Cardiac Catheterization and Interventions in Pediatric Patients on ECMO: Analysis of the IMPACT Registry
Kelsey D. McLean, Gerard R. Martin, Joshua P. Kanter, Kevin F. Kennedy, Shriprasad R. Deshpande

TL;DR
This study analyzes the safety and outcomes of cardiac catheterization in pediatric patients on ECMO, finding key risk factors and adverse events.
Contribution
The first large, multicenter analysis of cardiac catheterization safety in pediatric ECMO patients, identifying risk factors and adverse events.
Findings
Survival to hospital discharge was 53.2% overall, with lower rates in single ventricle patients.
Interventional procedures occurred in 52.5% of cases, and major adverse events occurred in 11.5%.
Single ventricle physiology was significantly associated with major adverse events.
Abstract
There are limited published studies on the performance and safety of cardiac catheterization in pediatric patients on extracorporeal membrane oxygenation (ECMO). We sought to understand the utilization and procedural safety of cardiac catheterization in pediatric patients on ECMO. We also aimed to understand differences in the types of interventions and outcomes in patients with single ventricle (SV) physiology compared to those with biventricular physiology. Characteristics and outcomes for patients undergoing cardiac catheterization while on ECMO were collected from the American College of Cardiology National Cardiovascular Data Registry: IMPACT (Improving Pediatric and Adult Congenital Treatment) Registry from 2011-2022. There were 3473 cardiac catheterizations performed on 2980 pediatric patients during the study period. Patients with SV comprised 31.6% of the population. Survival…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
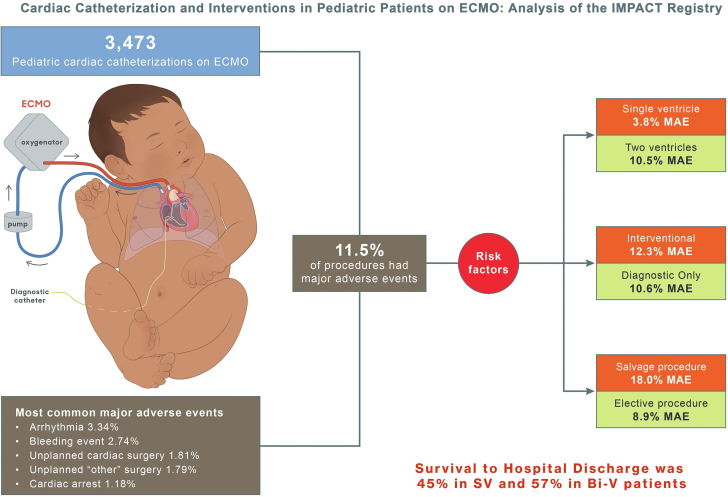 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Congenital Heart Disease Studies · Cardiac Arrhythmias and Treatments
Introduction
The use of extracorporeal membrane oxygenation (ECMO) to provide temporary cardiopulmonary support has continued to increase. It is a therapy that is associated with a high burden of morbidity and mortality.1^,^2 In pediatric patients, ECMO is commonly utilized in postoperative cardiac surgical patients with low cardiac output syndrome or failure to separate from bypass, in patients with refractory cardiopulmonary resuscitation attempts, and in patients presenting with decompensated heart failure from acute myocarditis.1 Outcomes of such ECMO support vary significantly by underlying indications for use. Specifically, congenital heart disease patients supported by ECMO have a higher rate of hospital mortality as seen with registry analysis of the Extracorporeal Life Support Organization.3 Such analysis and other studies have identified chromosomal anomalies, single ventricle (SV) physiology, multiple ECMO runs, higher 24-hour ECMO flows, decreased lung compliance, need for plasma exchange, infectious indications, and cardiac indications as risk factors for ECMO mortality.1, 2, 3 Additionally, the presence of residual lesions in those needing ECMO after cardiac surgery has been identified as a potential reason for ECMO nonsurvival. Addressing these residual lesions is important. The use of diagnostic cardiac catheterization in congenital heart disease patients on ECMO can be valuable to assess residual lesions, and hemodynamically significant anatomic issues, and potentially address them. Early catheterization has the potential to reduce time on ECMO as well as potential ECMO survival.4, 5, 6 Although there are single-center and small-scale reports of performance, utility, and safety of cardiac catheterization on pediatric patients supported on ECMO, there are no large multicenter studies addressing this important issue.
The aim of this study was therefore to understand the utilization of cardiac catheterization, interventions performed, and safety of these procedures in pediatric patients supported on ECMO from a multicenter, national database. We also aim to understand differences in the types of interventions and outcomes in patients with SV physiology compared to those with biventricular (BV) physiology.
