Assessment of Adherence to Consolidated Standards of Reporting Trials 2010 Guidelines of Randomized Controlled Trials Published in an Indian and International Pharmacology Journal From 2019 to 2023
Jitendra H Hotwani, Pankaj U Mahadkar, Ankita A Rao

TL;DR
This study compares how well Indian and international pharmacology journals followed reporting standards for clinical trials from 2019 to 2023.
Contribution
The study provides a comparative analysis of CONSORT guideline adherence in RCTs published in Indian versus international pharmacology journals.
Findings
International journals showed higher adherence to CONSORT guidelines than Indian journals.
Suboptimal overall reporting was observed in both journals.
Significant differences were found in trial design description and harm reporting.
Abstract
Randomized controlled trials (RCTs) are considered the gold standard in clinical research, providing the highest level of evidence for the effectiveness of healthcare interventions. However, the validity and utility of RCTs depend on the quality of their design, conduct, and reporting. The purpose of this review was to assess the adherence of RCTs published in Indian and international pharmacology journals to the Consolidated Standards of Reporting Trials (CONSORT) statement. RCTs published from 2019 to 2023 from one Indian and one international pharmacology journal were assessed using the CONSORT 2010 checklist, and the items were assigned as "present" or "absent." Data was analyzed using descriptive statistics, and chi-square and Fisher’s exact tests were used for categorical data. A total of 61 articles were analyzed, out of which 31 and 30 articles belonged to international and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
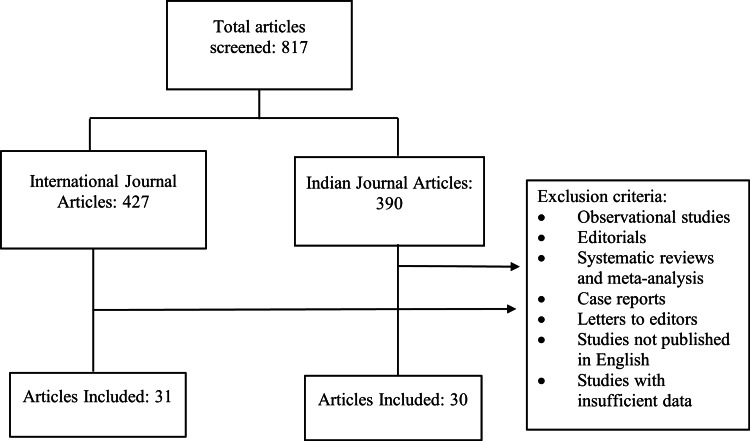 Figure 1
Figure 1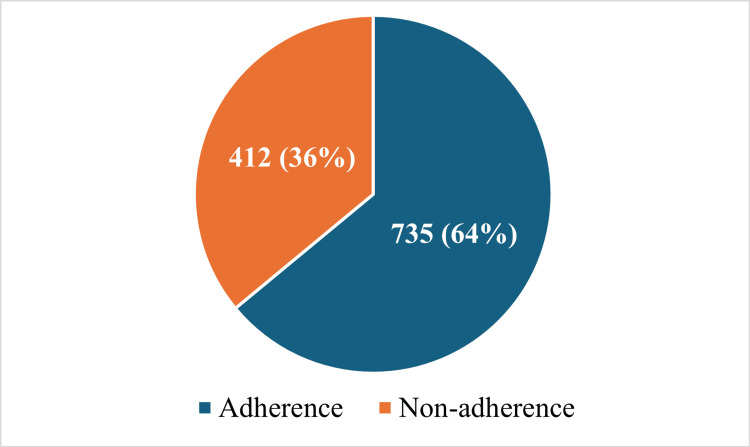 Figure 2
Figure 2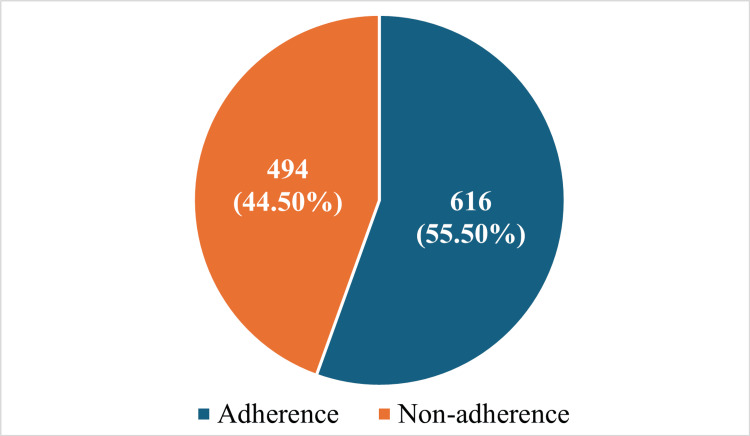 Figure 3
Figure 3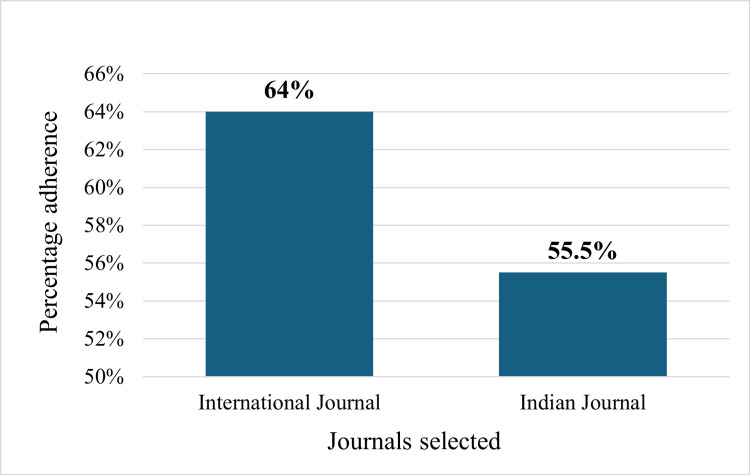 Figure 4
Figure 4| BMC journal (international journal) n = 31 | IJP | Calculated using chi-square test and Fisher’s exact test | ||||
| Checklist items | Item present | Item absent | Item present | Item absent | p-value < 0.05 is significant | |
| 1a | Identification as a randomized trial in the title | 19 (61.3%) | 12 (38.7%) | 21 (70%) | 9 (30%) | p > 0.05 |
| 1b | Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts) | 31 (100%) | 0 (0%) | 29 (96.6%) | 1 (3.4%) | p > 0.05 |
| 2a | Scientific background and explanation of rationale | 27 (87%) | 4 (13%) | 30 (100%) | 0 (0%) | p > 0.05 |
| 2b | Specific objectives or hypotheses | 31 (100%) | 0 (0%) | 30 (100%) | 0 (0%) | p > 0.05 |
| 3a | Description of trial design (such as parallel, factorial) including allocation ratio | 31 (100%) | 0 (0%) | 23 (76.6%) | 7 (23.3%) | p < 0.05* |
| 3b | Important changes to methods after trial commencement (such as eligibility criteria), with reasons | 5 (16%) | 26 (84%) | 0 (0%) | 30 (100%) | p > 0.05 |
| 4a | Eligibility criteria for participants | 31 (100%) | 0 (0%) | 30 (100%) | 0 (0%) | p > 0.05 |
| 4b | Settings and locations where the data were collected | 25 (80.6%) | 6 (19.4%) | 28 (93.3%) | 2 (6.7%) | p > 0.05 |
