Small Intestinal Neurofibroma With Atypical 17q11.2 Microdeletions: A Rare Cause of Abdominal Distension
Yating Wang, Chunwei He, Dedong Ma, Leiqi Xu

TL;DR
A rare case of NF1 with a small intestinal tumor caused by a genetic deletion is reported, highlighting the importance of comprehensive diagnosis and treatment.
Contribution
This case expands the known range of NF1 symptoms and emphasizes the role of genetic testing in diagnosing rare gastrointestinal manifestations.
Findings
A 22-year-old male with NF1 presented with abdominal distension due to a small intestinal neurofibroma.
Whole-exome sequencing confirmed a 17q11.2 microdeletion involving the NF1 gene.
Surgical resection led to complete remission, underscoring the need for multidisciplinary management in such cases.
Abstract
Neurofibromatosis Type 1 (NF1) is a rare autosomal dominant disorder caused by mutations or deletions in the NF1 gene, with approximately 5% to 11% of cases specifically attributed to the 17q11.2 microdeletion. While cutaneous manifestations are common, gastrointestinal involvement occurs in 10%‐25% of cases, with symptomatic presentations being exceptionally rare. This report describes an unusual case of NF1 presenting with small intestinal neurofibroma, emphasizing diagnostic challenges and management strategies. A 22‐year‐old male with a 1‐year history of recurrent abdominal distension was admitted. Physical examination revealed pathognomonic features of NF1, including axillary freckling and café‐au‐lait macules. Laboratory tests demonstrated anemia and hypoalbuminemia. Imaging and enteroscopy identified a stenotic ileal lesion with mesenteric lymphadenopathy. Initial biopsy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
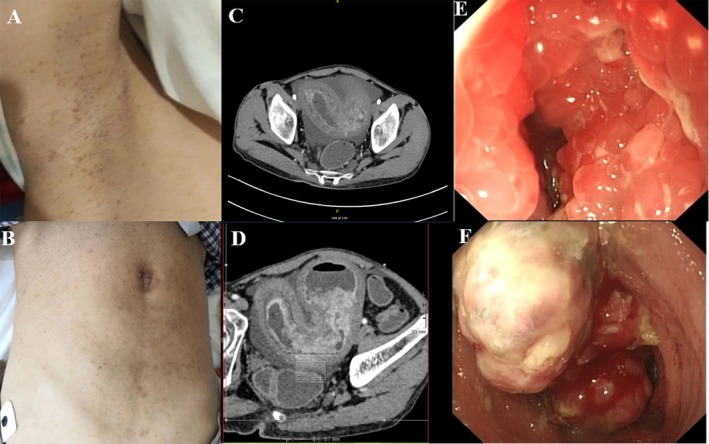 Figure 1
Figure 1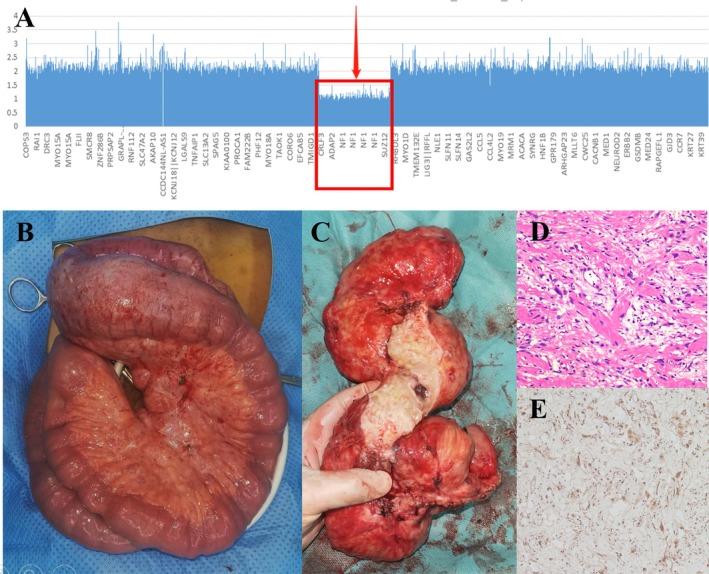 Figure 2
Figure 2- —National Natural Science Foundation of China 10.13039/501100001809
- —Natural Science Foundation of Shandong Province 10.13039/501100007129
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurofibromatosis and Schwannoma Cases · Soft tissue tumor case studies · Gastrointestinal Tumor Research and Treatment
A 22‐year‐old man with a complaint of recurrent abdominal distension for 1 year was admitted to our hospital. He was diagnosed as “ulcerative colitis” by colonoscopy without specific medication. He has no family history. Physical examination revealed freckling at axillary (Figure 1A) and inguinal regions and diffused café‐au‐lait macules on skin (Figure 1B). Laboratory tests showed anemia (hemoglobin 76.0 g/L), fecal occult blood, and hypoalbuminemia (albumin 30.4 g/L).
Abdominal enhanced computed tomography (CT) showed marked thickening and mild enhancement in the ileal mucosa and mesentery with multiple enlarged lymph nodes (Figure 1C,D).
Enteroscopy showed multiple nodular bulges with apparent stenosis in the distal ileum, where the biopsy revealed inflammation (Figure 1E,F).
Laparotomy exploration revealed a 5 × 5 cm mass in the distal ileum with poor mobility and diffused mesenteric lymphadenopathy, of which the biopsy supported neurofibroma. Then, a palliative ileostomy was performed for symptom relief.
