A tympanitis-related brain abscess caused by Helcococcus kunzii in China: a case report and literature review
Liyan Mao, Zhongju Chen, Chao Xu, Xueman Wang, Lu Gong, Sui Gao, Ziyong Sun, Cui Jian

TL;DR
This paper reports the first case of a brain abscess caused by Helcococcus kunzii in China, emphasizing the importance of accurate diagnosis and treatment of such rare infections.
Contribution
The study presents the first documented case of a brain abscess caused by H. kunzii in China and highlights its clinical significance.
Findings
A 54-year-old patient with tympanitis developed a brain abscess caused by H. kunzii.
The H. kunzii strain was resistant to erythromycin and clindamycin but successfully treated with ceftriaxone, meropenem, and norvancomycin.
MALDI-TOF MS and 16S rRNA sequencing confirmed the presence of H. kunzii and two anaerobic bacteria.
Abstract
Infections attributed to Helcococcus kunzii are rarely documented, especially in relation to brain abscesses. This study aims to report the first documented case of a brain abscess associated with tympanitis caused by H. kunzii in China, alongside a comprehensive review of the existing literature. We detail the case of a 54-year-old female patient with a history of hypertension, who was diagnosed with tympanitis complicated by a brain abscess. An urgent occipital lobectomy was performed, during which pus was collected for culture analysis. Three distinct colony morphologies were identified through matrix-assisted laser desorption/ionization time of flight mass spectrometry (MALDI-TOF MS) analysis, including H. kunzii and two additional anaerobic bacterial species. Subsequent biochemical assays and 16S rRNA gene sequencing corroborated the presence of H. kunzii. Antimicrobial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
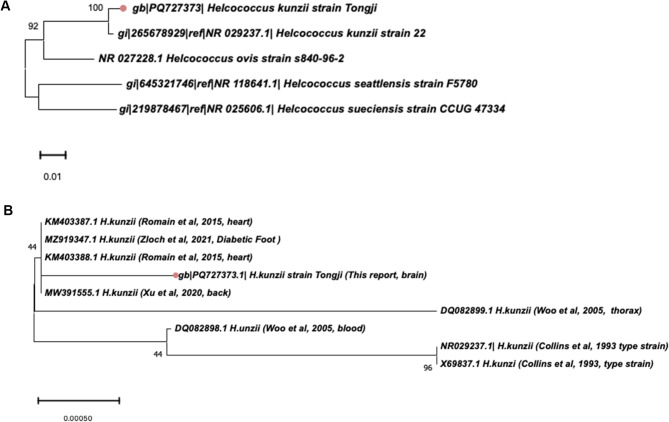 Figure 1
Figure 1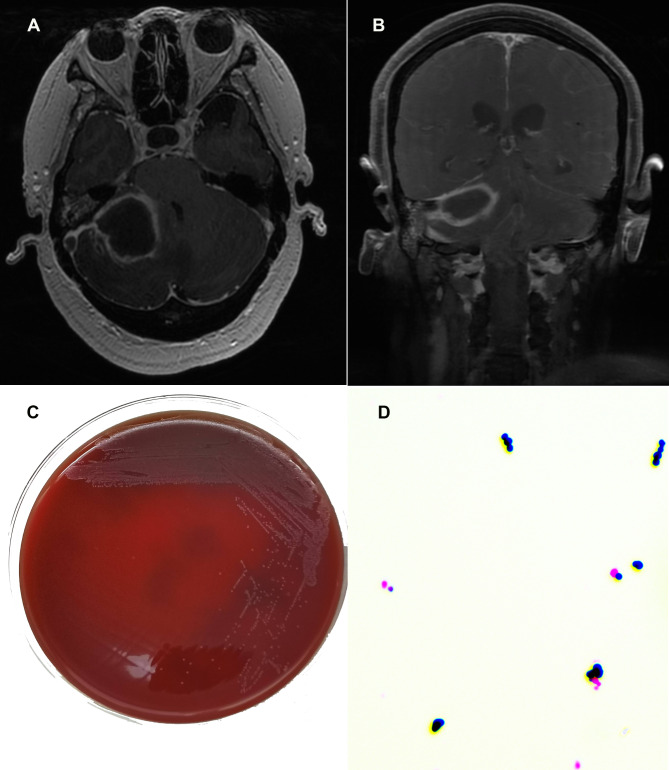 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Infections and Vaccines · Infective Endocarditis Diagnosis and Management · Actinomycetales infections and treatment
Background
Helcococcus, a Gram-positive cocci, was initially characterized in 1993 by Collins and colleagues [1]. This microorganism is a facultative anaerobe and catalase-negative. To date, six species within this genus have been identified, namely Helcococcus kunzii [1], Helcococcus ovis [2], Helcococcus pyogenica [3], Helcococcus sueciensis [4], Helcococcus seattlensis [5] and Helcococcus massiliensis [6]. These species have been isolated from a variety of animal and human specimens, suggesting a potential for zoonotic transmission as well as human infections [7–10]. Notably, H. kunzii is the most frequently identified pathogenic species [11]. H. kunzii is predominantly regarded as a commensal organism on the skin and is generally considered innocuous [12]. However, in immunocompromised individuals, it can act as an opportunistic pathogen [13, 14]. H. kunzii has been implicated in a variety of infections, including infective endocarditis, osteomyelitis, bacteremia, and abscesses at various anatomical sites [15–21].
In this report, we present the first documented case of a tympanitis-related brain abscess caused by H. kunzii in China, and we provide a comprehensive review of the existing literature on infections associated with H. kunzii.