| 5 | The interventions for each group with sufficient details to allow replication, including how and when they were actually administered | 31 (100%) | 0 (0%) | 25 (83.3%) | 5 (16.7%) | p < 0.05* |
| 6a | Completely defined pre-specified primary and secondary outcome measures, including how and when they were assessed | 7 (22.5%) | 24 (77.5%) | 8 (26.6%) | 22 (73.4%) | p > 0.05 |
| 6b | Any changes to trial outcomes after the trial commenced, with reasons | 3 (9.6%) | 28 (90.4%) | 0 (0%) | 30 (100%) | p > 0.05 |
| 7a | How sample size was determined | 20 (64.5%) | 11 (35.5%) | 13 (43.4%) | 17 (56.7%) | p > 0.05 |
| 7b | When applicable, explanation of any interim analyses and stopping guidelines | 2 (6.5%) | 29 (93.5%) | 0 (0%) | 30 (100%) | p > 0.05 |
| 8a | Method used to generate the random allocation sequence | 22 (70.9%) | 9 (29.1%) | 23 (76.7%) | 7 (23.3%) | p > 0.05 |
| 8b | Type of randomization; details of any restriction (such as blocking and block size) | 24 (77.4%) | 7 (22.6%) | 17 (56.7%) | 13 (43.4%) | p > 0.05 |
| 9 | Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned | 15 (48.4%) | 16 (51.6%) | 12 (40%) | 18 (60%) | p > 0.05 |
| 10 | Who generated the random allocation sequence, who enrolled participants, and who assigned participants to interventions | 11 (35.5%) | 20 (64.5%) | 7 (23.3%) | 23 (76.7%) | p > 0.05 |
| 11a | If done, who was blinded after assignment to interventions (for example, participants, care providers, those assessing outcomes) and how | 14 (45.1%) | 17 (54.9%) | 11 (36.7%) | 19 (63.3%) | p > 0.05 |
| 11b | If relevant, description of the similarity of interventions | 15 (48.4%) | 16 (51.6%) | 0 (0%) | 30 (100%) | p < 0.05* |
| 12a | Statistical methods used to compare groups for primary and secondary outcomes | 28 (90.3%) | 3 (9.7%) | 3 (10%) | 27 (90%) | p < 0.05* |
| 12b | Methods for additional analyses, such as subgroup analyses and adjusted analyses | 7 (22.5%) | 24 (22.5%) | 19 (63.3%) | 11 (36.7%) | p < 0.05* |
| 13a | For each group, the numbers of participants who were randomly assigned, received intended treatment, and were analyzed for the primary outcome | 30 (96.7%) | 1 (3.3%) | 19 (63.3%) | 11 (36.7%) | p < 0.05* |
| 13b | For each group, losses and exclusions after randomization, together with reasons | 20 (64.5%) | 11 (35.5%) | 20 (66.7%) | 10 (33.4%) | p > 0.05 |
| 14a | Dates defining the periods of recruitment and follow-up | 11 (35.5%) | 20 (65.5%) | 23 (76.6%) | 7 (23.3%) | p < 0.05* |
| 14b | Why the trial ended or was stopped | 3 (9.7%) | 28 (90.3%) | 0 (0%) | 30 (100%) | p > 0.05 |
| 15 | A table showing baseline demographic and clinical characteristics for each group | 26 (83.9%) | 5 (16.1%) | 26 (86.7%) | 4 (13.3%) | p > 0.05 |
| 16 | For each group, number of participants (denominator) included in each analysis and whether the analysis was by original assigned groups | 31 (100%) | 0 (0%) | 28 (93.3%) | 2 (6.7%) | p > 0.05 |
| 17a | For each primary and secondary outcome, results for each group, and the estimated effect size and its precision (such as 95% confidence interval) | 31 (100%) | 0 (0%) | 27 (90%) | 3 (10%) | p > 0.05 |