Methods
The data for the study were obtained from the National Cardiovascular Data Registry (NCDR) sponsored IMPACT registry (IMproving Pediatric and Adult Congenital Treatments). The details about the registry formation, design, data collection, center participation, and data verification have been described previously.7^,^8 The centers report patient and procedural data to the registry using standardized data collection forms. The data elements include demographics, diagnostic details, procedural details, findings and complications, and outcomes for the episode of care. The data reporting tools as well as participating centers are available on the NCDR website: https://cvquality.acc.org/NCDR-Home/registries/hospital-registries/impact-registry and https://www.ncdr.com/WebNCDR/impact/home/datacollection. NCDR National Audit Program validates the accuracy of the submitted data on a yearly basis.8 To ensure the reliability and validity of an audit, eligible hospitals are given an opportunity to refute the findings, and an interrater reliability assessment of the auditors is built into the program.8 All of the definitions used in the study are consistent with the IMPACT registry definitions, including those for cardiac anatomy, primary and nonprimary IMPACT procedures, complications, and outcomes.8 The American College of Cardiology has designated Chesapeake Research Review Incorporated as its institutional review board (IRB) of record. Each registry has submitted a protocol to the IRB, which governs all human subject research conducted by that registry. All registry protocols on file have currently been granted a waiver of informed consent.
Study population
Data from 101 independent sites reporting to the registry were used for this study. Patients aged 0 days to 18 years who were supported with ECMO at the start of their cardiac catheterization were included and data were analyzed. The registry does not delineate the use of veno-venous ECMO vs veno-arterial ECMO and all comers were included.
Study outcome
The primary outcome of interest was the occurrence of a major adverse event (MAE) whereas the secondary outcome of interest was hospital survival. Occurrence of MAE was defined by having any of the following: death in lab, cardiac arrest, arrhythmia, new heart valve regurgitation, cardiac tamponade, air embolus, embolic stroke, device malposition/thrombosis, device embolization, new dialysis requirement, coronary artery compression, device erosion, postprocedure left ventricular assist device, bleeding, other vascular complication, unplanned surgery, or subsequent catheterization due to complications.
Statistical analysis
Data are shown as mean ± SD for continuous variables or median (IQR) and n (%) for categorical variables. When comparing SV vs BV patients and patients with MAE and those without MAE we used t test or a nonparametric alternative for continuous and χ^2^ test for categorical variables. Using these variables, we ran a multivariable logistic regression model predicting MAE with the following a priori variables: SV defect, age grouping, sex, race/ethnicity, insurance status, heterotaxy, chronic lung disease, diabetes mellitus, preprocedural antiarrhythmic drug, preprocedural antihypertensive drug, procedure status (elective, urgent, emergent, salvage), nonsinus rhythm, interventional procedure performed, prior intubation, systemic heparinization, and inotrope use at the start of the case. Summary statistics are all based on procedure-level data, and for the purposes of statistical analysis, procedures are considered independent observations. However, multivariable models were run with and without clustering procedures within patients in a hierarchical model. Because the clustered and unclustered models produced similar results, we used the clustered model for the final regression model presented. Data are shown as odds ratio and 95% CI. For all comparisons, a P < .05 was considered statistically significant for the analysis. All analysis was done with SAS 9.4 (SAS Institute).
Results
Patient characteristics and procedures
From January 1, 2011, through June 30, 2022, 3473 diagnostic or interventional cardiac catheterization procedures were performed on 2980 pediatric patients (age 0 days to 18 years) supported by ECMO at 101 centers in the US.
