633/RPSP.2024.41PMC 1101825838623527 · doi ↗ · pubmed ↗
- 6Institute for Health Metrics and Evaluation (IHME): GBD compare 7 2024 2020 https://vizhub.healthdata.org/gbd-compare/
- 7Mesoamerican endemic nephropathy (Me N): a disease reported in adults that may start since childhood?Semin Nephrol Lou-Meda R Alvarez-Elías AC Bonilla-Félix M 1513374220223702814710.1016/j.semnephrol.2023.151337 · doi ↗ · pubmed ↗
- 8Mesoamerican nephropathy (Me N): what we know so far Int J Nephrol Renovasc Dis Sanchez Polo V Garcia-Trabanino R Rodriguez G Madero M 2612721320203311675710.2147/IJNRD.S 270709 PMC 7588276 · doi ↗ · pubmed ↗