Peripheral blood whole‐exome sequencing showed 17q11.2 microdeletions involving the entire region of NF1 and adjacent genes (Figure 2A), atypical microdeletions supporting the diagnosis of Neurofibromatosis Type 1 [1].
Six months later under better self‐conditions, he underwent partial small intestine resection (Figure 2B,C) and ileostomy closure, finally achieving curable excision and functional recovery. The postoperation pathology confirmed the final diagnosis: small intestinal neurofibroma in Neurofibromatosis Type 1 (Figure 2D,E).
Neurofibromatosis Type 1 is a rare hereditary disease, of which only 5% to 11% of patients are caused by the 17q11.2 microdeletions with a more severe phenotype and complications [2]. Currently, the clinical diagnostic criteria for Neurofibromatosis Type 1 are mainly based on the consensus established by the National Institutes of Health (NIH) in 1987 (Table 1). Patients are diagnosed with Neurofibromatosis Type 1 if they have two or more of these features [3]. Our patient met the criteria of 1 and 3, and could be clearly diagnosed with Neurofibromatosis Type 1. Gastrointestinal involvement is present in 10%–25% of Neurofibromatosis Type 1 patients, but less than 5% of patients develop symptoms [4]. Small intestinal neurofibroma is even rarer since the majority of Neurofibromatosis Type 1 patients with intestinal involvement exhibit stromal tumors [5]. Neurofibromas of digestive organs in Neurofibromatosis Type 1 are very scarce, with only a few cases described in the literature (Table 2) [6, 7, 8, 9, 10, 11, 12, 13, 14, 15]. Literature review reveals that the affected sites included stomach, small intestine, mesentery, cecum, appendix, and liver. Abdominal pain is the most common symptom, often combined with gastrointestinal bleeding, perforation, obstruction, and appendiceal diverticula. No patient has gene mutations or deletions. Only one patient is found to have a diffuse mesenteric lesion that could not be completely resected for conservative treatment during surgery, and the treatment method of one patient is unknown while surgical resection is performed in the remaining cases. All cases are diagnosed as neurofibromas on histopathological examination and are benign. For neurofibromas of digestive organs in Neurofibromatosis Type 1, clinical and endoscopic manifestations lack specificity, while treatments remain controversial. Indications for surgery are not clearly defined and are mostly presented in the form of case reports. Surgical resection is seldom needed in most cases as there is limited malignant transformation potential. However, when there is a risk of malignant transformation, obstruction, and bleeding, surgical resection of the neurofibroma is required. According to the size and location of the tumor, local resection of the tumor or partial resection of the involved bowel and intestinal anastomosis are performed. This case expands the spectrum of initial clinical manifestations of Neurofibromatosis Type 1. The possibility of gastrointestinal neurofibroma in Neurofibromatosis Type 1 patients with recurrent abdominal distension should be considered. Physical examination, endoscopy, and radiographic images provide valuable visual information to other clinicians, which contributes to identifying Neurofibromatosis Type 1 at an early stage. Pathological examination and gene sequencing are critical in diagnosis, and surgical treatment should be considered when necessary.
Ethics Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Written informed consent was obtained from the patient for publication of this “Education and Imaging – Gastroenterology.”
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1H. Kehrer‐Sawatzki and D. N. Cooper , “Classification of NF 1 Microdeletions and Its Importance for Establishing Genotype/Phenotype Correlations in Patients With NF 1 Microdeletions,” Human Genetics 140, no. 12 (2021): 1635–1649.34535841 10.1007/s 00439-021-02363-3PMC 8553723 · doi ↗ · pubmed ↗
- 2L. Kluwe , R. Siebert , S. Gesk , et al., “Screening 500 Unselected Neurofibromatosis 1 Patients for Deletions of the NF 1 Gene,” Human Mutation 23, no. 2 (2004): 111–116.14722914 10.1002/humu.10299 · doi ↗ · pubmed ↗
- 3“Neurofibromatosis. Conference statement. National Institutes of Health Consensus Development Conference,” Archives of Neurology 6, no. 12 (1987): 1–7.3128965 · pubmed ↗
- 4G. Cavallaro , U. Basile , A. Polistena , et al., “Surgical Management of Abdominal Manifestations of Type 1 Neurofibromatosis: Experience of a Single Center,” American Surgeon 76, no. 4 (2010): 389–396.20420249 · pubmed ↗
- 5U. Basile , G. Cavallaro , A. Polistena , et al., “Gastrointestinal and Retroperitoneal Manifestations of Type 1 Neurofibromatosis,” Journal of Gastrointestinal Surgery 14, no. 1 (2010): 186–194.19495890 10.1007/s 11605-009-0940-5 · doi ↗ · pubmed ↗
- 6K. Koşucu , A. Ahmetoĝlu , U. Cobanoĝlu , et al., “Mesenteric Involvement in Neurofibromatosis Type 1: CT and MRI Findings in Two Cases,” Abdominal Imaging 28, no. 6 (2003): 822–826, 10.1007/s 00261-003-0040-z.14753598 · doi ↗ · pubmed ↗
- 7J. R. Bakker , M. M. Haber , and F. U. Garcia , “Gastrointestinal Neurofibromatosis: An Unusual Cause of Gastric Outlet Obstruction,” American Surgeon 71, no. 2 (2005): 100–105.16022006 · pubmed ↗
- 8R. Rastogi , “Intra‐Abdominal Manifestations of von Recklinghausen's Neurofibromatosis,” Saudi Journal of Gastroenterology 14, no. 2 (2008): 80–82.19568505 10.4103/1319-3767.39623 PMC 2702901 · doi ↗ · pubmed ↗