Immune checkpoint inhibitor-induced dyshidrotic eczema following tremelimumab therapy for hepatocellular carcinoma
Raphaella Lambert, Scott Stratman, Grace Rabinowitz, Hannah Verma, Jonas A. Adalsteinsson, George Niedt, Benjamin Ungar, Nicholas Gulati

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1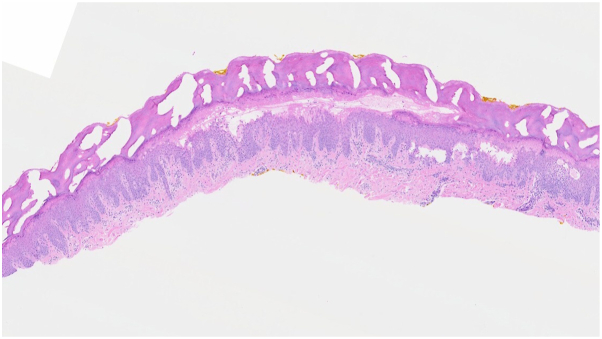 Figure 2
Figure 2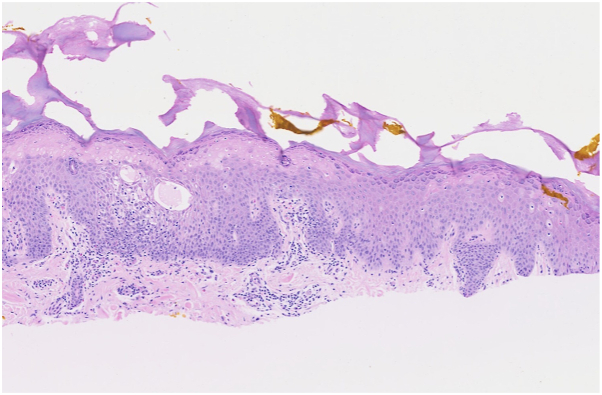 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Melanoma and MAPK Pathways · Colorectal Cancer Treatments and Studies
Introduction
Tremelimumab is an anti-cytotoxic T-lymphocyte–associated antigen-4 (CTLA-4) monoclonal antibody within the category of antineoplastic therapeutics known as immune checkpoint inhibitors (ICIs).1 Tremelimumab is approved for the management of hepatocellular carcinoma and non-small cell lung cancer when used in conjunction with durvalumab, an ICI and programmed death ligand 1 monoclonal antibody.1 ICIs are used in the management of numerous solid and hematologic malignancies; however, such therapies are associated with cutaneous immune-related adverse events (cirAEs) including eczema, pruritus, psoriasis, vitiligo, bullous pemphigoid, and lichenoid eruptions.2^,^3 These reactions may vary in timing, presentation and severity, although they often require acute dermatologic evaluation.2^,^3
Eczematous reactions have been observed in patients treated with various ICIs, including pembrolizumab, ipilimumab, nivolumab, and durvalumab.2^,^3 Literature characterizing the cutaneous reactions induced by tremelimumab is limited.4^,^5 We report a case of dyshidrotic eczema induced by tremelimumab use.
Case report
A 67-year-old man with a previous medical history of well-controlled HIV on bictegravir, emtricitabine, and tenofovir alafenamide, nonalcoholic steatohepatitis, and recurrent, metastatic hepatocellular carcinoma presented for evaluation of a pruritic, blistering rash involving the palms. The patient was diagnosed with hepatocellular carcinoma 4 years prior during routine nonalcoholic steatohepatitis screening and was treated with transarterial chemoembolization and radiofrequency ablation with good initial therapeutic response. Given subsequent progression of disease with metastasis to the left adrenal gland, he began immunotherapy with durvalumab 1500 mg every 4 weeks, with plan to add a single dose of tremelimumab 300 mg. The patient received his first durvalumab infusion without complication. Several days after his second durvalumab and first tremelimumab infusion, he experienced progressive symptoms of rash on the palms, believed to be secondary to tremelimumab infusion. Examination revealed clear, fluid-filled vesicles on the bilateral palms (Fig 1).Fig 1. Vesicular palmar rash.
Shave biopsy of a vesicle from the left second digit revealed spongiotic dermatitis with eosinophils. Microscopic evaluation was notable for superficial necrosis of the epidermis, epidermal acanthosis, intercellular edema, and a perivascular mononuclear infiltrate within the dermis (Figs 2 and 3).Fig 2. Diffusely acanthotic epidermis with intense spongiosis, intercellular edema, and vesicle formation, with underlying perivascular inflammation.Fig 3. Intercellular edema, spongiotic vesicles, and scattered eosinophils.
Clinicopathologic correlation was consistent with dyshidrotic eczema; upon questioning, the patient denied any excessive hand washing or exposure to irritants. As such, irritant contact dermatitis was clinically excluded. Treatment with triamcinolone 0.1% topical ointment twice daily led to resolution of the rash within 2 weeks. The patient has continued durvalumab infusions without issue.
