Pseudotumor Tensor Fascia Lata Syndrome From Underlying Severe Lumbar Stenosis: A Case Report
Zane Shah, Won J Jeong, Wyatt I Kupperman, Yonghoon Lee

TL;DR
This case report describes a rare condition where a pseudotumor in the tensor fascia lata mimics a soft tissue mass, linked to severe lumbar stenosis and altered gait.
Contribution
The paper presents a new clinical case linking TFL pseudotumor to lumbar stenosis and radiculopathy, highlighting diagnostic challenges.
Findings
Pseudotumor of the tensor fascia lata can mimic a soft tissue tumor and lead to unnecessary oncologic workups.
MRI is the gold standard for diagnosing TFL pseudotumor, with treatment options including hip abductor strengthening and botulinum toxin.
Altered gait mechanics and denervation from lumbar stenosis may contribute to TFL hypertrophy.
Abstract
A pseudotumor of the tensor fascia lata (TFL) describes a rare condition characterized by hypertrophy or pseudohypertrophy of the TFL that can mimic a soft tissue mass. Without the right clinical suspicion, it can be misdiagnosed as a benign or malignant soft tissue tumor, leading to oncologic workups. Unnecessary workups can cause patient distress, waste resources, and delay the management of the condition and its associated symptoms. Here, we describe a 65-year-old male who developed a pseudotumor of the TFL in the setting of severe lumbar spinal stenosis. The etiology for this patient was suspected to be a combination of altered gait mechanics and denervation secondary to L4/5 radiculopathy. There is a paucity of current research, literature, and clinical cases on this topic. However, the prior cases share similarities in presentation and imaging findings. Magnetic resonance imaging…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
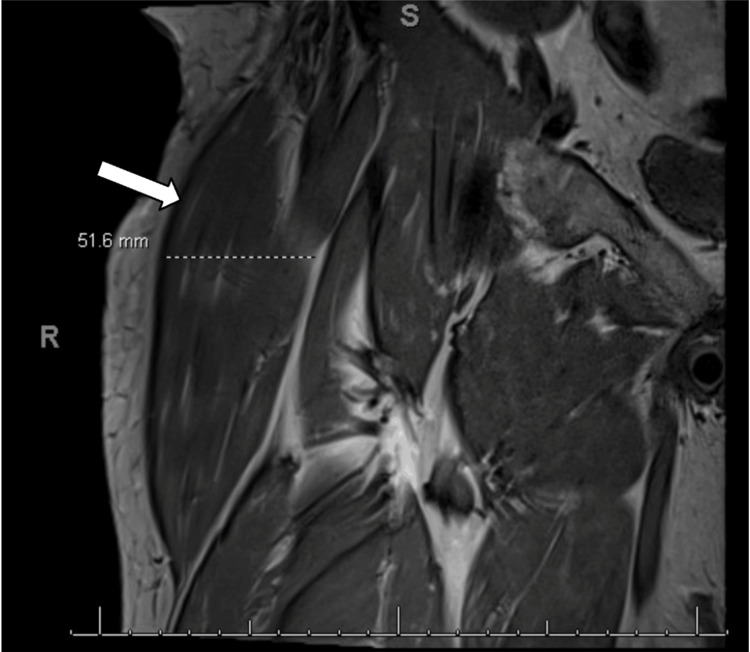 Figure 1
Figure 1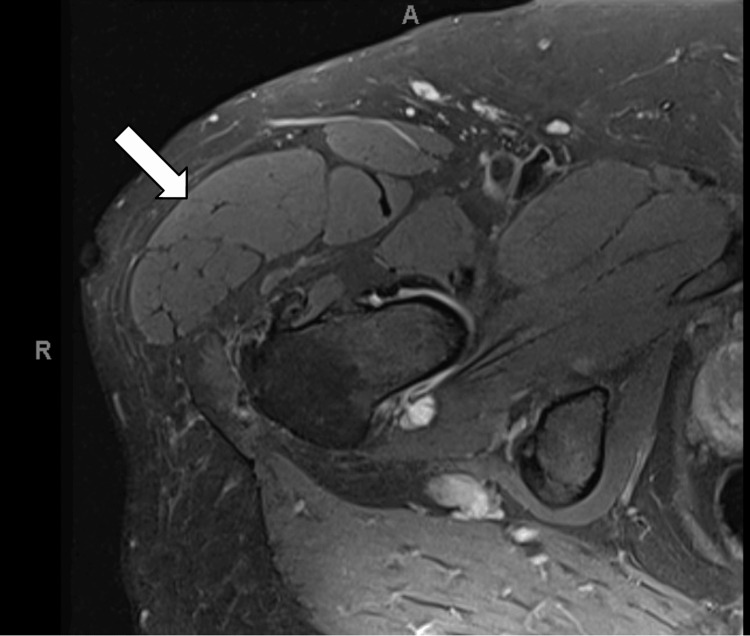 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Nerve Injury and Rehabilitation · Pectus Deformity Diagnosis and Treatment
Introduction
Pseudotumor of the tensor fascia lata (TFL) describes a rare condition characterized by hypertrophy of the TFL that can mimic a soft tissue mass. The etiology is not entirely understood, but two theories are suggested in the literature: mechanical hypertrophy, where altered biomechanics lead to compensatory hypertrophy of the TFL, and denervation hypertrophy, where a muscle unexpectedly enlarges following the loss of innervation [1,2]. Mechanical hypertrophy can result from the overuse of a specific muscle or group of muscles as a result of changes in a patient's gait, while the exact mechanism of denervation hypertrophy is not well understood. On magnetic resonance imaging (MRI), true muscle hypertrophy appears as an isointense enlargement of normal-appearing muscle fibers, while