Case presentation
In November 2023, a 54-year-old female patient presented with a ten-day history of dizziness, headache, and vomiting. She sought medical attention at our Neurology Department due to the persistence of her symptoms despite rest at home. A computed tomography (CT) scan of the head, performed at a local hospital, identified an intracranial space-occupying lesion. The patient’s medical history includes hypertension, which she managed with self-administered medication of limited efficacy. She reported no history of smoking, alcohol consumption, or other underlying diseases. A timeline shown in Supplemental Fig. 1 in Additional file 1.
Upon admission, the patient exhibited a body temperature of 36.8℃, accompanied by normal pulse and respiratory rates. The recorded blood pressure was 199/104 mmHg. The patient demonstrated an altered mental status, while no abnormalities were observed in the skin or lymph nodes. Pupillary examination revealed equal, round, and reactive pupils with a diameter of 2.5 mm, and visual fields were intact. The neck was supple, and no abnormalities were identified during the cardiac, pulmonary, and abdominal examinations. The patient demonstrated normal limb function and muscle strength, exhibiting physiological rather than pathological reflexes. Laboratory investigations indicated elevated inflammatory markers, including leukocytes (10.55 × 10^9/L), neutrophils (6.94 × 10^9/L), and monocytes (0.8 × 10^9/L). The dynamic changes in these indicators during hospitalization are depicted in Supplemental Fig. 2.
Upon admission, a head magnetic resonance imaging (MRI) scan conducted on November 21, 2023, revealed circumferential enhancement in the right cerebellopontine angle region, suggestive of an infectious lesion, with possibility of abscess formation. The imaging revealed increased enhancement of the falx cerebri and tentorium, along with a filling defect within the right sigmoid sinus, suggesting the possibility of venous thrombosis. Additionally, there were indications of infection in the right middle ear and mastoid, as illustrated in Fig. 1. Clinically, the patient presented with persistent confusion and ongoing episodes of vomiting. A subsequent MRI of the head, conducted on November 23, 2023, demonstrated no significant abnormalities in the bilateral vestibulocochlear nerves. However, a mixed-signal mass was detected in the right cerebellar hemisphere, with enhancement characteristics indicative of a potential abscess with associated hemorrhage. Right-sided tympanitis was reconfirmed, and imaging of the right sigmoid sinus revealed abnormal signals indicative of venous sinus thrombosis, accompanied by supratentorial hydrocephalus. A chest X-ray and echocardiogram showed no significant cardiopulmonary abnormalities. Integrating the clinical presentation, laboratory findings, and imaging results, in conjunction with a neurosurgical consultation, suggested a high likelihood of a brain abscess associated with right-sided middle ear tympanitis and concurrent venous sinus thrombosis. Surgical intervention for abscess drainage was recommended. Empirical antibiotic therapy was initiated with intravenous ceftriaxone at a dosage of 3 g per day.
