Basilar Artery Fenestration Aneurysm Treated With the Woven EndoBridge (WEB) Device: A Case Report and Review of the Literature
Albatool M Mansouri, Wesam O Mandoura, Jehad K Alharbi, Renad A Alsharif, Naif Alharbi

TL;DR
A rare case of a basilar artery fenestration aneurysm was successfully treated using a new endovascular device called the Woven EndoBridge (WEB).
Contribution
This case report highlights the successful use of the WEB device for treating a rare and complex basilar artery fenestration aneurysm.
Findings
The WEB device was successfully used to embolize a ruptured proximal basilar artery fenestration aneurysm.
The treatment resulted in favorable outcomes with fewer complications compared to traditional surgical methods.
Abstract
Fenestration of the basilar artery (BA) is a rare congenital malformation resulting from anomalies in embryonic vascular development. Basilar artery fenestration aneurysms (BAFAs), especially in the proximal region, present unique challenges in neurosurgery. Their location in the critical and eloquent brainstem area makes open surgical clipping high-risk. Endovascular management has emerged as a less invasive alternative for aneurysms in such locations. The Woven EndoBridge (WEB) device (Terumo Neuro, Aliso Viejo, CA, United States) is a self-expanding, intrasaccular flow disruptor designed to treat wide-necked aneurysms without the need for additional devices, leading to improved outcomes and fewer complications from further interventions. This case describes a 52-year-old female patient with hypertension who presented to the emergency room following a two-minute seizure attack,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
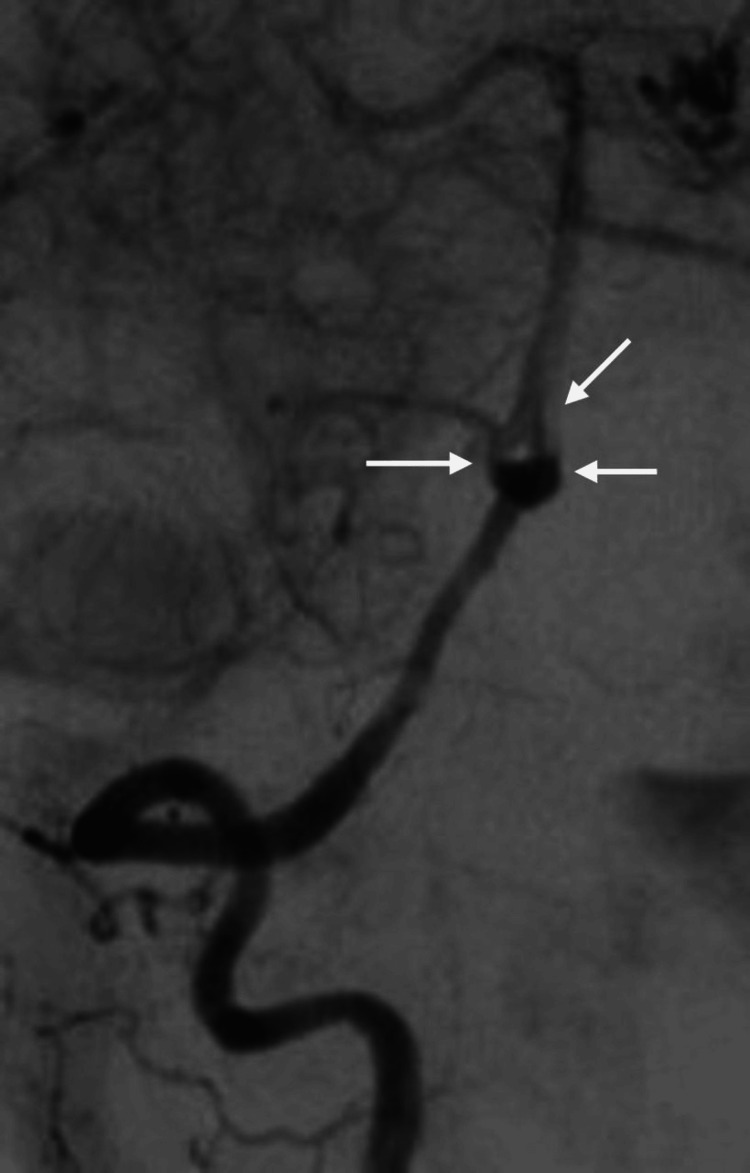 Figure 1
Figure 1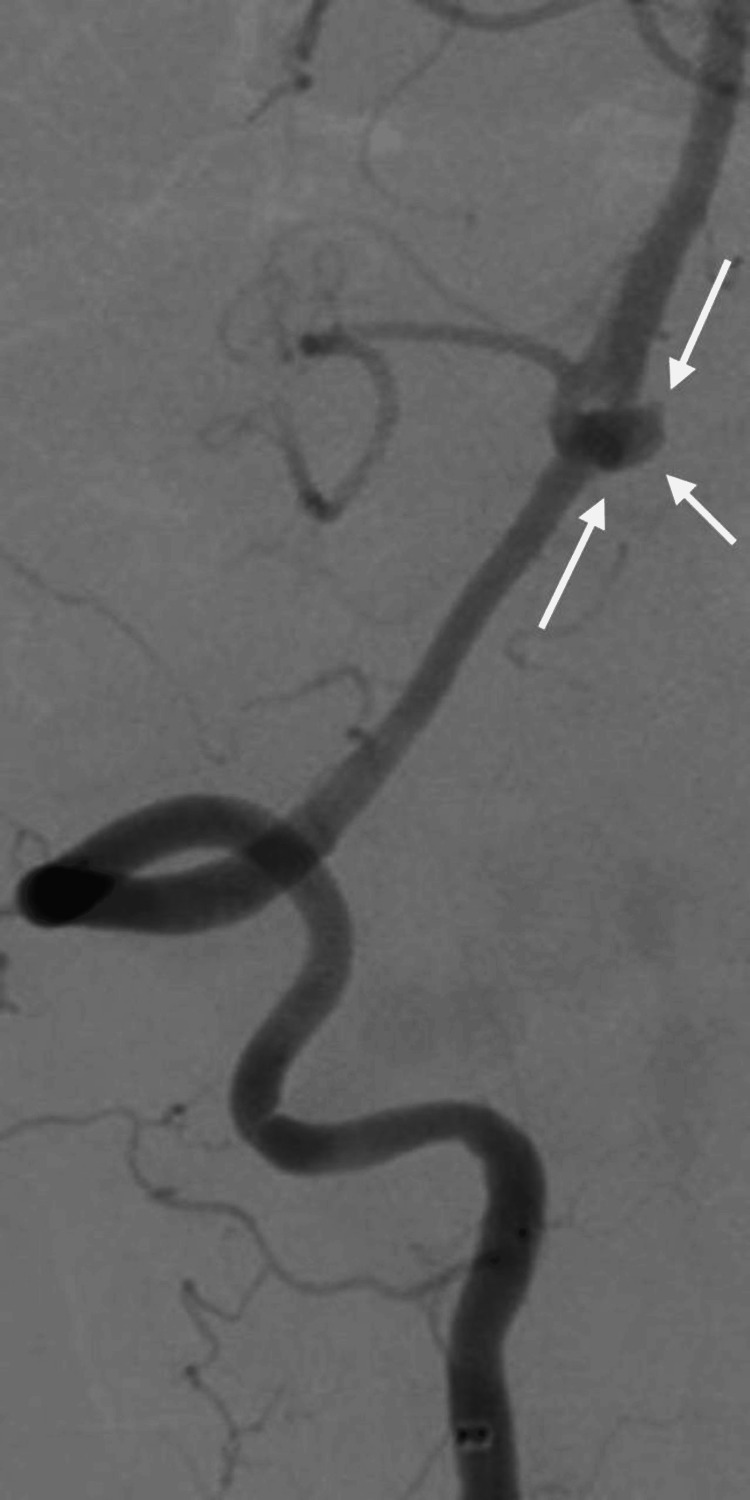 Figure 2
Figure 2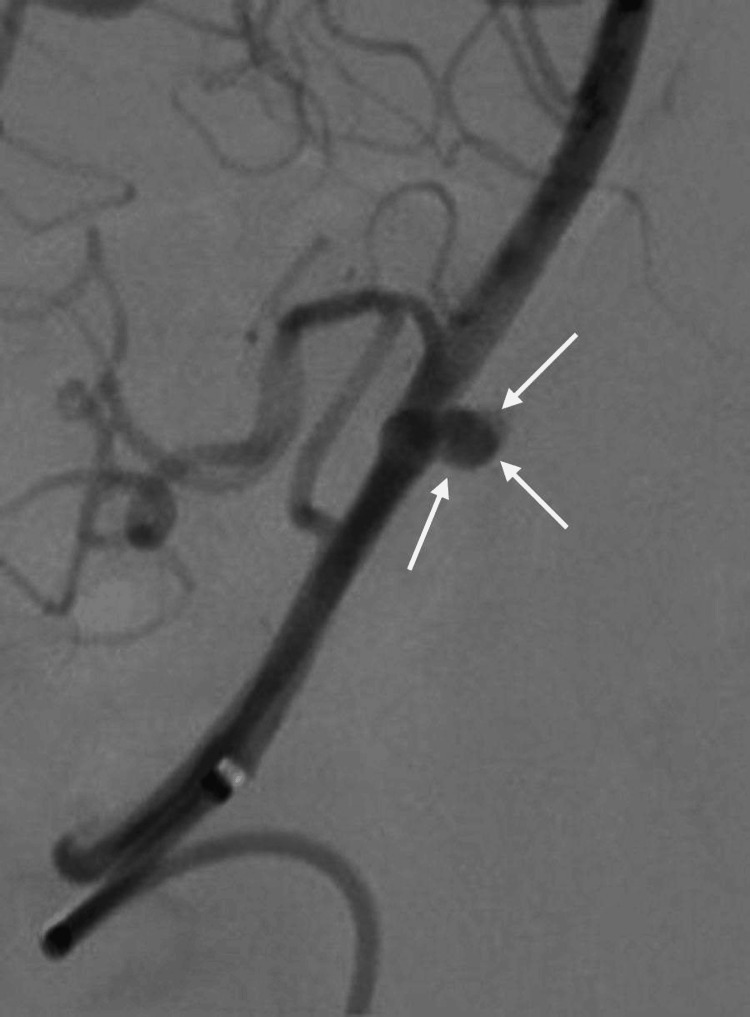 Figure 3
Figure 3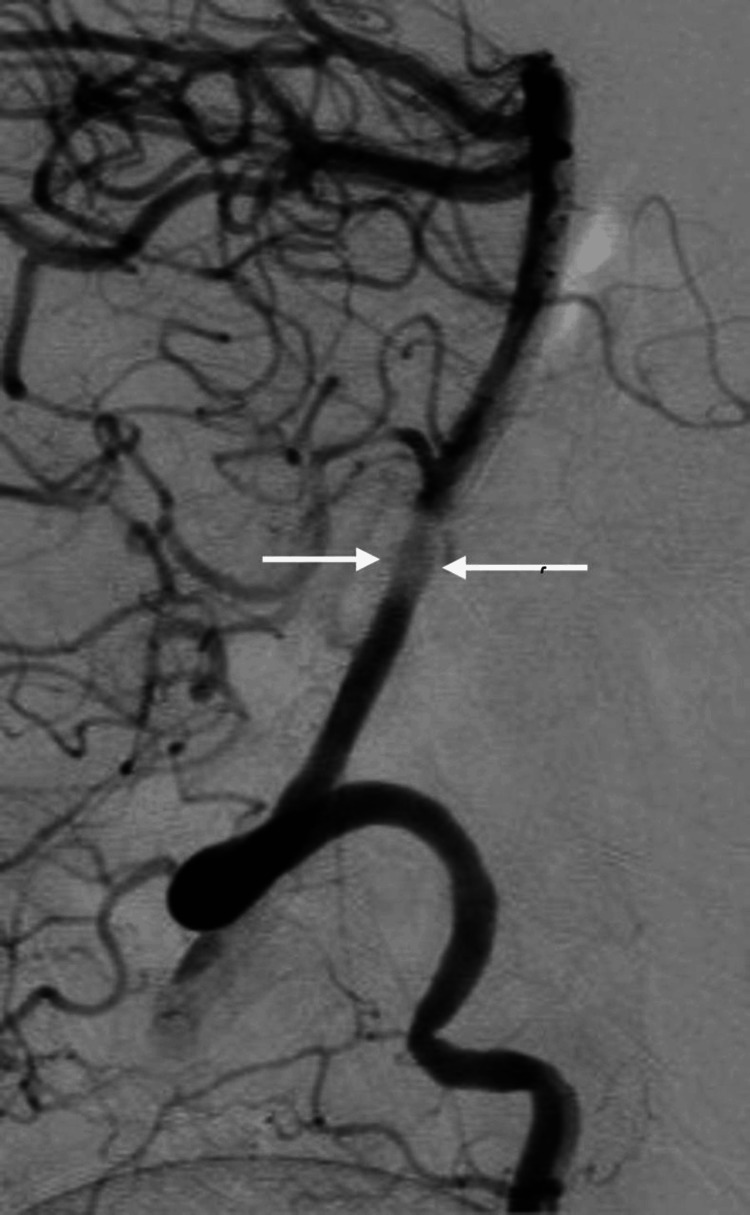 Figure 4
Figure 4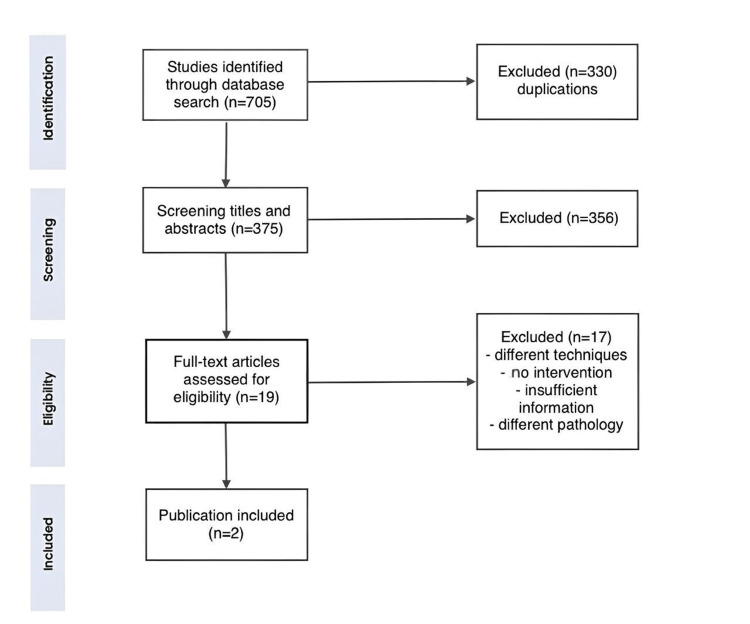 Figure 5
Figure 5| Author | de Almeida Silva et al. [ | Drijkoningen et al. [ | Current study |
| Year | 2021 | 2021 | 2024 |
| Demographics | |||
| Sex | Female | Female | Female |