Discussion
ICIs cause upregulation of the immune response, leading to cirAEs.2^,^3 CirAEs occur in up to 68% of patients treated with ICIs, with most reactions being pruritic and those that are non-specific in nature.2^,^6 Although less common, eczematous reactions in the setting of ICIs are most often observed as scaly macules and papules but can range from localized patches and plaques to nummular plaques and asteatotic eczema.7 Reports of dyshidrotic vesicles or morphologies are limited.7 Although clinical presentation of cirAEs can be nonspecific, most rashes are low grade (Common Terminology Criteria for Adverse Events Grade 1-2) and occur mainly on the trunk, with less frequent involvement of the extremities, digits, or face.2 Lesions typically appear after the first few ICI treatments, with rashes caused by anti-CTLA-4 agents often appearing sooner than those caused by anti-PD-1 agents (5 weeks with anti-PD-1 vs 3-4 weeks with anti-CTLA-4 antibodies).2 Eczematous reactions are histopathologically defined by spongiotic dermatitis with sparse to abundant eosinophils and perivascular T-lymphocyte infiltrate,2 consistent with the present case. Such eruptions are often self-limited, with good response to oral antihistamines and topical steroids in most patients. Cessation of ICI treatment is rarely required; some literature suggests that development of cirAEs may portend better prognostic outcome.7 However, clinical severity of cirAEs must be thoroughly evaluated, as systemic corticosteroids or biologic agents may be warranted for severe, persistent reactions. Further, clinicopathologic and laboratory evaluation may be necessary to rule out life-threatening cutaneous reactions including Stevens-Johnson syndrome, toxic epidermal necrolysis, or drug reaction with eosinophilia and systemic symptoms.2^,^7
Other cirAEs observed in the setting of programmed death ligand 1 inhibitor therapy, including durvalumab, have included vasculitis, dermatomyositis, lupus erythematosus-like eruptions, acneiform eruptions, lichenoid eruptions, psoriasiform eruptions, and bullous pemphigoid.7 Literature characterizing cirAEs resulting from tremelimumab therapy is limited. A single center, retrospective review of 17 patients treated with tremelimumab with resultant cirAEs observed pruritus (12/17), eczematous dermatitis (8/17), morbilliform rash (5/17), vitiligo (2/17), xerosis (3/17), acneiform rash (2/17), and psoriasiform dermatitis (1/17) among their cohort.4 None of the patients with eczematous dermatitis were noted to have a vesicular appearance consistent with dyshidrotic eczema.4 Six of the 17 patients were being treated with additional ICIs during the course of their tremelimumab therapy, including 4 concurrently receiving durvalumab.4 The average time to cirAE onset was 15 weeks, with an average of 54 weeks to clearance among patients with eczematous reactions.4 Only one patient required cessation of tremelimumab therapy given the severity of their rash.4
Identifying the causative agent behind cirAEs in the setting of multiple immunotherapies presents a diagnostic challenge.4 Given the resumption of this patient’s durvalumab treatment without continuation of rash, tremelimumab was favored as the trigger. Despite this, an important limitation of this case is the absence of a tremelimumab rechallenge; however, tremelimumab was intended as a single dose. The mechanisms underlying cirAE development secondary to CTLA-4 agents are incompletely understood, although research suggests some cirAEs may be related to the loss of T-cell tolerance.4^,^8 Such as other CTLA-4 agents including ipilimumab, tremelimumab induces T-cell proliferation to increase autoimmune tumor response. Tremelimumab is an IgG2 antibody and ipilimumab is an IgG1 antibody, with research suggesting that IgG2 antibodies result in less complement activation and less complement-dependent cytotoxicity as compared with IgG1 antibodies.4 Thus, IgG2 antibodies such as tremelimumab may lower the risk of cytokine-release syndrome, which should theoretically lead to fewer cirAEs, but may also decrease tremelimumab’s antineoplastic efficacy.4
With many cancer treatment paradigms favoring immunotherapies, dermatologists must be aware of the variety of cirAEs that may occur as well as their management. Literature on dyshidrotic eczematous reactions in the setting of immunotherapy is scarce. We highlight this case to add to the list of possible programmed death ligand 1 and CTLA-4 inhibitor cirAEs, and to improve both provider recognition of these reactions as well as patient outcomes.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tremelimumab Liver Tox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]2012 National Institute of Diabetes and Digestive and Kidney Diseases Bethesda (MD)Published online January 15, 2023 https://pubmed.ncbi.nlm.nih.gov/36795905/
- 2Sibaud V.Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy Am J Clin Dermatol 193201834536110.1007/s 40257-017-0336-329256113 · doi ↗ · pubmed ↗
- 3Le T.K.Brown I.Goldberg R.Cutaneous toxicities associated with immune checkpoint inhibitors: an observational, pharmacovigilance study J Invest Dermatol 14211202228962908.e 410.1016/j.jid.2022.04.02035605659 PMC 10796162 · doi ↗ · pubmed ↗
- 4Welborn M.Kubicki S.L.Garg N.Patel A.B.Retrospective chart review of cutaneous adverse events associated with tremelimumab in 17 patients Am J Clin Dermatol 196201889990510.1007/s 40257-018-0376-330073495 · doi ↗ · pubmed ↗
- 5Frey C.Etminan M.Adverse events of PD-1, PD-L 1, CTLA-4, and LAG-3 immune checkpoint inhibitors: an analysis of the FDA adverse events database Antibodies (Basel)13320245910.3390/antib 1303005939051335 PMC 11270294 · doi ↗ · pubmed ↗
- 6Curry J.L.Tetzlaff M.T.Nagarajan P.Diverse types of dermatologic toxicities from immune checkpoint blockade therapy J Cutan Pathol 442201715817610.1111/cup.1285827859479 · doi ↗ · pubmed ↗
- 7Coleman E.Ko C.Dai F.Tomayko M.M.Kluger H.Leventhal J.S.Inflammatory eruptions associated with immune checkpoint inhibitor therapy: a single-institution retrospective analysis with stratification of reactions by toxicity and implications for management J Am Acad Dermatol 804201999099710.1016/j.jaad.2018.10.06230399387 PMC 6420863 · doi ↗ · pubmed ↗
- 8Quach H.T.Johnson D.B.Le Boeuf N.R.Zwerner J.P.Dewan A.K.Cutaneous adverse events caused by immune checkpoint inhibitors J Am Acad Dermatol 854202195696610.1016/j.jaad.2020.09.05434332798 · doi ↗ · pubmed ↗