Fig. 1 Imaging and microbiologic characteristics of the patient. (A). and (B). Head magnetic resonance imaging scan. (C). 1 Culture colonies of Helcococcus kunzii on sheep blood agar plates for 48 h. (D). Gram staining (× 1000 times) of H.kunzii
On the fourth day post-admission, the patient underwent an occipital lobectomy. During the procedure, the dura mater was incised under microscopic visualization, and a cortical puncture approximately 1 cm in depth was made, revealing the abscess capsule. Pus was aspirated for culture, and tissue samples from the walls of the intracranial abscess were collected for pathological examination. Intraoperative observations raised concerns regarding a potential anaerobic infection. Considering the necessity for comprehensive antimicrobial coverage targeting both Gram-positive cocci and β-lactamase-resistant anaerobes, along with meropenem’s enhanced ability to penetrate the blood-brain barrier, empirical treatment was commenced using intravenous meropenem (1 g every 8 h) for a duration of three days pending the availability of culture results. This therapeutic decision was further substantiated by a postoperative elevation in inflammatory markers: the white blood cell count increased from 10.55 × 10⁹/L preoperatively to 16.10 × 10⁹/L, and the neutrophil percentage rose from 65.7 to 91.2% (refer to Supplemental Fig. 2). Microbiological analysis of the pus aspirated intraoperatively, along with the abscess wall tissue, revealed a polymicrobial infection with H. kunzii as the predominant isolate. Histopathological analysis indicated necrotic regions within the cerebral tissue, along with the development of microabscesses. The adjacent inflammatory granulation tissue demonstrated significant infiltration by both acute and chronic inflammatory cells, as well as an accumulation of tissue cells. Additionally, mild reactive hyperplasia of certain glial cells was noted. In light of these findings, the antibiotic regimen was modified to include intravenous administration of norvancomycin at a dosage of 0.8 g, administered twice daily. A follow-up CT scan conducted seven days postoperatively revealed postoperative alterations in the abscess, including the absorption of hemorrhage and gas. The patient was discharged in a stable condition two weeks following admission. At the one-month follow-up, no significant abnormal symptoms were observed.
Postoperatively, a purulent specimen extracted from the brain abscess was submitted to the microbiology laboratory. The specimen was inoculated onto 5% sheep blood Columbia agar plates and chocolate agar to facilitate both aerobic and anaerobic bacterial cultures. After incubation at 35 °C for 24 h under aerobic conditions and 48 h under anaerobic conditions, three distinct colony morphologies were observed. Identification was conducted using matrix-assisted laser desorption/ionization time of flight mass spectrometry (MALDI-TOF MS, Autof ms1000, Autobio, China), which identified the colonies as H. kunzii,* Peptoniphilus harei*,* and Peptostreptococcus lactolyticus.* On sheep blood agar, H. kunzii exhibited superior growth (4 + colony density), significantly surpassing the sparse growth of P. harei and P. lactolyticus (1 + colony density). Notably, the colonies of H. kunzii, the predominant isolate, were characterized by pinpoint size after 24 h of incubation. After 48 h, they developed into small, colorless, transparent colonies with slight alpha-hemolytic activity (Fig. 1). Gram staining indicated that H. kunzii is a Gram-positive coccus, typically occurring singly, in pairs, or in short chains, with no spores, capsules, or flagella. The catalase and oxidase assays for this strain yielded negative results. Phenotypic identification via the Vitek2 compact system (BioMérieux, France) corroborated the presence of H. kunzii. Comprehensive biochemical data are presented in Supplementary Table 1. Furthermore, 16S rRNA gene sequencing was conducted on the pathogen via Applied Biosystems 3730xl DNA Analyzer (Thermo Fisher Scientific, USA). Subsequent BLAST analysis indicated that the partial sequence (comprising 1465 nucleotides, GenBank accession number PQ727373) demonstrated 98% homology, with 31 nucleotide discrepancies, compared to the H. kunzii sequence (NR029237) initially characterized in 1993 [1].