| 17b | For binary outcomes, presentation of both absolute and relative effect sizes is recommended | 2 (6.4%) | 29 (93.6%) | 0 (0%) | 30 (100%) | p > 0.05 |
| 18 | Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing pre-specified from exploratory | 6 (19.4%) | 25 (80.6%) | 24 (80%) | 6 (20%) | p < 0.05* |
| 19 | All-important harms or unintended effects in each group (for specific guidance see CONSORT for harms) | 27 (87%) | 4 (13%) | 8 (26.7%) | 22 (73.3%) | p < 0.05* |
| 20 | Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses | 24 (77.5%) | 7 (22.5%) | 7 (23.3%) | 23 (76.6%) | p < 0.05* |
| 21 | Generalizability (external validity, applicability) of the trial findings | 30 (96.7%) | 1 (3.3%) | 30 (100%) | 0 (0%) | p > 0.05 |
| 22 | Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence | 31 (100%) | 0 (0%) | 30 (100%) | 0 (0%) | p > 0.05 |
| 23 | Registration number and name of trial registry | 31 (100%) | 0 (0%) | 15 (50%) | 15 (50%) | p < 0.05* |
| 24 | Where the full trial protocol can be accessed, if available | 2 (6.5%) | 29 (93.5%) | 0 (0%) | 30 (100%) | p > 0.05 |
| 25 | Sources of funding and other support (such as supply of drugs), role of funders | 31 (100%) | 0 (0%) | 30 (100%) | 0 (0%) | p > 0.05 |
| Total | 735 (64%) | 412 (36%) | 616 (55.5%) | 494 (44.5%) | p < 0.05* | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Systems, Economic Evaluations, Quality of Life · Medication Adherence and Compliance · Meta-analysis and systematic reviews
Introduction and background
Carefully designed clinical trials and observational studies are crucial for providing the necessary information that enables clinicians to modify or adjust treatments effectively. The primary mode of communication among practicing physicians is peer-reviewed publication. Hence, it is important that the quality of such publications be maximized [1]. Randomized controlled trials (RCTs) are considered the gold standard in clinical research, providing the highest level of evidence for the effectiveness of healthcare interventions [2-4]. However, the validity and utility of RCTs depend on the quality of their design, conduct, and reporting [5]. Inadequate reporting can lead to biased results, reducing the reliability of the findings and potentially leading to incorrect clinical decisions [6]. The Consolidated Standards of Reporting Trials (CONSORT) statement, updated in 2010, describes guidelines for transparent and thorough reporting of RCTs, aiming to strengthen the reliability and quality of published trial reports [5]. Adherence to CONSORT guidelines ensures comprehensive documentation of trial methodology, conduct, and outcomes, facilitating accurate interpretation and replication of research findings [2].
In 1996, to improve clinical trial reporting, the CONSORT statement was developed. Since its inception, there have been significant updates in 2001 and 2010 [3,5]. The CONSORT 2010 guidelines provide a checklist of 25 items that should be included in the report of an RCT, covering aspects such as title and abstract, introduction, methods, results, discussion, and other information [2,5,7]. Strict compliance with the checklist items enhances the clarity, completeness, and transparency of reporting. Precise descriptions, nonambiguity, or omission best serve the interests of all readers [5].
