Subdiaphragmatic bronchogenic cysts: Case report and literature review
Matin Vahedi, Ali Motamedi Rad, Elham Nazar, Alireza Samimiat

TL;DR
This paper reports a rare case of a subdiaphragmatic bronchogenic cyst in a 36-year-old man and reviews 24 new cases, highlighting the diagnostic challenges and successful surgical treatment.
Contribution
The paper adds 24 new cases to the literature on subdiaphragmatic bronchogenic cysts and emphasizes the importance of surgical resection for favorable outcomes.
Findings
Subdiaphragmatic bronchogenic cysts are rare and often present with nonspecific symptoms like abdominal pain.
Surgical resection is the optimal treatment, with excellent prognosis and no recurrence observed in the reported case.
The review of 24 new cases reinforces the diagnostic challenges due to the rarity and non-specific clinical features of these cysts.
Abstract
Bronchogenic cysts are rare congenital malformations of the respiratory tract, arising from abnormal budding of the foregut during embryogenesis. Clinical manifestations vary by location and complications, ranging from asymptomatic to causing respiratory distress in newborns or recurrent respiratory issues in adults. Subdiaphragmatic bronchogenic cysts are extremely rare, with only a limited number of case reports published. They often present without symptoms or with nonspecific symptoms such as abdominal pain. Diagnosis typically relies on histopathologic analysis of excised biopsies performed during surgery. Due to their rarity and lack of distinctive clinical features, these cysts pose significant diagnostic challenges. A 36-year-old Iranian man, presented with a 5-month history of abdominal pain. Abdominal sonography revealed a cystic lesion posterior to the liver. An aspiration…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2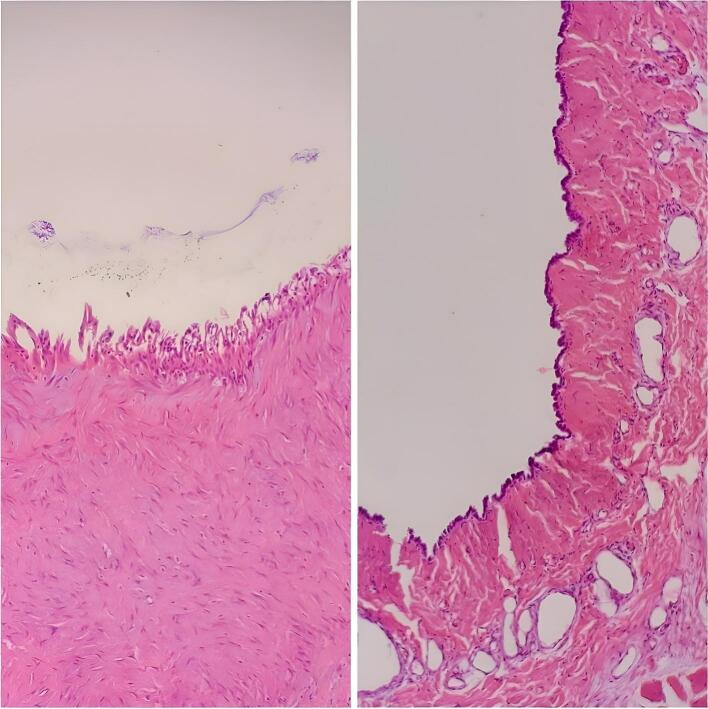 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Congenital Diaphragmatic Hernia Studies · Medical Imaging and Pathology Studies
Background
1
Bronchogenic cysts are uncommon congenital malformations of the respiratory tract, resulting from anomalous budding of the foregut during embryogenesis [1,2]. Although the exact pathogenesis remains unknown; the hypothesis of embryo abscission and translocation is widely accepted. During the early stages of embryo development, the thorax and abdomen cavity become integrated, and the primary tracheobronchial tree forms by the 5th week. Within this critical period, various abnormal germ cells detach and migrate. Due to the inability to discharge secretions effectively, a bronchogenic cyst develops at the site of migration [3]. They can be found in the mediastinum or the lung parenchyma, depending on the stage of embryological development they originate from. Mediastinal cysts arise earlier in development and peripheral ones (lungs) develop later [4].