Antimicrobial susceptibility testing (AST) of H. kunzii was performed to evaluate its response to penicillin and ceftriaxone using the E-test assay on blood Mueller-Hinton agar. The susceptibilities to additional antimicrobial agents were assessed via disk diffusion assays, as detailed in Supplementary Table 2. In the absence of specific antimicrobial testing guidelines from the Clinical and Laboratory Standards Institute (CLSI) for Helcococcus, interpretations were made in accordance with the CLSI M100-ED34 (2024) guidelines established for Streptococcus species [22]. According to the CLSI guidelines [22], the strain under investigation exhibited susceptibility to penicillin, vancomycin, cefotaxime, ceftriaxone, linezolid, levofloxacin, and chloramphenicol. Conversely, it demonstrated resistance to erythromycin and clindamycin.
Discussion
H. kunzii was originally isolated from human clinical samples in 1993 [1]. This facultatively anaerobic, catalase-negative Gram-positive coccus demonstrates unique phylogenetic placement within the Helcococcus genus, as evidenced by 16 S rRNA divergence from Aerococcus species. The taxon honors Lawrence J. Kunz for his foundational work in Gram-positive bacterial systematics. Morphologically, H. kunzii grows as paired or clustered cocci, forming translucent-gray colonies (0.5–1 mm diameter) on sheep blood agar within 48 h [13]. Unlike many fastidious anaerobes, it grows equally well under atmospheric (18–22% O₂), microaerophilic (5% CO₂), and anaerobic conditions, producing non-hemolytic or α-hemolytic colonies across these environments [18, 23].
Published case reports of H. kunzii infections (summarized in Table 1) show a predilection for elderly males with comorbidities [5, 12, 15–18, 20, 24–28]. Over one-third of cases describe polymicrobial infections involving staphylococci, enterococci, Enterobacterales, or anaerobic bacteria [5, 12, 15, 17, 19, 26, 28]. While initially characterized as a skin commensal of the lower extremities, emerging evidence redefines it as an opportunistic pathogen, particularly in immunocompromised hosts [19]. The clinical spectrum of H. kunzii infections spans both localized and systemic manifestations. Notably, diabetic foot ulcers represent a key clinical manifestation [27], where impaired cutaneous integrity and microangiopathy likely facilitate microbial invasion. However, cases in non-diabetic patients with intact immune function demonstrate its pathogenic versatility beyond diabetic populations, including prosthetic joint infections [16] and soft tissue abscesses [29]. Of particular concern is the organism’s invasive potential, with severe manifestations such as infective endocarditis requiring combined antimicrobial and surgical management [12]. Notably, recent reports document neuroinvasive cases in immunocompetent individuals [28], solidifying its classification as a bona fide pathogen rather than an immunocompromise-dependent opportunist.