Despite the widespread endorsement of the CONSORT guidelines by medical journals, adherence to these guidelines remains suboptimal [6]. Previous studies have shown that the reporting quality of RCTs varies widely across different journals and countries [8]. Evidence suggests that reports of low-quality RCTs as compared with higher-quality ones overestimate the effectiveness of interventions by about 30% across a variety of healthcare conditions [2,5]. RCTs that do not follow CONSORT guidelines while reporting yield unreliable and unpredictable results [9]. Readers of scientific literature deserve to know that editors, reviewers, and authors have adopted processes that foster clarity and replication [10].
This review aims to assess the adherence of RCTs published in Indian and international journals from 2019 to 2023 to CONSORT 2010 guidelines. The comparison with international journals will provide insights into the global trends and potential areas for improvement in the reporting of RCTs. Furthermore, investigating CONSORT adherence in both Indian and international journals allows for a comparative analysis that can reveal disparities and similarities in reporting practices across different research landscapes.
This article was previously presented as a poster at the 2024 Swaasthik Medical Conference on October 25, 2024.
Review
Materials and methods
Research Design, Setting, and Approval
A cross-sectional, observational research project was conducted in the Department of Pharmacology, Topiwala National Medical College and B. Y. L. Nair Charitable Hospital, Mumbai, India, for a period of nine months, starting from May 2024 to January 2025. As there is no involvement of human or animal subjects in our review, ethics committee approval was not sought.
Selection Criteria
We selected two PUBMED-indexed pharmacology journals with comparable high-impact factors using Thomson Reuters journal citation reports 2022 [11], which were 2.4 and 2.9 for one Indian and one international journal, i.e., Indian Journal of Pharmacology (IJP) and Biomed Central Pharmacology and Toxicology (BMC), respectively. RCTs published in both these journals from 2019 to 2023 were selected.
Inclusion Criteria
We included published articles in which the research design was described as random, randomly allocated, randomized, or randomization.
Exclusion Criteria
Non-RCT research designs (e.g., observational studies, editorials, systematic reviews and meta-analyses, case reports, and letters to editors), studies not published in English, and studies with insufficient data for assessment were excluded.
Data Evaluation
Two reviewers received training on assessing RCTs based on the CONSORT 2010 guidelines. They independently extracted data from all selected studies, and any discrepancies were resolved through in-depth discussion. The articles were reviewed by two authors (PUM and AAR) using the CONSORT 2010 checklist items and the individual items were marked as "present" or "absent." Assessment of adherence to individual checklist items as well as overall adherence to the CONSORT statement was done.