The clinical manifestations of affected patients vary according to their location and associated complications. Although they can be asymptomatic [5], and discovered incidentally on radiological imaging, they may become symptomatic in infancy or adulthood. In adults, bronchogenic cysts may cause recurrent coughing, wheezing, or pneumonia [6]. In newborns, they may lead to life-threatening conditions, such as respiratory distress, cyanosis, and feeding difficulty [7,8].
On chest radiography, they present as sharp-defined, solitary, round, or oval-shaped masses with water-density opacities. They may have air-fluid levels, due to previous or current infection. The density of lesions in the CT scan varies from water density to high density because of the blood, calcium, or protein content of the fluid in the cysts. MRI is better than a CT scan at determining the anatomical relations of the cysts, their signal intensity on MRI, also depends on the cyst content [9,10].
In gross pathology, they are Spherical, Smooth, White or pinkish, Single or multiple, ranging from 2 to 12 cm in diameter, frequently unilocular, and filled with clear fluid or proteinaceous mucus, and rarely air or hemorrhagic secretions. Calcification of the cyst wall is uncommon, and communication with the bronchial tree is rare [2]. Histologically, the cysts are lined with columnar respiratory epithelium with occasional areas of squamous metaplasia. The wall may contain airway components such as cartilage plates, bronchial glands, and smooth muscle [2].
Due to the potential risk of complications such as infection, rupture, bleeding, and malignant transformation, complete surgical resection even for asymptomatic patients is recommended [11]. Recurrent cyst aspiration may be an option, but due to the high risk of recurrence, it is not widely accepted. The prognosis, after the cyst resection is excellent [12,13].
Subdiaphragmatic bronchogenic cysts are exceptionally rare, and only a limited number of case reports have been published to date. The clinical presentations of subdiaphragmatic bronchogenic cysts are typically nonspecific, primarily attributed to complications such as local compression and infection. Depending on their location that may cause abdominal pain, dysphagia, chest pain, and dyspnea [14]. Due to the absence of specific radiographic features, they may be easily mistaken for other common diseases of the same origin. These cysts pose challenges in preoperative diagnosis due to their lack of distinctive clinical features, as well as inconclusive findings from laboratory tests and imaging. Their rarity further complicates the diagnostic process, necessitating histopathological examination for definitive diagnosis [15].
In this article, we report another rare case of an ectopic bronchogenic cyst in the subdiaphragmatic space. The patient presented with abdominal pain and the pathology report confirmed a bronchogenic cyst. In addition, we conducted a comprehensive review of recent literature concerning subdiaphragmatic bronchogenic cysts. These cases have been reported after the review conducted by Xiao, J et al (Table 1).Table 1. Demographics, clinical symptoms, imaging features, surgical and follow-up information of literature review and our case.Table 1. CaseYearAgeSexSymptomsCyst numberCyst localizationSize (cm)CT featuresPreoperative diagnosisSurgical procedureContent of cystFollow up1202276MAbdominal pain, distention1Lesser gastric curvature3131Well define soft tissue massGastrointestinal stromal tumorLaparoscopyMucoidN/A2202239FUpper abdominal pain1Retroperitoneal space5026Cystic massLymphatic cystLaparoscopyN/AN/A3202246FAbdominal pain1Large curvature4241Uniform massGastrointestinal stromal tumorGastrectomyTurbid fluidN/A4202249FNone1Left adrenal gland5440Moderate density cystLeft adrenal tumorLaparoscopyGelatinous6 m5202240FIntermittent upper abdominal pain1Left inner lobe of liver3216Elliptical low-density cystGallbladder diverticulumLaparoscopyLight yellow turbid fluid6 m6202260MNone1Left upper abdominal quadrant150120120Multifocal cystic massLesser momentum malignancyLaparoscopyViscous mucus1y7202252FNone1Above pancreas3926N/AN/ALaparoscopyN/AN/A8202257FNone1Left adrenal2258Ovoid, well-defined, heterogenousBenign lesionLaparoscopyMucoid6 m9202238FLeft upper abdominal pain1Left