pseudohypertrophy appears as an enlargement of muscle with excessive amounts of fat interspersed throughout the muscle [2]. Without proper clinical suspicion, it can be misdiagnosed as a benign or malignant soft tissue tumor, leading to unnecessary oncologic workups that can cause patient distress and waste resources. Here, we describe a 65-year-old male who developed a pseudotumor of the TFL in the setting of lumbar spinal stenosis. This case adds to the existing knowledge regarding this rare condition, including its etiology, evaluation, and management for appropriate patient care.
Case presentation
A 65-year-old male with a history of diffuse idiopathic skeletal hyperostosis (DISH) and chronic low back pain for many years presented to a Physical Medicine and Rehabilitation (PM&R) clinic with acute-on-chronic right gluteal and sacroiliac joint (SIJ) pain, which had been constant for six months with occasional episodes of worsening pain. The pain was rated as five out of 10 on a Visual Analog Scale. The patient reported that the pain improved with mild physical activity and analgesic medications, such as gabapentin and acetaminophen, but worsened with strenuous or prolonged exertion. He denied any symptoms of neurogenic claudication, motor weakness, bowel and bladder dysfunctions, or saddle anesthesia.
On physical exam, tenderness was noted in the right mid to distal SIJ region, along with decreased lumbar spine and hip range of motion. Strength and sensation in the upper and lower extremities were intact. Various maneuvers, namely Faber, Yeoman’s, and sacral compression tests, were positive. MRI of the lumbar spine showed moderately severe central stenosis at L4-L5 as well as mild and moderately severe bilateral foraminal narrowing at L3-L4 and L4-L5, respectively. The patient was diagnosed with chronic low back pain, likely due to SIJ-referred pain and/or L4/5 radiculopathy, and was treated with physical therapy, a home exercise program, and right L4-L5 transforaminal epidural steroid injections. At follow-up visits, the patient reported symptom improvement with this comprehensive treatment plan.
However, 15 months after the initial consultation, the patient reported new symptoms, including swelling and discomfort in the right lateral gluteal region. Examination revealed a notable palm-sized fullness at the anterior and lateral right greater trochanter region with mild discomfort on palpation. Internal and external rotation of the hip was decreased. Diagnostic ultrasound performed in the clinic revealed a large, well-demarcated soft tissue mass or hypertrophy along the TFL, gluteus medius, and gluteus minimus muscles. The mass appeared more hyperechoic than adipose tissue, with its thickest point measuring approximately 4 cm. This finding prompted further evaluation.