The study population was split into 2 cohorts based on SV physiology (31.6%) and BV physiology (68.4%). The mean age of the SV cohort was 0.77 ± 2.32 years compared with 3.60 ± 5.37 years for the BV cohort. Patients in the SV cohort were more likely to be neonates (47.3% vs 26.6%) or infants (37.6% vs 29.5%). There was a male predominance overall, 59.0% in the SV cohort and 53.5% in the BV cohort. The race distribution was primarily White (49.5%), followed by Black (17.9%), Hispanic (16.4%), other (12.2%), and Asian (4.0%). SV patients were more likely to have a higher proportion of White patients (54.0% vs 47.5%; P < .001). The presence of a genetic condition was reported in 14.0% of all patients. Each identified syndrome occurred more frequently in the BV cohort with the exception of heterotaxy, which occurred significantly more frequently in the SV cohort (Supplemental Table S1). Patients in the SV cohort were less likely to have comorbidities than the BV cohort (25.1% vs 32.8%). The payor mix was represented by private and public insurance equally for the entire cohort (40.5% vs 41.0%) with the SV cohort carrying a significantly higher portion of public insurance (44.7%). Patients in the SV cohort were more likely to have had a prior cardiac catheterization or a prior cardiac surgery compared to the BV cohort (27.3% and 35.3% compared with 26.5% and 27.4%). Only 13.6% of the cardiac catheterizations were performed “electively” in total with significant differences in the distribution of the nonelective catheterizations (urgent/emergent/salvage) between the SV and BV cohorts (Table 1).Table 1. Characteristics of pediatric patients undergoing cardiac catheterization while on ECMO from 2011-2022.CharacteristicTotal (N = 3473)Single ventricle (n = 1096)Biventricle (n = 2377)P valueAge, y2.71 ± 4.810.77 ± 2.323.60 ± 5.37<.001Age groups<.001 Age ≤ 30 d1151 (33.14%)518 (47.26%)633 (26.63%) Age 30-365 d1112 (32.02%)412 (37.59%)700 (29.45%) Age 1-8 y729 (20.99%)136 (12.41%)593 (24.95%) Age 9-17 y481 (13.85%)30 (2.74%)451 (18.97%)Sex.002 Male1919 (55.25%)647 (59.03%)1272 (53.51%) Female1554 (44.75%)449 (40.97%)1105 (46.49%)Race distributiona<.001 White1720 (49.52%)592 (54.01%)1128 (47.45%) Black622 (17.91%)190 (17.34%)432 (18.17%) Asian140 (4.03%)21 (1.92%)119 (5.01%) Hispanic568 (16.35%)171 (15.60%)397 (16.70%) Other423 (12.18%)122 (11.13%)301 (12.66%)Insurance payors.01 Private health insurance1407 (40.51%)420 (38.32%)987 (41.52%) Public health insurance1425 (41.03%)490 (44.71%)935 (39.34%) Others/missing641 (18.46%)186 (16.97%)455 (19.14%) Prior cardiac catheterization927 (26.77%)298 (27.26%)629 (26.54%).65 Prior cardiac surgery1033 (29.91%)385 (35.26%)648 (27.43%)<.001Procedure status<.001 Elective470 (13.56%)160 (14.63%)310 (13.06%) Urgent1463 (42.20%)509 (46.53%)954 (40.20%) Emergency1262 (36.40%)353 (32.27%)909 (38.31%) Salvage272 (7.85%)72 (6.58%)200 (8.43%)Missing624 Any genetic condition486 (14.03%)160 (14.61%)326 (13.77%).51 Any comorbidity1052 (30.36%)275 (25.09%)777 (32.80%)<.001Values are mean ± SD or n (%).ECMO, extracorporeal membrane oxygenation.aRace designation may be checked for more than 1 race.
Regarding procedural and hemodynamic data acquired while on ECMO, those in the SV cohort had a longer fluoroscopy time compared to the BV cohort (28.1 vs 24.8 minutes; P < .001). The rest of the hemodynamics were representative of adequate ECMO support including normal cardiac index (Supplemental Table S2).
Distribution of catheterization procedures
There was a slight propensity for interventional catheterizations (1822, 52.5%) compared with diagnostic-only catheterizations (1651, 47.5%). Of primary IMPACT procedures (288, 8.3%), proximal pulmonary artery (PA) stenting was performed most frequently (80 in the SV cohort, 97 in the BV cohort), followed by interventions on aortic coarctation (25 in the SV cohort, 19 in the BV cohort). Other primary IMPACT procedures performed in order of decreasing frequency include atrial septal defect closure, aortic valvuloplasty, patent ductus arteriosus (PDA) closure, pulmonary valvuloplasty, and transcatheter pulmonary valve replacement. There were 1534 (44.2%) nonprimary IMPACT procedures performed (Supplemental Table S3), including interventions on the atrial septum/Fontan baffle/atrial baffle which were performed most frequently (34 in the SV cohort, 744 in the BV cohort), followed by stent/device/coil placement on the systemic side (139 in the SV cohort, 125 in the BV cohort), balloon dilation on the venous side (105 in the SV cohort, 104 in the BV cohort), stent/device/coil placement on the venous side (110 in the SV cohort, 96 in the BV cohort), and biopsies (6 in the SV cohort, 195 in the BV cohort). Procedures such as balloon dilation on the systemic side, “other” procedures, and pulmonary vein interventions were performed infrequently (Table 2).Table 2. Procedural information of cardiac catheterizations for patients supported on ECMO.ProcedureTotal (N = 3473)Single ventricle (n = 1096)Biventricle (n = 2377)P valueDiagnostic catheterization only1651 (47.54%)611 (55.75%)1040 (43.75%)<.001Primary impact procedure288 (8.29%)113 (10.31%)175 (7.36%).003 Atrial septal defect closure21 (0.60%)0 (0%)21 (0.88%).001 Aortic coarctation procedure44 (1.27%)25 (2.28%)19 (0.80%)<.001 Aortic valvuloplasty16 (0.46%)4 (0.36%)12 (0.50%).57 Pulmonary valvuloplasty11 (0.32%)1 (0.09%)10 (0.42%).11 PDA closure16 (0.46%)2 (0.18%)14 (0.59%).10 Proximal PA stenting177 (5.10%)80 (7.30%)97 (4.08%)<.001 Transcatheter pulmonary valve replacement6 (0.23%)2 (0.18%)4 (0.17%).90Other procedure groups1534 (44.17%)372 (33.94%)1162 (48.49%)<.001 Balloon dilation on the venous side209 (6.02%)105 (9.58%)104 (4.38%)<.001 Stent/device/coil on the venous side206 (5.93%)110 (10.04%)96 (4.04%)<.001 Balloon dilation on the systemic side119 (3.43%)79 (7.21%)40 (1.68%)<.001 Stent/device/coil on the systemic side264 (7.60%)139 (12.68%)125 (5.26%)<.001 Pulmonary vein interventions64 (1.84%)15 (1.37%)49 (2.06%).16 Interventions on atrial septum/Fontan baffle/atrial baffle778 (22.40%)34 (3.10%)744 (31.30%)<.001 Biopsies201 (5.79%)6 (0.55%)195 (8.20%)<.001 “Other”121 (3.48%)34 (3.10%)87 (3.66%).40Values are n (%).ECMO, extracorporeal membrane oxygenation; PA, pulmonary artery; PDA, patent ductus arteriosus.