suprarenal space632555Well-defined, ovoid, heterogenous lesionN/ALaparoscopyMucoidN/A10202235MNone1Lower left of diaphragm50Well-defined cystLymphangiomaLaparoscopyN/A3 m11202345FUpper abdominal pain1Left upper abdominal quadrant3020Cystic massGastrointestinal stromal tumorLaparoscopyGelatinous and mucoid12 m12202350MN/A1Posterior gastric fundus wall2530Lightly low-density noduleSchwannoma or stromal tumorGastroscopic exertionN/AN/A13202337FNone1Cardia of stomach30Cystic massGastric duplication, foregut cyst or bcLaparoscopyBright yellow fluid9 m14202347MNone1Cardia of stomach50Homogeneous low-density lesionGastric bcLaparoscopyN/A6 m15202337MNone1Posterior wall of the stomach,35Cystic massBcLaparoscopyYellow-brownish liquid3 m16202367MNone1Liver and gastric ligament3136Round, slightly, low-densityGastrointestinal stromal tumorLaparoscopyN/A6 m17202365MBelching, intermittent epigastric pain1Cardia of stomach4030Cystic massN/ALaparoscopyCoffee colored liquid2 m18202341FDiastolic arterial hypertension1Left adrenal5228Heterogeneous massAdrenal massLaparoscopySerousN/A19202354MNone2Left diaphragmatic crura4732Irregular mass shadowN/ALaparoscopyGelatinous2 y20202347MRight chest pain1Posterior wall of stomach8070Elliptical homogeneous massN/ALaparoscopyYellow liquid2 m21202340FNone1Left adrenal555035Mass and cystic lesionAdrenal massN/AGelatinousN/A22202365FN/A1N/AN/AN/AN/AN/AN/AN/A23202448FFrequent urination1Right side of pelvic9957Cystic massOvarian cyst, cystic massLaparoscopyBrown sticky fluidN/A24202418MRecurrent nephrolithiasis, severe left back pain, recurrent abdominal pain1Left suprarenal9669Homogenous, thin walled, well circumscribedAdrenal cyst, gastrointestinal duplication cyst, and adrenal neoplasmLaparoscopyWhite creamy fluidN/ACase202436MUpper abdominal pain1Right sub diaphragm685248Well define cystDiaphragm massLaparotomyBrown turbid fluid6 m
This study has been reported in line with the SCARE criteria [40].
Case presentation
2
A 36-year-old Iranian man presented with the chief complaint of abdominal pain about 5 months ago preferably the upper part of the abdomen. The nature of the pain was vague and occasional and did not spread anywhere. Hematochezia, melena, anorexia, vomiting, nausea, or fever were not present. He had no significant previous medical history or drug history. He was a smoker (30 Pack/year) and alcoholic. Physical examination revealed 129/700 mmHg blood pressure, a temperature of 36.9 °C, and heart and respiratory rates of 80 and 16 per minute, respectively. Examination of the abdomen showed symmetry without any scars. The abdominal assessment revealed no tenderness and no rebound tenderness, and auscultation detected normal intestinal sounds. The complete blood count (CBC) reported white cell and platelet counts of 5.1 × 10^3^/μL and 246 × 103/μL, respectively. Hemoglobin was 16.5 g/dl at admission. The abdominal sonography was done which reported a cystic lesion with a benign appearance with the size of 756530 in the posterior of the liver and lateral to Perirenal space, about 70 cc brownish liquid aspiration was done which was sent for cytology and analysis. The cystic lesion fluid cytology reported an acute inflammatory process (consisting of abscess material), and no malignant cell was seen. Furthermore, an abdominal CT scan W/O contrast was done and a cystic lesion with the size of 685248 in the right sub diaphragm with pressure effect on the right lobe of the liver was reported (Fig. 1).Fig. 1. Abdominal CT scan W/O contrast was done which a cystic lesion with the size of 685248 in the right sub diaphragm.Fig. 1
A laparotomy plan was considered for the patient. The mass was completely removed after being freed from the adhesion of the surrounding tissues and it was sent for pathology evaluation. (Fig. 2). Pathological assessment of the extracted tissue pointed to a Benign cystic lesion lined by flat to low columnar epithelial cells and a variable number of goblet cells overlying the congested fibromuscular wall, compatible with bronchogenic cyst (Fig. 3). A three-day hospital discharge followed the patient's uneventful recovery. We performed follow-ups for the patient at the hospital outpatient department at 3-month intervals. The follow-up after 6 months showed that the patient had no signs of recurrence.Fig. 2. Sub diaphragmatic cystic mass completely surgically removed.Fig. 2. Fig. 3Histopathologic examination showed cystic lesion lined by flat and columnar epithelial cells and variable numbers of goblet cells (H&E X400).Fig. 3