Table 1. Main features of reported cases of Helcococcus kunzii infectionsAuthorSex/age of patient (years)Underlying condition(s)Type of infectionTreatmentOutcomeOther bacteriaMethods of identificationPeel et al., 1997M, 36Hypertension, obesity, hypercholesteremiaInfected sebaceous cystFlucloxacillin IV and orally for 5 daysRecoveryNoneAPI 20 Strep systemChagla et al., 1998F, 57NoneBreast abscessCephalexin 0.5 g orally every 8 hRecoveryNoneAPI 20 S Strep system, 16 S rDNA gene sequencingRiegel et al., 2003F, 36NonePost-surgical foot abscessPristinamycin and rifampicinRecoveryNoneRapid ID 32 Strep system, 16 S rDNA gene sequencingWoo et al., 2005M, 41/M, 55Intravenous-drug use / Intravenous-drug use, alcoholismBacteremia / Empyema thoracis3 weeks of penicillin G and cloxacillin IV/8 weeks of amoxicillin-clavulanateRecovery/RecoveryNone/NoneAPI 20 Strep system, 16 S rDNA gene sequencingLemaître et al., 2008M, 79Hypertension, intermittent claudicationPlantar phlegmonCurative debridement and drainage of phlegmonN.A.Klebsiella oxytoca,* Bacteroides fragilisVITEK 2 GP card identification system, 16 S rDNA gene sequencingMcNicholas et al., 2011M, 75N.A.Infection of implantable cardiac deviceFlucloxacillin and benzylpenicillin IV (3 days) then vancomycin and clindamycin IV (14days) and oral amoxicillin and rifampicin (4 weeks)RecoveryNoneBBL CrystalTM System, BD Phoenix TM Automated Microbiology System, 16 S rDNA gene sequencingPérez-Jorge et al., 2011M, 39OsteochondritisProsthetic joint chronic infectionClindamycin and gentamicin initially, then clindamycin and rifampin for 3 monthsRecoveryNoneAPI 20 Strep system, 16 S rDNA gene sequencingChow et al., 2013M, 25/M, 68PTSD, CAD, colonic polypsToe abscess/Inner thigh wound from traumaSXT, cephalexin/Vancomycin and piperacillintazobactam inpatient; cephalexin outpatientN.A. Staphylococcus aureus/Staphylococcus aureus API 20 Strep system and VITEK 2, 16 S rDNA gene sequencingStanger et al. 2013M, 86Malignant melanoma, congenital thrombocytopeniaOsteomyelitisCefuroxime and metronidazole, radical debridement, then amoxicillin/clavulanic acid for 6 weeksRecoveryNormal skin flora, anaerobic bacteriaN.A.Park et al., 2014M, 58Diabetes and end-stage renal diseaseUlcerative lesion of footPiperacillin/tazobactam IV for 3 weeksRecovery Proteus mirabilis Matrix-assisted laser desorption time-of-flight mass spectrometry, Vitek2 GP system, 16 S rDNA gene sequencingSridhar et al., 2014M, 83Hypertension, diabetes, prostate cancerBrain abscessCeftriaxone and metronidazole IV (2 weeks), then oral amoxicillin-clavulanate, then ceftriaxone and metronidazole and vancomycin IV (total 12 weeks)RecoveryNoneVitek2 system, MALDI-TOF MS, 16 S rDNA gene sequencingLotte et al., 2015M, 79Heavy smoker, alcoholism, dyslipidemia, hypertension and polyvascular diseaseInfective endocarditisAmoxicillin and gentamicin, then Amoxicillin (4 weeks), mitral valve replacementRecoveryKlebsiella oxytoca*,* Bacteroides fragilisAPI 20 Strep system, MALDI-TOF MS, 16 S rDNA gene sequencingVergne et al., 2015M(82%), 61(21–91)Trophic disorders of the lower limbs (77%), cardiovascular pathology (67%), and diabetes mellitus (51%)Foot ulcers (79%), bacteremia (3%) and other ulcers (18%)Amoxicillinclavulanate (28%), fluoroquinolones (24%), and third-generation cephalosporins (21%)NAStaphylococcus aureus (62%), Enterobacteria (44%) and Anaerobes (31%)MALDI-TOF MS,16 S rDNA gene sequencingFarid et al., 2017M, 88Hypertension, hyperlipidemia, CAD, diastolic HF, paroxysmal AF, COPD, bilateral knee replacements, CKD, and OSA.Bacteremia, prosthetic valve endocarditis secondary to lower extremity cellulitis4 weeks of intravenous ceftriaxone. Cardiothoracic surgery and 4-week course of intravenous ceftriaxone at readmission.RecoveryNoneMALDI-TOF MS, leucine amino peptidase and pyrrolidonyl arylamidase testLi et al., 2021M, 66Coronary heart disease, heart failure, hypertension, and type 2 diabetes mellitusDiabetic footClindamycin and