Procedural complications and MAE
The most common complications reported included arrhythmia (3.3%), bleeding events (2.7%), unplanned cardiac surgery (1.8%), and other unplanned surgery (1.8%). Complications were similar between the SV and BV cohorts except vascular complications necessitating intervention, which occurred significantly more frequently in the SV cohort compared to the BV cohort (1.6% vs 0.3%; P < .001) Overall outcomes demonstrated 6 total deaths in the lab (0.4%), and 41 episodes of cardiac arrest (1.2%). The total cohort had 53.2% survival to hospital discharge, with 45.2% in the SV cohort and 56.8% in the BV cohort (P < .001) (Table 3).Table 3. Complications and outcomes reported following cardiac catheterization for pediatric patients supported on ECMO.Procedural complicationsTotal (N = 3473)Single ventricle (n = 1096)Biventricle (n = 2377)P valueArrhythmia116 (3.34%)42 (3.83%)74 (3.11%).27New valve regurgitation7 (0.20%)3 (0.27%)4 (0.17%).52Tamponade15 (0.43%)2 (0.18%)13 (0.55%).13Air embolus4 (0.12%)3 (0.27%)1 (0.04%).06Embolic stroke6 (0.17%)1 (0.09%)5 (0.21%).43Device malposition or thrombus11 (0.32%)2 (0.18%)9 (0.38%).34Device embolization (requiring retrieval)4 (0.12%)1 (0.09%)3 (0.13%).78New requirement for dialysis19 (0.55%)3 (0.27%)16 (0.67%).14Coronary artery compression1 (0.04%)0 (0.00%)1 (0.06%).50Erosion1 (0.04%)0 (0.00%)1 (0.06%).50Airway event requiring escalation of care13 (0.37%)6 (0.55%)7 (0.29%).26Event requiring ECMO28 (0.81%)14 (1.28%)14 (0.59%).04Event requiring LVAD4 (0.12%)0 (0.00%)4 (0.17%).17Bleeding event95 (2.74%)41 (3.74%)54 (2.27%).01Vascular complications requiring treatment25 (0.72%)18 (1.64%)7 (0.29%)<.001Unplanned cardiac surgery63 (1.81%)20 (1.82%)43 (1.81%).97Unplanned vascular surgery7 (0.20%)4 (0.36%)3 (0.13%).14Unplanned other surgery62 (1.79%)27 (2.47%)35 (1.47%).04Subsequent cardiac catheterization20 (0.58%)9 (0.82%)11 (0.46%).19Outcomes Death in lab6 (0.37%)2 (0.33%)4 (0.39%).85 Cardiac arrest41 (1.18%)15 (1.37%)26 (1.09%).49 Alive at discharge1846 (53.15%)495 (45.16%)1351 (56.84%)<.001Values are n (%).ECMO, extracorporeal membrane oxygenation; LVAD, left ventricular assist device.