Discussion
3
Bronchogenic cysts are rare congenital abnormalities that originate during embryogenesis. While the thorax and mediastinum are their typical locations, they occasionally manifest in the subdiaphragmatic space [[1], [2], [3]]. In the most recent review article, approximately 100 cases of subdiaphragmatic bronchogenic cysts were identified in the English literature [15]. This article contributes an additional 24 cases, sourced from 21 articles and letters published between April 2022 and April 2024 [14,[16], [17], [18], [19], [20], [21], [22], [23], [24], [25], [26], [27], [28], [29], [30], [31], [32], [33], [34], [35]]. Furthermore, we present a case from our own institution.
Although rare instances of subdiaphragmatic bronchogenic cysts (sBCs) have been discovered during pregnancy and childhood [7,8,36]. The majority of cases in this review were individuals between 40 and 60 years old, which is consistent with the previous review. Regarding gender distribution, the number of male cases slightly exceeds that of females, mirroring the findings of the last review [15].
Except for one case [32], all other cysts were solitary. The outlier was a 54-year-old male, referenced in a Chinese letter, who simultaneously had a mediastinal bronchogenic cyst (BC) and a subdiaphragmatic bronchogenic cyst (sBC). There was another unusual case in previous literature where multiple cysts were present, either unilaterally or bilaterally, on the same side or both sides of the diaphragm.
Cyst sizes varied from 2.0 cm to 15.0 cm, with the majority ranging between 3.0 cm and 5.0 cm, according to the data available in this review. It has been reported that subdiaphragmatic bronchogenic cysts (sBCs) are most commonly found within the size range of 3 cm to 7 cm. The majority of the cysts were located in the left upper abdominal cavity and left retroperitoneal space, in close proximity to the left adrenal gland and pancreas, and around the gastric wall. There was a unique case where an sBC was discovered in the left inner lobe of the liver, a finding that was reported for the first time [20].
A significant number of cases were asymptomatic, while others presented with nonspecific symptoms such as intermittent abdominal pain. Subdiaphragmatic bronchogenic cysts (sBCs) may become symptomatic due to compression at the location or infection. One case exhibited diastolic hypertension, likely due to the cyst's compressive effect on the renal artery [31]. Another case involved an intestinal bronchogenic cyst (BC) that led to frequent urination due to bladder compression [34]. A case reported in the previous review presented with hypertension [37], and another case became symptomatic due to a cyst infection [15].
In most instances, laboratory findings and tumor markers do not contribute significantly to the diagnosis as they are predominantly negative. However, there are rare instances where tumor markers such as CA19–9, CEA, AFP, CA47–7, and CA72–4 have tested positive [21,22,26,28,33,34]. Nonetheless, only one case exhibited malignant changes following surgical biopsy [21].
Imaging studies often do not provide definitive diagnostic information due to their nonspecific findings. Our review, consistent with previous studies, has determined that the density of sBC on CT scans can vary from low to high, with or without enhancement. Additionally, other imaging modalities such as ultrasound (US), endoscopic ultrasound (EUS), and MRI have not proven helpful in diagnosis.
Histopathological findings are crucial for diagnosis. All cysts examined exhibited column-ciliated epithelium. Additionally, cartilage, smooth muscle, and bronchial glands were observed. Only two cases underwent biopsy before surgery [28]. Given that the majority of sBCs are benign, a biopsy could potentially obviate the need for surgery, although those two cases terminated to surgery too. However, it should be noted that biopsies may not always be diagnostic due to issues related to sampling [38]. In the reviewed literature, all cases underwent surgical intervention, with the majority being performed via retroperitoneal laparoscopy.