debridement, cefotiam and metronidazole after operation. VSD proceduresRecoveryNoneMALDI-TOF-MS, 16 S rRNA gene sequencingMouro et al., 2021M, 17CholesteatomaMastoiditis complicated by intracranial empyemaOral cefuroxime and topical ofloxacin. Ceftazidime 2 g tid, metronidazole 1 g bid, and vancomycin 1 g bid (4 weeks). Debridement and IV ciprofloxacin (with metronidazole). Oral ciprofloxacin and metronidazole.RecoveryPorphyromonas assacharolitica*,* Bacteroides ovatus*,* B. fragilis*Mass spectrometry (Vitek MS, bioMérieux, with Vitek MS comprehensive CE- marked database)Note: N.A. means Not Available, not mentioned in original article. Abbreviation: CAD, coronary artery disease. PTSD, post-traumatic stress disorder. HF, heart failure. AF, atrial fibrillation. COPD, chronic obstructive pulmonary disease. CKD, chronic kidney disease. OSA, obstructive sleep apneoa. VSD, vacuum sealing drainage. Tid, three times per day. Bid, twice per day. IV, intravenous
This report details China’s first documented case of a brain abscess linked to tympanitis caused by H. kunzii, marking the fourth known intracranial infection by this bacterium. Previous reports demonstrate variable clinical trajectories. Sridhar et al. (2014) achieved cure through 12-week antibiotic monotherapy for a solitary frontal lobe abscess [18]. A 2020 conference report by Ishak et al. described transient radiological improvement with ceftriaxone followed by fatal deterioration within 4 days [21]. The most recent case (2023) involved mastoiditis-associated polymicrobial abscess requiring combined surgical and antimicrobial intervention [28]. It is noteworthy that the case presented in this study also involved polymicrobial anaerobic co-infection and otogenic origin. However, this case uniquely demonstrates tympanic cavity involvement preceding intracranial spread, expanding the recognized pathophysiology of H. kunzii neuro-invasion. The inference of H. kunzii as the primary pathogen based on semi-quantitative culture predominance requires cautious interpretation in this polymicrobial context. Potential synergistic interactions between H. kunzii and co-infecting anaerobes remain speculative and warrant validation through future metagenomic and co-culture studies.
Accurate identification of H. kunzii remains challenging due to biochemical profiling inconsistencies across studies. While conventional API system (API20 STREP, bioMérieux, France) exhibit documented misidentification rates frequently confusing H. kunzii with Aerococcus spp. [1, 8, 26], our VITEK 2 compact system analysis achieved reliable species-level discrimination (94% confidence). As described in Supplementary Table 1,** H**. kunzii consistently tested positive for pyrrolidonyl arylamidase and negative for leucine aminopeptidase. Nevertheless, discrepancies were observed in the biochemical phenotyping, specifically regarding β-galactosidase, maltose, lactose, and ribose outcomes, when comparing our isolate to previously documented strains [5, 9, 15–17, 20, 24, 25, 29]. The MALDI-TOF MS successfully identified our strain at the species level. To corroborate the identification, we performed 16 S rRNA sequencing and submitted the sequence to GenBank under the accession number PQ727373. Our 16 S sequence showed 31-bp divergence from the Collins et al. type strain (NR029237) [1]. Phylogenetic reconstruction using MEGA11 (1400-bp alignment; the original sequence data can be found in Additional File 2) confirmed close clustering with H. kunzii (Fig. 2A**)**, while demonstrating distinct differences from other species within the Helcococcus genus. Although minor variations are observed at the species level in comparison to other strains in GenBank, the phylogenetic analysis of H. kunzii does not indicate significant clustering based on the infection site (refer to Fig. 2B). The present paucity of gene sequences within the database necessitates the continued accumulation of data to draw definitive conclusions.