| Age in years | 75 | 66 | 52 |
| DM | No | No | No |
| HTN | Yes | No | Yes |
| Smoking | Yes | No | No |
| Clinical presentation | |||
| Presenting symptoms | Headache | Headache and nausea | Headache and seizure |
| Initial imaging | CT | CT | CT |
| Confirmatory imaging | DSA | DSA | DSA |
| Aneurysm morphology | |||
| Site | Lower one-third of the BA | Vertebrobasilar junction | Proximal tip of the BA |
| Morphology | Sac and neck | Blood blister-like aneurysm | Sac and neck |
| Sac size | 5.5 x 5.5 mm | 2 mm | 4.4 mm |
| Neck size | 5.2 mm | - | 2 mm |
| Rupture | No | Yes | Yes |
| Procedure | |||
| Preop medications | ASA 200 mg/day | No | No |
| Peri-op medication | Heparinization with 5,000 IU of UFH | Heparinization with 3,000 IU of UFH | Heparinization with 3,000 IU of UFH |
| Postop medication | No | ASA 81 mg | ASA 81 mg |
| WEB size | 6 x 3 mm | 4.4 x 2.6 mm | 2 x 3.2 mm |
| Complications | |||
| Mortality | No | No | No |
| Recurrence | No | No | No |
| Retreatment | No | No | Yes |
| New neurological deficits | No | No | No |
| Follow-up | |||
| Duration (mean) | 6 m | 3 m | 1 m |
| New neurological deficits | No | No | No |
| Angiography | 6 m | - | - |
| MRI | - | 3 m | - |
| Occlusion | Yes | Yes | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Aortic Disease and Treatment Approaches · Aortic aneurysm repair treatments
Introduction
The basilar artery (BA) is formed by the joining of two vertebral arteries at the medullo-pontine junction. It gives rise to three cerebellar arteries and two posterior cerebral arteries before terminating in the posterior cerebral circulation [1,2]. Fenestration of the BA results from the incomplete fusion of the longitudinal neuronal arteries, creating an artery with two lumens and possibly two adventitia [3-5]. With an approximate prevalence of 1%, the BA is the second most common site of cerebral arterial fenestrations, following the anterior communicating artery (AComm) [4-6]. These fenestrations typically occur in the proximal part of the BA trunk, just above the vertebrobasilar junction, and have been associated with aneurysm development at the fenestrated segments [3,4,7,8].