Despite preoperative studies indicating that sBC is a benign lesion, predicting the likelihood of malignancy remains challenging. Additionally, some cases presented with symptoms, and patients were discharged promptly following surgery. Therefore, surgery continues to be the preferred treatment option.
Following resection, all reviewed cases demonstrated no recurrence. In the most recent review, only one case of malignancy recurred 14 months post-surgery. Thus, patients with sBC generally had a favorable prognosis [39].
Conclusion
4
We have added 24 additional cases to the previously reviewed article. Combined with the earlier findings, it is evident that sBC is a benign lesion predominantly occurring in the left adrenal or pancreatic space. Most patients are asymptomatic; however, due to the favorable prognosis following resection surgery, it remains the optimal management strategy.
Author contribution
MV conceived the study. AS and AM contributed to the case collection, discussion, literature review, and first manuscript draft. MV, AS and AM provided critical revisions. All authors contributed to the article and approved the submitted version.
Consent for publication
Written informed consent was obtained from the patient to publish this case report and accompanying images. On request, a copy of the written consent is available for review by the Editor-in-Chief of this journal.
Ethics approval and consent to participate
Ethical review and approval were not required for the study on human participants in accordance with the local legislation and institutional requirements. The ethics committee waived the requirement of written informed consent for participation.
Guarantor
Alireza Samimiat.
Research registration number
Not applicable.
Funding
We do not have any financial support for this study.
Declaration of competing interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Berrocal T.Madrid C.Novo S.Gutiérrez J.Arjonilla A.Gómez-León N.Congenital anomalies of the tracheobronchial tree, lung, and mediastinum: embryology, radiology, and pathology Radio Graphics 2412004 Jane 171461024510.1148/rg.e 17 · doi ↗ · pubmed ↗
- 2Rodgers B.M.Harman P.K.Johnson A.M.Bronchopulmonary foregut malformations The spectrum of anomalies. Ann. Surg.20351986 May 517524370723010.1097/00000658-198605000-00011 PMC 1251159 · doi ↗ · pubmed ↗
- 3Govaerts K.Van Eyken P.Verswijvel G.Van der Speeten K.A bronchogenic cyst, presenting as a retroperitoneal cystic mass Rare Tumors 412012 Mar 20374410.4081/rt.2012.e 13PMC 332574022532911 · doi ↗ · pubmed ↗
- 4Limaïem F, Ayadi-Kaddour A, Djilani H, Kilani T, El Mezni F. Pulmonary and mediastinal bronchogenic cysts: a clinicopathologic study of 33 cases. Lung 2008;186(1):55–61. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18064522.10.1007/s 00408-007-9056-418064522 · doi ↗ · pubmed ↗
- 5Bolton J.W.Shahian D.M.Asymptomatic bronchogenic cysts: what is the best management?Ann. Thorac. Surg.5361992 Jun 11341137159614610.1016/0003-4975(92)90412-w · doi ↗ · pubmed ↗
- 6Patel S.R.Meeker D.P.Biscotti C.V.Kirby T.J.Rice T.W.Presentation and management of bronchogenic cysts in the adult Chest 10611994 Jul 7985802032410.1378/chest.106.1.79 · doi ↗ · pubmed ↗
- 7Cohn J.E.Rethy K.Prasad R.Mae Pascasio J.Annunzio K.Zwillenberg S.Pediatric bronchogenic cysts: a case series of six patients highlighting diagnosis and management J. Investig. Surg.3362020 Jul 25685733043088610.1080/08941939.2018.1527419 · doi ↗ · pubmed ↗
- 8Jiang J.H.Yen S.L.Lee S.Y.Chuang J.H.Differences in the distribution and presentation of bronchogenic cysts between adults and children J. Pediatr. Surg.5032015 Mar 3994012574669610.1016/j.jpedsurg.2014.06.008 · doi ↗ · pubmed ↗