Next, we assessed the occurrence of MAE. Those with MAE were similar in age, sex, race, and insurance coverage to those who did not experience MAE. MAE occurred more frequently in neonates (155/1151, 13.5%) than other age groups. The history of prior cardiac catheterization or prior cardiac surgery was not significantly different between those with or without MAE. The presence of a genetic syndrome was not predictive of MAE, and no single genetic syndrome was significantly associated with MAE. Overall presence of a comorbidity was not predictive of MAE, but diabetes mellitus and chronic lung disease were more frequently associated with MAE (Supplemental Table S4). A procedure status of salvage procedure was more likely to result in MAE (49/272, 18.0%), compared to less emergent procedure indications (Table 4).Table 4. Characteristics of patients with MAE undergoing cardiac catheterization while on ECMO from 2011 to 2022.CharacteristicTotal (N = 3473)MAE (n = 400)No MAE (n = 3073)P valueAge, y2.71 ± 4.812.49 ± 4.712.73 ± 4.82.34Age groups.08 Age ≤ 30 d1151 (33.14%)155 (38.75%)996 (32.41%) Age 30-365 d1112 (32.02%)118 (29.50%)994 (32.35%) Age 1-8 y729 (20.99%)74 (18.50%)655 (21.31%) Age 9-17 y481 (13.85%)53 (13.25%)428 (13.93%)Weight14.05 ± 20.5113.14 ± 20.4014.17 ± 20.52.35Sex.11 Male1919 (55.25%)206 (51.50%)1713 (55.74%) Female1554 (44.75%)194 (48.50%)1360 (44.26%)Race distributiona.23 White1720 (49.52%)202 (50.50%)1518 (49.40%) Black622 (17.91%)78 (19.50%)544 (17.70%) Asian140 (4.03%)21 (5.25%)119 (3.87%) Hispanic568 (16.35%)52 (13.00%)516 (16.79%) Other423 (12.18%)47 (11.75%)376 (12.24%)Insurance payors.71 Private health insurance1407 (40.51%)155 (38.75%)1252 (40.74%) Public health insurance1425 (41.03%)171 (42.75%)1254 (40.81%) Others/missing641 (18.46%)74 (18.50%)567 (18.45%) Prior cardiac catheterization927 (26.77%)99 (24.75%)828 (26.94%).36 Prior cardiac surgery1033 (29.91%)119 (29.75%)914 (29.74%).97Procedure status<.001 Elective470 (13.56%)42 (10.5%)428 (13.93%) Urgent1463 (42.20%)153 (38.25%)1310 (42.63%) Emergency1262 (36.40%)155 (38.75%)1107 (36.02%) Salvage272 (7.85%)49 (12.25%)223 (7.26%) Missing615Any genetic condition486 (14.03%)58 (14.50%)428 (13.93%).78Any comorbidity1052 (30.36%)109 (27.25%)943 (30.69%).15Values are mean ± SD or n (%).ECMO, extracorporeal membrane oxygenation; MAE, major adverse event.aRace designation may be checked for more than 1 race.
We also assessed the occurrence of MAE by procedure. Diagnostic-only procedures on ECMO had a 10.6% (175/1651) rate of MAE. Primary IMPACT procedures had a 14.9% (43/288) rate of MAE, and nonprimary IMPACT interventional procedures had an 11.9% (182/1534) rate of MAE. Of the primary IMPACT interventional procedures performed while on ECMO, only aortic coarctation procedures were found to be significantly more associated with MAE with MAE occurring in 27.3% (12/44) of these procedures. The MAE rates were 25.0% (4/16) for PDA closures, 18.8% (3/16) for aortic valvuloplasty, 14.1% (25/177) for proximal PA stenting, 4.8% (1/21) for atrial septal defect closure, and 0% (0/11) for pulmonary valvuloplasty and (0/6) transcatheter pulmonary valve replacement. Of the nonprimary IMPACT interventional procedures, only stent/device/coil placement on the venous side and “other” interventions were found to be significantly more associated with MAE, with MAE occurring in 16.0% (33/206) and 22.3% (27/121) of these procedures. The MAE rates were 15.1% for balloon dilations on the systemic side, 13.3% for stent/device/coil placement on the systemic side, 12.4% for balloon dilation on the venous side, 11.9% for biopsies, 10.7% for interventions on the atrial septum/Fontan baffle/atrial baffle, and 7.8% for pulmonary vein interventions (Table 5).Table 5. Major adverse events based on procedural category for patients undergoing cardiac catheterization while on ECMO.ProcedureTotal (N = 3473)MAE (n = 400)No MAE (n = 3073)P valueDiagnostic-only catheterization1651 (47.54%)175 (43.75%)1476 (48.03%).11Primary impact procedure288 (8.29%)43 (10.75%)245 (7.97%).058 Atrial septal defect closure21 (0.60%)1 (0.25%)20 (0.65%).33 Aortic coarctation procedure44 (1.27%)12 (3.00%)32 (1.04%)<.001 Aortic valvuloplasty16 (0.46%)3 (0.75%)13 (0.42%).36 Pulmonary valvuloplasty11 (0.32%)0 (0%)11 (0.36%).23 PDA closure16 (0.46%)4 (1.00%)12 (0.39%).09 PA stenting177 (5.10%)25 (6.25%)152 (4.95%).26 Transcatheter pulmonary valve replacement6 (0.23%)0 (0%)6 (0.20%).42Other procedure groups1534 (44.17%)182 (45.50%)1352 (44.0%).57 Balloon dilation on the venous side209 (6.02%)26 (6.50%)183 (5.96%).67 Stent/device/coil on the venous side206 (5.93%)33 (8.25%)173 (5.63%).04 Balloon dilation on the systemic side119 (3.43%)18 (4.5%)101 (3.29%).21 Stent/device/coil on the systemic side264 (7.60%)35 (8.75%)229 (7.45%).36 Pulmonary vein interventions64 (1.84%)5 (1.25%)59 (1.92%).35 Interventions on atrial septum/Fontan baffle/atrial baffle778 (22.40%)83 (20.75%)695 (22.62%).40 Biopsies201 (5.79%)24 (6.00%)177 (5.76%).85 “Other”121 (3.48%)27 (6.75%)94 (3.06%)<.001Values are n (%).ECMO, extracorporeal membrane oxygenation; MAE, major adverse event; PA, pulmonary artery; PDA, patent ductus arteriosus.