Proximal BA aneurysms present a unique challenge in neurointerventional surgery. Their location in the critical and eloquent brainstem area makes open surgical clipping high-risk. Over the past two decades, endovascular embolization has emerged as a minimally invasive alternative for the treatment of these complex lesions. From coil embolization, whether balloon or stent assisted, to flow diverters and flow disrupters, numerous techniques can be used in these cases.
Here, we present the case of a 52-year-old female patient with a fenestration of the proximal BA trunk and a ruptured aneurysm at the fenestrated segment, accompanied by diffuse subarachnoid hemorrhage (SAH). The aneurysm was successfully embolized using the Woven EndoBridge (WEB; Terumo Neuro, Aliso Viejo, CA, United States) intrassacular flow disruption device, followed by the deployment of a flow diverter. We also review the current literature on endovascular embolization for basilar artery fenestrated aneurysms (BAFAs) using the WEB device, alongside published reports of similar cases.
Case presentation
A 52-year-old female patient with hypertension presented to the emergency room following a 2-minute seizure attack, preceded by a severe headache that began an hour earlier. She also experienced palpitations and chest tightness. Upon presentation, the Glasgow Coma Scale (GCS) was 8/15, Hunt and Hess (H&H) IV, and World Federation of Neurological Surgeons (WFNS) IV. The pupils were 3 mm in size, equal, and reactive bilaterally. The patient exhibited more movement on her left side than on the right, with all brainstem reflexes intact. Computerized tomography (CT) and CT angiography (CTA) of the brain revealed fenestration of the BA trunk, alongside a ruptured basilar tip aneurysm associated with diffuse subarachnoid hemorrhage (SAH) and intraventricular hemorrhage, with a modified Fisher (mFISHER) grade II. In addition, the patient developed non-communicating hydrocephalus and underwent external ventricular drainage (EVD) insertion. The patient was transferred to our hospital for neurointerventional management. Digital subtraction angiography (DSA) confirmed a BA deformity (fenestration) (Figure 1) with an outpouching involving the anterior part of the proximal BA, likely representing a saccular aneurysm just above the vertebrobasilar junction (Figure 2 and Figure 3). The neck of the aneurysm measured 2 mm, and the sac measured 4 x 4 mm in the anteroposterior (AP) and transverse (TR) planes.
DSA pre-op showing fenestration of the basilar artery (white arrows)DSA: digital subtraction angiography.
DSA pre-op showing aneurysmal sac out of the fenestration (white arrows)DSA: digital subtraction angiography.
DSA pre-op showing an oblique view of the aneurysm (white arrows)DSA: digital subtraction angiography.
After a multidisciplinary meeting, it was decided to use the WEB device for an endovascular approach. Under sterile aseptic technique and general anesthesia, a 6-French sheath and catheter were inserted through the right femoral artery, with continuous flushing using heparinized saline. Under fluoroscopic guidance, with the primary feeding artery coming from the right vertebral artery, the main findings included BA fenestration with an intrasaccular aneurysm, as well as an incidental middle cerebral artery (MCA) trifurcation. The Traxcess system (Terumo Neuro, Aliso Viejo, CA, United States) was then used for catheterization and delivery of the WEB device, which measured 2 x 3.2 mm. After the device was deployed, a 10-minute angiography before detachment showed successful embolization of the aneurysm without complications. The arteriotomy was sutured using the ProGlide closure device (Abbott Laboratories, Chicago, IL, United States), followed by manual compression for 10 minutes. The patient was placed on aspirin 81 mg daily, in addition to the SAH protocol. Twenty-one days later, the patient underwent diagnostic DSA, which revealed significant recanalization of the aneurysm at the fenestration set. A second therapeutic DSA was performed the following day, and successful embolization of the proximal BAFA was achieved using flow diversion (Figure 4).
DSA after flow diversion installment (white arrows)DSA: digital subtraction angiography.
The patient was discharged on dual antiplatelet therapy (aspirin 81 mg and clopidogrel 75 mg daily) for three months, with no active issues. No seizures or neurological deficits were reported at the one-month follow-up. Aneurysm assessment with cerebral angiography is planned after two months.