Subsequent MRI of the hip revealed a large TFL with a diameter of up to 5.2 cm, as seen in Figure 1 and Figure 2. The hypertrophied TFL demonstrated homogeneous muscle signal intensity on all sequences without evidence of a discrete mass, abnormal enhancement, necrosis, or infiltrative features, making a soft tissue tumor unlikely. While the etiology of TFL hypertrophy remains uncertain, we hypothesize a potential association with lumbar spinal stenosis radiculopathy based on limited reports in the literature, though the hip MRI alone does not establish this causal relationship. Diagnosed with pseudotumor syndrome of the TFL, the patient underwent ultrasound-guided TFL chemodenervation with 50 units of onabotulinum toxin type A, which significantly improved his symptoms. Follow-up visits confirmed a marked reduction in TFL muscle mass on physical examination along with improved pain; however, the patient continued to experience some residual pain and a sensation of fullness in the right leg. His condition was managed with increased doses of botulinum toxin injections, up to 100 units. At subsequent visits, the patient reported further improvement in pain over the TFL. Given the successful diagnosis and management of the patient's condition and symptoms, we plan to closely monitor the patient for potential further intervention for the pseudotumor syndrome of the TFL and ongoing management of lumbar stenosis.
MRI showing hypertrophy of the TFLThe scan of the right lower extremity in the coronal plane shows an enlarged TFL muscle measuring 51.6 mm as demarcated in the image (white arrow).TFL, tensor fascia lata; MRI, magnetic resonance imaging
MRI showing a cross-section of TFL hypertrophyThe scan of the right lower extremity at the level of the hip in the axial plane shows the enlargement of the TFL muscle (white arrow).TFL, tensor fascia lata; MRI, magnetic resonance imaging
Discussion
We present a case of a 65-year-old male with lower back and hip pain in the setting of lumbar canal and foraminal stenosis, and likely mechanical gluteal dysfunction, who developed pain, swelling, and fullness of the right lateral gluteal region. These symptoms were caused by hypertrophy of the TFL. This case is significant as it adds to the limited body of existing literature describing TFL hypertrophy and its possible etiologies. There is substantial overlap in the clinical presentation of TFL hypertrophy and the more serious diagnosis of sarcoma, with both conditions presenting as an anterolateral thigh mass. Therefore, increasing clinical awareness of the potential diagnosis of TFL hypertrophy or pseudohypertrophy in relevant cases is important.
The etiology of this condition is not entirely clear, but two possible mechanisms suggested in the literature are mechanical and denervation hypertrophy [1]. Mechanically, hypertrophy can follow local muscle tears, hip osteoarthritis, or anterior cruciate ligament tears [3]. Hypertrophy can also present in the setting of gluteus medius and minimus muscle atrophy, potentially as a compensatory mechanism for hip abduction function [3]. Additionally, altered gait and biomechanics following spine or hip surgery can cause the condition. Denervation hypertrophy, on the other hand, occurs when a muscle paradoxically enlarges, rather than atrophies, in response to loss of innervation [2]. This pathology can occur in various scenarios including radiculopathies, peripheral nerve injuries, peripheral neuropathies, and disorders of the anterior horn cells, such as poliomyelitis [4]. In rare instances, TFL pseudohypertrophy has been reported, characterized by fatty and connective tissue infiltration into the muscle belly, rather than true hypertrophy, which involves an increase in muscle fiber volume [5]. The exact mechanisms leading to pseudohypertrophy are not completely understood, and some cases are idiopathic, suggesting the process may be independent of the mechanisms causing true hypertrophy [5]. In our case, TFL hypertrophy was present in the setting of both denervation and mechanical hypertrophy. The denervation was likely related to the patient’s L4 radiculopathy, confirmed by MRI findings of moderately severe foraminal narrowing at the L4-L5 level. The mechanical contribution likely involved altered gait mechanics secondary to back pain, radiculopathy, and gluteal dysfunction.