Patients with MAE had high fluoroscopy times, and higher contrast volumes than those without MAE. The rest of the hemodynamics were comparable including cardiac index while supported by ECMO (Supplemental Table S5).
Lastly, we assessed risk factors associated with MAE. Using regression analysis with clustering of the procedures within patients, SV physiology (OR, 1.31; 95% CI, 1.02-1.69) was found to be significantly associated with MAE in patients undergoing cardiac catheterization on ECMO. Other significant risk factors include interventional catheterization, non-Hispanic race, diabetes mellitus, procedure status classified as salvage vs elective, and systemic heparinization (Table 6 and Central Illustration).Table 6. Predictors of major adverse events following cardiac catheterization in pediatric patients on ECMO using a clustered model.Odds ratio (95% CI)P valueSingle ventricle defect present1.31 (1.01-1.69).04Age group: ≤30 d vs 9-17 y1.26 (0.84-1.9).26Age group: 30-365 d vs 9-17 y0.99 (0.66-1.48).95Age group: 1-8 y vs 9-17 y0.89 (0.58-1.36).58Sex: male vs female0.8 (0.64-1.01).057Race/ethnicity: Hispanic vs NH-White0.67 (0.46-0.96).03Race/ethnicity: NH-Black vs NH-White1.07 (0.78-1.47).67Race/ethnicity: NH-Asian vs NH-White1.42 (0.82-2.44).21Race/ethnicity: Other/multiple vs NH-White1.07 (0.74-1.56).71Insurance: public vs private1.11 (0.85-1.44).46Insurance: other/none vs private0.99 (0.71-1.38).95Heterotaxy1.3 (0.78-2.16).31Chronic lung disease0.68 (0.42-1.09).11Diabetes3.88 (1.29-11.65).016Preprocedural antiarrhythmic therapy1.28 (0.96-1.7).09Preprocedural antihypertensive therapy0.75 (0.55-1.02)0.07Status: urgent vs elective1.05 (0.69-1.61).81Status: emergency vs elective1.23 (0.8-1.9).34Status: salvage vs elective1.73 (1.03-2.93).040Rhythm: nonsinus vs sinus1.3 (0.95-1.76).10Any procedure vs diagnostic catheterization1.35 (1.06-1.71).015Previous intubation1.35 (0.78-2.32).28Systemic heparinization preprocedure1.46 (1.12-1.9).006Inotrope preprocedure1.08 (0.8-1.47).60ECMO, extracorporeal membrane oxygenation; NH, non-Hispanic.Central IllustrationCardiac catheterizations on pediatric patients on extracorporeal membrane oxygenation (ECMO) had an 11.5% rate of major adverse events (MAE). Risk factors were single ventricle (SV) physiology, interventional procedure, procedure status classified as salvage, non-Hispanic race, diabetes, and systemic heparinization. Bi-V, biventricular; IMPACT registry, IMproving Pediatric and Adult Congenital Treatments.
Discussion
This is the first large, multicenter study of the performance and procedural safety of cardiac catheterization in pediatric patients supported on ECMO, including those with SV circulation. Overall, this study of over 3400 procedures including over 1000 procedures in SV patients demonstrated a relatively low procedural risk given the clinical acuity of these patients, but about double the risk associated with cardiac catheterization in pediatric patients not on ECMO. The study analyzed diagnostic and procedural catheterizations and identified modifiable and nonmodifiable patient and procedural factors associated with MAE during such catheterizations. Lastly, the study provides benchmarking data for quality improvement, as well as for future studies aimed at further improving the performance of said procedures.