Discussion
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we systematically reviewed the literature related to BAFA on PubMed, Medline, and Web of Science (WoS) using the following search terms: ("fenestration" OR "fenestrated" OR "fenestrations") AND ("basilar" OR "BA") AND ("aneurysm" OR "aneurysms"). This search included studies published up to August 2024. We also screened the references of the included studies for possible relevant articles. We included case reports, case series, case-control studies, and observational studies published in English. Eligible articles met the following criteria: (1) patients with BAFAs, whether ruptured or unruptured, (2) endovascular treatment of BAFAs using the WEB device, (3) sufficient reporting of aneurysm morphology, (4) angiographic results pre- and postoperatively, and (5) reporting of complications peri- or postoperative complications. We excluded abstracts, conference papers, animal studies, review articles, and studies using treatment methods other than WEB, and articles with insufficient reporting of aneurysm morphology or treatment modality (Figure 5).
PRISMA flowchartPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Two authors independently screened titles and abstracts, followed by a full-text screening of the included studies, with a third reviewer resolving any discrepancies.
BA fenestration is an anatomical variant in which the artery forms two lumens, each lined with muscular and endothelial layers, and may involve the adventitia. This phenomenon occurs due to the failure of fusion of the primitive longitudinal neuronal arteries during embryonic development [3,6,7]. BA fenestration is the second most common site of cerebral arterial fenestrations after AComm. However, it is easier to detect on angiography than AComm due to its larger size [4-6]. While BA fenestrations can occur at any part of the trunk, those in the proximal segment, just above the vertebrobasilar junction, are the most common [3,4,7]. This involvement of the lower half of the vessel is believed to be due to the cranio-caudal fusion of the longitudinal arteries during development [7].
Aneurysms associated with BA fenestration have been widely reported [3-6,8-10], especially in the proximal segment [3,8,11]. Aneurysms arising from the proximal BA, defined as those distal to the origin of the anterior inferior cerebellar artery, are particularly challenging due to their proximity to eloquent brainstem structures and the BA bifurcation. The walls of the fenestrated limbs have normal architecture laterally, but medially, there is an elastin discontinuity at the proximal part, along with subendothelial thinning [3,8,12]. These structural changes are also observed in cerebral arterial bifurcations. Furthermore, high blood flow and excessive pressure on the fenestration wall lead to hemodynamic instability, significantly increasing the risk of aneurysm formation [3,4,8].
Surgically approaching aneurysms in such a location while minimizing complications presents a challenge. The approach requires cranial access to the lower part of the brainstem, an area containing the lower cranial nerves and numerous small arterial perforators. This complex anatomy makes successful microsurgical clipping difficult [4,8,11]. Several endovascular techniques have been described for treating proximal BA aneurysms, including coil embolization, balloon-assisted coil embolization, stent-assisted coil embolization, flow diversion, and parent vessel occlusion [4,8]. The choice of technique depends on the aneurysm size, morphology, neck width, and the presence of branches incorporated into the aneurysm dome [6,8,13]. To our knowledge, this is the third reported case, alongside Drijkoningen et al. [10] and de Almeida Silva et al. [4], of treating an aneurysm at the tip of a fenestrated BA using the WEB device, meeting the inclusion criteria outlined earlier. Table 1 displays data from two previous cases, in addition to the current study, including demographics, clinical presentation, aneurysm morphology, and patient procedural and clinical outcomes. The study by Styczen et al. [14] also reports the treatment of BAFA with endovascular techniques including WEB. However, it did not provide sufficient information to meet the criteria for our study.
The WEB device is an intrasaccular flow disruptor featuring a self-expanding braided mesh made of platinum-cored nitinol wires, delivered via a micro-catheter. Upon deployment, the mesh covers the aneurysm neck, achieving metallic coverage ranging from 55% to 100%. This coverage disrupts intra-aneurysmal blood flow, promoting intrasaccular thrombosis and promoting neo-endothelialization [4,15]. Specifically designed to treat wide-necked aneurysms without the need for additional supporting devices [15], the WEB device has been successfully used in a wide range of aneurysms, regardless of neck size, morphology, rupture status, or location [15-17]. A case reported by Drijkoningen et al. [10] highlighted a unique blood blister-like aneurysm in a BA fenestration, where the sac was smaller than the neck in both lobes; despite this, the WEB device was still effectively used. In a meta-analysis by Asnafi et al. [17], the initial occlusion rate for wide-neck bifurcation aneurysms was higher in patients treated with the WEB device (60%) compared to those treated with stent-assisted coiling (54%). Furthermore, the need for pre- and/or perioperative antiplatelet therapy is reduced when using a WEB device, especially for patients with ruptured aneurysms, as demonstrated in the current case and the case reported by Drijkoningen et al. [10].