Limited case reports and series in the literature discuss TFL hypertrophy or pseudohypertrophy, and many describe patients with clinical symptoms or imaging findings similar to those in our case. One existing case written by Shields et al. describes similar US and MRI findings of unilateral TFL muscle hypertrophy to those found in our case [1]. For both Shields's case, as well as another case described by Pereira et al., sarcoma is the suspected diagnosis until MRI imaging points clinicians in the direction of TFL hypertrophy, rather than malignancy, due to muscle enlargement without fatty replacement, edema, or abnormal enhancing masses [1,3]. For TFL hypertrophy, MRI is the gold standard for confirming the diagnosis in nearly all cases [1,3,5-9,10,11]. In our case, we used both diagnostic ultrasound and MRI as diagnostic tools. However, ultrasound as a modality can be highly user-dependent, making MRI the preferred gold standard.
Treatment for TFL hypertrophy often involves physical therapy consisting of stretching and strengthening of the hip abductors, although patients may also benefit from botulinum toxin injections [1]. Strengthening of the hip abductors, namely the gluteus medius and minimus muscles, may help to address the compensatory mechanical causes of TFL hypertrophy in response to weakened overall hip abduction function. In our case, the patient was treated with increasing doses of botulinum toxin, which resulted in a reduction of muscle mass and an improvement in pain symptoms.
Conclusions
A pseudotumor of the TFL is a rare condition characterized by hypertrophy of the TFL, typically presenting as a mass in the anterolateral thigh and accompanied by localized pain. This condition can mimic the presentation of a soft tissue tumor. Clinical assessment and MRI characteristics are crucial for an accurate diagnosis. To limit unnecessary diagnostic testing and invasive procedures, clinicians should be aware of TFL hypertrophy and its possible etiologies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hypertrophy of the tensor fascia lata: a pseudotumor due to lumbar radiculopathy Surg Neurol Int Shields LB Iyer V Bhupalam RC Zhang YP Shields CB 5221220213475457210.25259/SNI_857_2021 PMC 8571211 · doi ↗ · pubmed ↗
- 2Denervation hypertrophy of muscle: MR features J Comput Assist Tomogr Petersilge CA Pathria MN Gentili A Recht MP Resnick D 596600191995762269110.1097/00004728-199507000-00017 · doi ↗ · pubmed ↗
- 3Unilateral hypertrophy of the tensor fascia lata J Belg Soc Radiol Pereira C Toukouki A Kurth W 3210820243852372710.5334/jbsr.3462 PMC 10959137 · doi ↗ · pubmed ↗
- 4Denervation pseudo hypertrophy of the calf: an important cause of lower limb swelling Radiol Case Rep Hynes JP Glynn D Eustace SJ 170217041720223534556510.1016/j.radcr.2022.02.066PMC 8956883 · doi ↗ · pubmed ↗
- 5Unilateral hypertrophy of tensor fascia lata: a case report Cureus Al Gallaf LY Asiri YN Al Dawsari FA Al Adel FI 014202210.7759/cureus.32463 PMC 975023936531789 · doi ↗ · pubmed ↗
- 6Abductor tendon tears are associated with hypertrophy of the tensor fasciae latae muscle Skeletal Radiol Sutter R Kalberer F Binkert CA Graf N Pfirrmann CW Gutzeit A 6276334220132294083710.1007/s 00256-012-1514-2 · doi ↗ · pubmed ↗
- 7Association of tensor fascia lata hypertrophy and fatty infiltration in the presence of abductor tendon tears: a radiographic study J Hip Preserv Surg Quinn M Levins J Mojarrad M 197201820213514571810.1093/jhps/hnab 058PMC 8826352 · doi ↗ · pubmed ↗
- 8Bilateral hypertrophy of the M. tensor fascia latae J Belg Soc Radiol De Clercq C Jans L Verstraete K 4410620223564748310.5334/jbsr.2724 PMC 9104491 · doi ↗ · pubmed ↗