Currently, there are very limited data on the safety of cardiac catheterizations performed in pediatric patients supported on ECMO. Survival to hospital discharge in pediatric patients on ECMO undergoing cardiac catheterization is widely variable and ranges from 29% to 74% with rates of procedural MAE ranging from 0% to 18%.4, 5, 6^,^9, 10, 11, 12, 13, 14 These studies are mostly single-center, small studies with lower survival rates in the earliest studies and improvement in the modern era.4, 5, 6^,^9, 10, 11, 12, 13, 14 In the present study, survival to hospital discharge was 57% in the BV cohort and 45% in the SV cohort, with an overall 11.5% rate of MAE. When compared to the previously described population on ECMO, rates of procedural complications in our study were similar.
Comparing event rates across studies is challenging as there is ambiguity as to what constitutes an MAE. A previous IMPACT report looking at all pediatric patients undergoing catheterization reported an MAE rate of 7%.15 The definition of MAE used in our study was very similar to this report. The Congenital Cardiac Catheterization Outcomes Project, which collects data on a similar patient population, has reported an overall adverse event rate of 11%, with hemodynamically significant adverse events occurring in 5% of cases.16 Our MAE variables are similar to the hemodynamically significant adverse events reported in that study. Pediatric patients on ECMO are high-risk patients and understandably accrue more risk than the general population, roughly 2 times the amount.
In addition, our study consisted of a significant cohort of SV patient procedures (>1000). This allowed us to assess the impact of an underlying diagnosis of SV on MAE and outcomes in detail. We found that MAE were more likely to occur in SV patients (OR, 1.31; 95% CI, 1.01-1.69; P = .04). SV patients who underwent catheterization while on ECMO were younger and more likely to have had a prior cardiac catheterization or cardiac surgery compared to BV patients. This association of SV patients on ECMO and relative risk for MAE is a novel finding.
Major adverse events were also more likely to occur when the procedure involved intervention rather than just diagnostic catheterization. Patients who underwent balloon atrial septostomy while on ECMO, presumably for left atrial hypertension, have been previously described and perhaps carry a unique or different risk stratification.17 A 2020 study from the IMPACT registry on atrial septostomy performed in patients on ECMO reported a 54% hospital survival17 which approaches our BV cohort survival rate. Not surprisingly, in our group of patients, primary IMPACT interventions including aortic coarctation interventions, PDA closure, aortic valvuloplasty, and proximal PA stenting all had much higher rates of MAE compared to the same interventions performed in patients not on ECMO from the same registry.15^,^18 However, atrial septal defect closure, pulmonary valvuloplasty, and transcatheter pulmonary valve placement in this population had lower rates of MAE than in prior registry reports. Albeit each of these procedures was performed infrequently in this study group. The majority of interventions performed were nonprimary IMPACT procedures, and individual procedures occurred infrequently which led us to create 8 broad groups of interventions. Overall, interventions performed on ECMO carry a higher risk of MAE than when performed off ECMO.16^,^18^,^19 Based on our grouping of nonprimary IMPACT procedures, only stent/device/coil placement on the venous side and “other” interventions were significantly more associated with MAE, occurring in 16% and 22% of those procedures, respectively. It is unclear why interventions on the right side of the heart or the systemic venous side had higher rates of MAE. With the most common MAE being arrhythmia, perhaps this is more frequent with right-sided procedures that involve intracardiac catheter manipulation. The “other” group is a heterogeneous group of procedures making it difficult to attribute any meaning to this association with MAE. Looking more closely at this group to further risk stratify procedures could be an area of interest for future studies given the high rate of MAE.
Major adverse events also occurred more frequently in patients whose catheterization was categorized as a salvage procedure, with BV patients more frequently undergoing emergent and salvage procedures. This may be a reflection on the acuity of the patient status, lack of preparatory planning, and the urgency of the procedure rather than the performance of the procedure itself. Nonetheless, it underscores the point that any advance planning and avoidance of “last minute” intervention as a rescue, may impact the outcomes of such procedures. That being said, there may be subjectivity in labeling a procedure elective, urgent, or salvage procedure as the data dictionary definitions do not specify a scenario that includes ECMO support. Including further guidance within the data dictionary may help improve consistency in reporting and interpretation of such data.
Systemic heparinization was also significantly associated with MAE. We hesitate to attribute too much clinical significance to this finding given that all patients on ECMO are systemically anticoagulated at baseline. We considered comparing the activated clotting time between the groups but there was a large portion of missing data for that variable. Non-Hispanic race and diabetes mellitus were also more frequent in patients with MAE. Regarding racial disparities, ECMO utilization and outcomes in pediatric patients based on race have been studied previously in large, multicenter studies.20^,^21 Our cohort had a similar race breakdown as these population-based ECMO utilization studies. A review of the Pediatric Cardiac Critical Care Consortium clinical registry found that Black race and “other” races were associated with increased ECMO utilization during surgical hospitalizations, but racial disparities in outcomes were not explained by differences in ECMO utilization.20 Data from the Extracorporeal Life Support Organization Registry demonstrated that Black race and Hispanic ethnicity were independently associated with mortality in children who require cardiac ECMO.21 This factor certainly warrants ongoing critical evaluation. We also found the lack of association of MAE with genetic syndromes as noteworthy, although this may be limited by registry reporting accuracy and practice variation of genetic testing and documentation between centers.