In the current case, although the neck of the aneurysm was narrow (2 mm), significant recanalization occurred after the initial occlusion was achieved. This was subsequently treated successfully with flow diversion. This was subsequently treated successfully with flow diversion. Such recanalization is considered one of the less significant complications of using the WEB device, often requiring retreatment with another WEB device, flow diversion, or coiling [14,17]. Factors associated with recanalization include large aneurysm size, wide neck, and incomplete initial occlusion. Asnafi et al. [17] reported retreatment rates of 4% for ruptured aneurysms and 7% for unruptured aneurysms treated with the WEB device, similar to the rates published by van Rooij et al. [15,16]. Although device deployment carries the risks of treatment failure, thromboembolic complications, and retreatment, these risks are still lower compared to other endovascular techniques like coiling [15-18]. On the other hand, angiographic and clinical outcomes after WEB application are promising. Numerous retrospective case series have reported high rates of immediate aneurysm occlusion with endovascular WEB treatment and even higher rates of mid- to long-term occlusion of 70%-96%. Furthermore, good midterm neurological outcomes were achieved in the vast majority of the cases [15-17]. Despite these positive outcomes and advances in endovascular technology, several technical challenges remain. Navigating guidewires and catheters through the tortuous vertebrobasilar system can be difficult, with risks of perforator occlusion or brainstem infarct. Therefore, careful patient selection, accurate device measurements, precise deployment, antiplatelet therapy, and close follow-up are crucial to minimize complications.
Conclusions
The field of endovascular neurointervention is continuously evolving, with new devices and techniques being developed. The use of intrasaccular flow disruptors has the potential to improve angiographic outcomes and reduce complications. However, further prospective studies with larger sample sizes and long-term follow-up are needed to compare the safety and efficacy of different endovascular techniques and to optimize patient outcomes. A multidisciplinary approach involving neurointerventionists, neurosurgeons, and neurologists is essential for optimal patient selection and management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anatomy, head and neck: basilar artery Stat Pearls [Internet] Adigun OO Reddy V Sevensma KE Treasure Island (FL)Stat Pearls Publishing 2023 http://europepmc.org/books/NBK 459137
- 2Vascular geometry of vertebrobasilar tree with and without aneurysm Med Glas (Zenica) EfendićA IsakovićE DelićJ MehiovićA HrustićA 252257112014 https://ljkzedo.ba/sites/default/files/Glasnik/11-02-aug 2014/24.pdf 25082236 · pubmed ↗
- 3Basilar artery fenestration Folia Morphol (Warsz) Dodevski A Lazareska M Tosovska-Lazarova D Zhivadinovik J Stojkoski A 8083702011 https://journals.viamedica.pl/folia_morphologica/article/view/1931021630227 · pubmed ↗
- 4Basilar artery fenestration aneurysm treated with the Woven Endo Bridge device Interdiscip Neurosurg de Almeida Silva JM Dias GM Rezende AL 100936232021 https://www.sciencedirect.com/science/article/pii/S 2214751920304977?via%3Dihub
- 5Cerebral arterial fenestrations Interv Neuroradiol Cooke DL Stout CE Kim WT 2612742020142497608710.15274/INR-2014-10027 PMC 4178766 · doi ↗ · pubmed ↗
- 6Basilar artery fenestration aneurysms: endovascular treatment strategies based on 3D morphology Clin Neuroradiol Trivelato FP Abud DG Nakiri GS de Castro Afonso LH Ulhôa AC Manzato LB Rezende MT 73792620162516469210.1007/s 00062-014-0336-0 · doi ↗ · pubmed ↗
- 7Segmental unfused basilar artery with kissing aneurysms: report of three cases and literature review Acta Neurochir (Wien) Krings T Baccin CE Alvarez H Ozanne A Stracke P Lasjaunias PL 56757414920071751435210.1007/s 00701-007-1118-0 · doi ↗ · pubmed ↗
- 8Endovascular management of basilar artery aneurysms associated with fenestrations Am J Neuroradiol Islak C Kocer N Kantarci F Saatci I Uzma O Canbaz B 958964232002 https://www.ajnr.org/content/23/6/958.short 12063224 PMC 7976902 · pubmed ↗