Statistical Analysis
Data for descriptive statistics were presented using frequencies and percentages. Data was analyzed using Microsoft Excel 2021 (Microsoft Corp., Redmond, WA, USA) and GraphPad Prism 9 software (GraphPad Software, San Diego, CA, USA). Normality was tested using the Kolmogorov-Smirnov test, and statistical tests such as the chi-square test or Fisher’s exact test were used for categorical data. Statistical tests were summarized with a p-value <0.05 level of significance and a confidence interval of 95%.
Results
Out of 817 articles screened in both journals from 2019 to 2023, a total of 61 articles were analyzed in our research, out of which 31 belonged to international and 30 belonged to Indian journals. Out of 427 articles published in international journals, 31 (7.25%) articles were RCTs, and out of 390 articles published in Indian journals, 30 (7.69%) articles were RCTs (Figure 1).
Study flowchart
Adherence of International Journal Articles to Individual Items in the CONSORT 2010 Checklist
Analysis of articles in international journals to CONSORT guidelines uncovered varying levels of adherence. A full adherence rate, i.e., 31 (100%), was noted with 10 key checklist items: structured summaries of trial design, methods, results, and conclusions; specific objectives or hypotheses; descriptions of trial design; eligibility criteria for participants; details of interventions for each group; numbers of participants for each group; outcome results; their interpretation, benefits, and harms; funding; and trial registration.
However, our analysis uncovered some significant shortcomings. Less than 50% of the studies adhered to CONSORT guidelines with respect to the changes to methods after trial commencement with justifications - 5 (16%), prespecified primary and secondary outcome measures and their assessment methods - 7 (22.5%), reporting changes to trial outcomes after commencement - 3 (9.6%), interim analysis and stopping guidelines - 2 (6.5%), allocation concealment mechanism and its implementation - 15 (48.4%), blinding - 14 (45.1%), methods for additional analyses - 7 (22.5%), recruitment details - 11 (35.5%), absolute and relative effect sizes for binary outcomes - 2 (6.4%), results of any other analyses and accessibility to full trial protocols - 2 (6.5%).
The overall adherence of the international journal to the CONSORT 2010 checklist was about 64% as demonstrated in Figure 2.
Adherence of articles in international journal
Adherence of Indian Journal Articles to Individual Items in the CONSORT 2010 Checklist
The articles adhered fully, i.e., 30 (100%), with respect to six checklist items: scientific background and explanation of rationale, specific objectives or hypotheses, eligibility criteria for participants, generalizability of findings, interpretation of results, and funding source.
Significant gaps were identified in several areas, with no adherence 0 (0%) observed for important changes to methods after trial commencement, any changes to trial outcomes after commencement, explanation of any interim analysis and stopping guidelines, description of similarity of interventions, reason for stopping of trial, for binary outcomes (absolute and relative effect sizes), and access to full protocol.
The overall adherence of the Indian journal to the CONSORT 2010 checklist was about 55.5% as demonstrated in Figure 3. The details of adherence of all the articles of both journals to the individual checklist items in CONSORT guidelines are given in Table 1.
Adherence of articles in Indian journal
Table 1: Adherence of all articles in BMC and IJP journals to the CONSORT 2010 guidelinesBMC: Biomed Central Pharmacology and Toxicology; IJP: Indian Journal of Pharmacology; CONSORT: Consolidated Standards of Reporting Trials*p-value < 0.05 is considered statistically significant
Comparison of Adherence Between the Two Journal Articles
In this review, we also compared the adherence between the two pharmacology journals chosen. A statistically significant difference (p < 0.05) was noted for some of the checklist items, such as items 3a, 5, 11b, 12a, 12b, 13a, 14a, 18, 19, 20, and 23. The details are mentioned in Table 1. Overall, a significant difference in adherence to CONSORT guidelines was observed between the two journals, with BMC journals demonstrating higher overall adherence (735, 64%) compared to IJP journals (616, 55.5%) (p < 0.05) as shown in Figure 4.
Overall adherence of international and Indian journal
Discussion
By scrutinizing 61 articles, this review highlights significant discrepancies in adherence between the international and Indian pharmacology journals, which provide valuable insights into the current state of reporting quality in scientific publications.