Outcomes on ECMO continue to be suboptimal in general, and hospital survival is low. There are data to show that performing catheterizations on ECMO early can improve outcomes.4, 5, 6^,^14 Here, we provide data that catheterization on ECMO can be done with relatively low risk in what is considered a high-risk population.
As with all large registry studies, there are inherent limitations such as lack of details and granularity especially around specific cardiac surgeries, inability to account for practice variability among participating and nonparticipating centers, potentially unmeasured confounding variables, and variability in coding and reporting. For example, 0.8% of patients in our study had an event requiring ECMO but also had ECMO in place at the start of the procedure, which we included in our complications but do not necessarily have a good clinical explanation for. The registry has in place rigorous quality assurance standards and periodic data audits to combat some of these limitations. The registry has limited information about the impact of interventions done such as serial hemodynamic data or follow-up surgical interventions. Surgical intervention following catheterization may be to rescue from a complication. However, in other cases, the diagnostic information from the procedure may have guided a surgical intervention allowing for successful recovery. Such detailed information to classify a follow-up surgery after the procedure was not available. Lastly, the timing of the procedure and separation from ECMO could not be ascertained to evaluate the immediate impact of the procedure on the ECMO need. From a statistical standpoint, large registry analysis with multiple comparisons could lead to type I error especially when using a simple P value of <.05. We did not adopt overly conservative methods for correction due to the potential for type II error.
Conclusion
Cardiac catheterization and interventions can be performed safely on pediatric patients supported by ECMO, albeit with higher rates of adverse events compared to patients not on ECMO. We have provided benchmarking data regarding outcomes and identified procedural and patient risk factors for MAE including the presence of SV circulation and the performance of the procedure as a salvage procedure. Further efforts should focus on validation studies, and modification of preprocedural risk factors including avoiding emergent or salvage procedures and optimizing patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chrysostomou C.Morell V.O.Kuch B.A.O’Malley E.Munoz R.Wearden P.D.Short- and intermediate-term survival after extracorporeal membrane oxygenation in children with cardiac disease J Thorac Cardiovasc Surg 1462201331732510.1016/j.jtcvs.2012.11.01423228400 · doi ↗ · pubmed ↗
- 2Bhatt P.Lekshminarayanan A.Donda K.National trends in neonatal extracorporeal membrane oxygenation in the United States J Perinatol 38820181106111310.1038/s 41372-018-0129-429795325 · doi ↗ · pubmed ↗
- 3Geisser D.L.Thiagarajan R.R.Scholtens D.Development of a model for the pediatric survival after veno-arterial extracorporeal membrane oxygenation score: the Pedi-SAVE score ASAIO J 681120221384139210.1097/MAT.000000000000167835184092 · doi ↗ · pubmed ↗
- 4Kato A.Lo Rito M.Lee K.-J.Impacts of early cardiac catheterization for children with congenital heart disease supported by extracorporeal membrane oxygenation Catheter Cardiovasc Interv 895201789890510.1002/ccd.2663227416545 · doi ↗ · pubmed ↗
- 5Abraham B.P.Gilliam E.Kim D.W.Wolf M.J.Vincent R.N.Petit C.J.Early catheterization after initiation of extracorporeal membrane oxygenation support in children is associated with improved survival Catheter Cardiovasc Interv 884201659259910.1002/ccd.2652627037743 · doi ↗ · pubmed ↗
- 6Burke C.R.Chan T.Rubio A.E.Mc Mullan D.M.Early cardiac catheterization leads to shortened pediatric extracorporeal membrane oxygenation run duration J Interv Cardiol 302201717017610.1111/joic.1236828271557 · doi ↗ · pubmed ↗
- 7Martin G.R.Beekman R.H.Ing F.F.The IMPACT Registry TM: I Mproving Pediatric and Adult Congenital Treatments Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 1312010202510.1053/j.pcsu.2010.02.00420307857 · doi ↗ · pubmed ↗
- 8Malenka D.J.Bhatt D.L.Bradley S.M.The national cardiovascular data registry data quality program 2020: JACC state-of-the-art review J Am Coll Cardiol 791720221704171210.1016/j.jacc.2022.02.03435483759 · doi ↗ · pubmed ↗