Fig. 2 Phylogenetic tree of Helcococcus kunzi (A) Phylogenetic tree of Helcococcus kunzi and other Helcococcus genus. Other compared Helcococcus genus included Helcococcus ovis, Helcococcus sueciensis and Helcococcus seattlensis, and only type strains were focused. There was no 16 S rRNA gene sequence of Helcococcus massiliensis by Sanger sequencing submitted on GenBank. The length of 16 S rRNA gene sequence of Helcococcus pyogenica on the GenBank is only nearly 500 bp, which is not used for comparison. The lengths of all sequences included in the Phylogenetic tree are almost 1400 bp. (B) Phylogenetic tree of H.kunzi in this report and the H.kunzi isolates published by other literature
Supplementary Table 2 summarizes published AST profiles for H. kunzii. The pathogen generally demonstrates consistent susceptibility to β-lactams (penicillin, amoxicillin, cephalosporins), quinolones, and glycopeptides [18, 24], supporting Infectious Diseases Society of America's recommendations prioritizing β-lactams as first-line therapy for intracranial infections [30]. This pharmacological profile explains the radiographic resolution observed after ceftriaxone dose escalation in our case, where initial treatment failure likely resulted from suboptimal blood-brain barrier penetration rather than microbial resistance. However, emerging resistance patterns warrant vigilance. Reduced susceptibility to aminoglycosides, sulfonamides, nitroimidazoles, macrolides, and lincosamides has been documented in specific strains [16, 17, 25, 28, 29]. Our isolate’s resistance to erythromycin and clindamycin aligns with reports of ermA-mediated macrolide resistance in Helcococcus spp [25]., necessitating avoidance of these agents in empirical regimens. Notably, while Mouro et al. [28] observed penicillin resistance in one strain, our findings and most literature confirm preserved β-lactam susceptibility, suggesting resistance mechanisms may be strain-specific or geographically restricted. This geographical variability necessitates region-specific empirical approaches: in settings reporting β-lactam resistance, initial combination therapy with glycopeptides (e.g., norvancomycin) and carbapenems provides dual coverage against both H. kunzii and β-lactamase-producing anaerobes, as implemented in our case. Subsequent de-escalation to β-lactam monotherapy should be guided by confirmed susceptibility, particularly in polymicrobial infections where most of cases require concurrent anaerobic coverage. The therapeutic efficacy of norvancomycin in our patient despite in vitro β-lactam susceptibility underscores the complexity of polymicrobial infection management. This approach provided dual coverage against β-lactamase-producing anaerobes while maintaining antimicrobial activity for H. kunzii, illustrating the critical role of AST-guided combinatorial therapy in mixed infections. These observations collectively reinforce the imperative for continuous resistance surveillance and pharmacokinetic optimization in treating H. kunzii infections.
In conclusion, this study reports the first documented case of a brain abscess secondary to tympanitis caused by H. kunzii in China. Together with accumulating evidence of its neuroinvasive potential, these findings position H. kunzii as an emerging etiological agent requiring clinical vigilance. For accurate identification amidst its heterogeneous biochemical characteristics, MALDI-TOF MS and 16 S rRNA sequencing should be prioritized in diagnostic workflows.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Farid S, Miranda W, Maleszewski J, Sohail MR. Helcococcus kunzii prosthetic valve endocarditis secondary to lower extremity cellulitis. BMJ Case Rep 2017, 2017.10.1136/bcr-2017-219330 PMC 574764328473362 · doi ↗ · pubmed ↗
- 2Ishak NAHR, Abdul Wahab Z. A case of fatal brain abscess due to Helcococcus kunzil. In: Proceedings of the 19th international Congress on infectious diseases (ICID). Malaysia; 2020.
- 3CLSI. Performance Standards for Antimicrobial Susceptibility Testing. 34th ed. CLSI supplement M 100. Clinical and Laboratory Standards Institute 2024.
- 4Durand BARN, Yahiaoui Martinez A, Baud D, François P, Lavigne J-P, Dunyach-Remy C. Comparative genomics analysis of two Helcococcus kunzii strains co-isolated with Staphylococcus aureus from diabetic foot ulcers. Genomics 2022, 114(3).10.1016/j.ygeno.2022.11036535413435 · doi ↗ · pubmed ↗
- 5Mouro M, Frade J, Chaves C, Velez J. Helcococcus Kunzii, a skin-colonising microorganism with pathogenic capacity: a case of polymicrobial intracranial empyema. BMJ Case Rep 2021, 14(11).10.1136/bcr-2021-244600 PMC 857894534753723 · doi ↗ · pubmed ↗