The overall adherence of the IJP journal was 616 (55.5%), and that of the BMC journal was 735 (64%), which was a statistically significant difference (p < 0.05). The perfect adherence to item 3a (description of trial design including allocation ratio) in the BMC journal compared to the (23, 76.6%) adherence in the IJP journal underscores the rigorous reporting standards upheld by the BMC journal. This distinction is statistically significant (p < 0.05), suggesting that BMC journal may be more committed to ensuring clarity in trial design, which is crucial for reproducibility and understanding of the studies. Similarly, perfect adherence was also observed in the analysis conducted by Huang et al. on 182 RCTs [12]. The complete adherence of the BMC journal to item 5 (intervention details) versus the (25, 83.3%) adherence in the IJP journal further emphasizes the superior reporting quality in BMC publications, which was also observed in an analysis done by McErlean et al., which also showed 100% adherence to item 5 for the international journal [3]. This aspect is vital for the replication of studies and for clinicians to understand and apply the findings accurately. Details about pre-specified primary and secondary outcome measures (item 6a) had similar adherence by both the journals. This was also observed in studies done by Susvirkar et al. and Goenka et al. [4,13]. The disparity observed in item 11b (description of the similarity of interventions) - 15 (48.4%) in the BMC journal and 0 (0%) in the IJP journal - reveals a significant gap in reporting standards, which was also noted in studies by Sarveravan et al. and McErlean et al., reporting about 81% and 73%, respectively, for international journals [3,14].
The most likely cause of non-adherence to some items in IJP may be that the items themselves are not applicable to the articles, such as item 3b (important changes to methods after trial commencement), item 6b (changes to trial outcomes after the trial commencement), item 7b (explanation of interim analysis and stopping guidelines), and item 14b (why the trial ended or was stopped). This was similarly observed in the systematic reviews of 244 RCTs and 50 RCTs done by Singh et al. and McErlean et al., respectively [3,7].
Statistical methods for analysis should be described with enough detail to yield an estimate of the treatment effect, which is a contrast between the outcomes in the comparison groups [2]. Adherence to item 12a, which involves statistical methods used to compare groups for primary and secondary outcomes, was markedly higher in BMC journal articles, i.e., 28 (90.3%), than in IJP journal articles, 3 (10%). This observation was also corroborated by the studies conducted by Canagarajah et al. and Stevanovic et al., which yielded a result of approximately 95.1% and 98% for the international journal [15,16]. This suggests that the BMC journal may place a stronger emphasis on detailed statistical reporting for primary and secondary outcomes compared to the IJP journal. Conversely, adherence to item 12b, which refers to methods for additional analyses such as subgroup and adjusted analyses, was more frequently observed in IJP journal articles - 19 (63.3%) - compared to BMC journal articles - 7 (22.5%). This was found to be higher in our review as compared to the systematic review done by Singh et al. (16%) for the Indian journal [7]. This indicates that the IJP journal might be more focused on reporting additional analytical methods, potentially reflecting different editorial priorities or author practices.
Moreover, adherence to item 13a, which involves reporting the numbers of participants who were randomly assigned, received intended treatment, and were analyzed for the primary outcome, was significantly higher, amounting to 30 (96.7%) in BMC journal articles, which was also in accordance with the research done by Susvirkar et al. [4]. This disparity highlights a potential area for improvement in the reporting standards of the IJP journal, emphasizing the need for stricter adherence to CONSORT guidelines to enhance the transparency and reliability of published RCTs. Conversely, the IJP journal demonstrated better adherence to item 14a (dates defining recruitment and follow-up), which came to be 23 (76.6%), and item 18 (results of additional analyses), which was 24 (80%); this indicates that while the BMC journal excels in certain areas, the IJP journal may provide more comprehensive timelines and additional analysis results, which are also critical components of transparent and thorough reporting.
Sample size determination was reported more in BMC journals, though not adequately, as it is required to ensure that these publications are transparent and comprehensible [17]. According to the analysis done by Warrier and Jayanthi, out of 276 trials assessed, sample size determination of Indian journals during 2017, 2018, and 2019 was reported to be about 72%, 70%, and 77%, respectively, which was found to be higher as compared to our research, which was about 13 (43.4%) [18]. In the analysis of 25 RCTs done by Juneja et al., sample size determination was found to be 46%, which was in concordance with our analysis [19]. According to the analysis done by Susvirkar et al., sample size determination in international journals was found to be 97.9%, which was found to be higher as compared to our result of about 20 (64.5%) for the BMC journal [4].
Despite these strengths, the IJP journal showed significantly lower adherence in reporting important harms and unintended effects (item 19), with only 8 (26.7%) adherences as compared to BMC's 27 (87%). This discrepancy is concerning as it suggests a potential underreporting of adverse effects, which is crucial for assessing the safety profile of interventions.
Additionally, BMC journal's superior adherence, i.e., 24 (77.5%) to reporting trial limitations and addressing potential sources of bias versus IJP's 7 (23.3%) and their complete compliance with trial registration reporting accounting for 31 (100%) versus IJP’s 15 (50%) highlight areas where IJP journal needs substantial improvement.
Limitations
The focus on a specific time frame (2019-2023) may not capture long-term trends or improvements in adherence to CONSORT guidelines over different time periods. Instead of only two journals, multiple journals could have been analyzed to measure the wide variability and adherence of different journals to CONSORT 2010 guidelines. Lastly, we could not discuss adherence to all the checklist items due to the word constraint of the journal.
Conclusions
This review highlights a significant variation in adherence to CONSORT 2010 guidelines between international and Indian pharmacology journals. The international journal demonstrated a higher overall adherence rate (64%) compared to the Indian journal (55.5%) (p < 0.05). Notably, the international journal excelled in reporting trial design, intervention details, harms, and statistical methods, whereas the Indian journal performed better in reporting additional analyses and recruitment details. However, both journals exhibited weaknesses in areas such as reporting changes to trial methodology, allocation concealment, and access to full trial protocols. To improve adherence, journals should enforce stricter editorial policies, provide reviewer training on guideline compliance, and encourage authors to follow best practices in trial reporting. Conducting workshops and establishing post-publication audits could further enhance adherence. Strengthening these measures will help ensure greater transparency, reproducibility, and reliability in the reporting of RCTs, ultimately improving the integrity of clinical research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Publication guidelines need widespread adoption J Clin Epidemiol Larson EL Cortazal M 2392466520122200081510.1016/j.jclinepi.2011.07.008 · doi ↗ · pubmed ↗
- 2CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials BMJ Moher D Hopewell S Schulz KF 0340201010.1136/bmj.c 869PMC 284494320332511 · doi ↗ · pubmed ↗
- 3The reporting standards of randomised controlled trials in leading medical journals between 2019 and 2020: a systematic review Ir J Med Sci Mc Erlean M Samways J Godolphin PJ Chen Y 738019220233523790810.1007/s 11845-022-02955-6PMC 8890950 · doi ↗ · pubmed ↗
- 4An assessment of the compliance of randomized controlled trials published in two high impact journals with the CONSORT statement Natl Med J India Susvirkar A Gada P Figer B Thaker S Thatte UM Gogtay NJ 79823120183082922210.4103/0970-258X.253165 · doi ↗ · pubmed ↗
- 5CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials BMJ Schulz KF Altman DG Moher D 0340201010.4103/0976-500X.72352 PMC 304333021350618 · doi ↗ · pubmed ↗
- 6Does use of the CONSORT statement impact the completeness of reporting of randomised controlled trials published in medical journals? a cochrane review Syst Rev Turner L Shamseer L Altman DG Schulz KF Moher D 60120122319458510.1186/2046-4053-1-60PMC 3564748 · doi ↗ · pubmed ↗
- 7Assessment of reporting quality of drug- related randomized controlled trials conducted in India and published in MEDLINE- indexed Indian journals over a decade: a systematic review Cureus Singh MP Prakash MG Gaikwad NR Keche YN Dhaneria S 015202310.7759/cureus.34353 PMC 997438336874727 · doi ↗ · pubmed ↗
- 8The quality of reports of randomised trials in 2000 and 2006: comparative study of articles indexed in Pub Med BMJ Hopewell S Dutton S Yu LM Chan AW Altman DG 0340201010.1136/bmj.c 723PMC 284494120332510 · doi ↗ · pubmed ↗