Effective coverage for maternal health: operationalising effective coverage cascades for antenatal care and nutrition interventions for pregnant women in seven low- and middle-income countries
Ashley Sheffel, Emily Carter, Rebecca Heidkamp, Aniqa Tasnim Hossain, Joanne Katz, Sunny Kim, Tsering Pema Lama, Tanya Marchant, Jamie Perin, Jennifer Requejo, Shelley Walton, Melinda K Munos

TL;DR
This study improves understanding of maternal health services by analyzing coverage and quality gaps in seven low- and middle-income countries.
Contribution
The paper operationalizes effective coverage cascades for antenatal care and nutrition services using real-world data from LMICs.
Findings
High service contact coverage for ANC1 exists, but drops significantly when adjusting for readiness and quality.
Gaps in provider training and nutrition counseling contribute to declines in effective coverage.
Effective coverage cascades reveal critical bottlenecks in service quality and readiness.
Abstract
Efforts to improve maternal health have focused on measuring health and nutrition service coverage. Despite improvements in service coverage, maternal mortality rates remain high. This suggests that coverage indicators alone do not fully capture the quality of care and may overestimate the health benefits of a service. Effective coverage (EC) cascades have been proposed as an approach to capture service quality within population-based coverage measures, but the proposed maternal health EC cascades have not been operationalised. This study aims to operationalise the effective coverage cascades for antenatal care (ANC) and maternal nutrition services using existing data from low- and middle-income countries (LMICs). We used household surveys and health facility assessments from seven LMICs to estimate EC cascades for ANC and maternal nutrition services provided during ANC visits. We…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
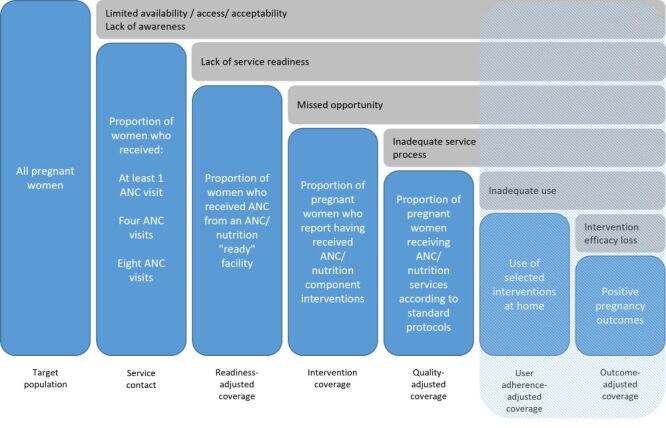 Figure 1
Figure 1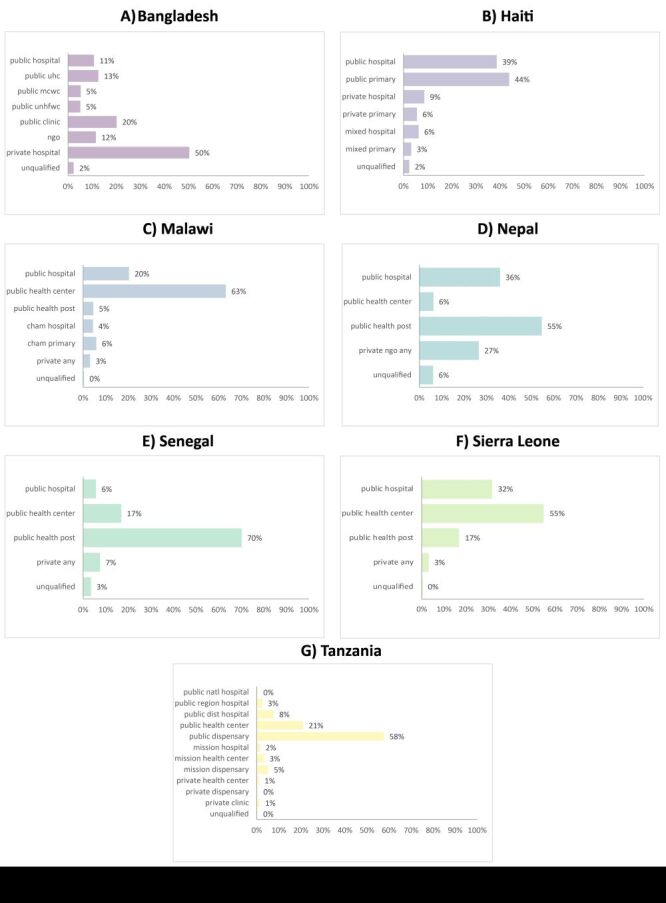 Figure 2
Figure 2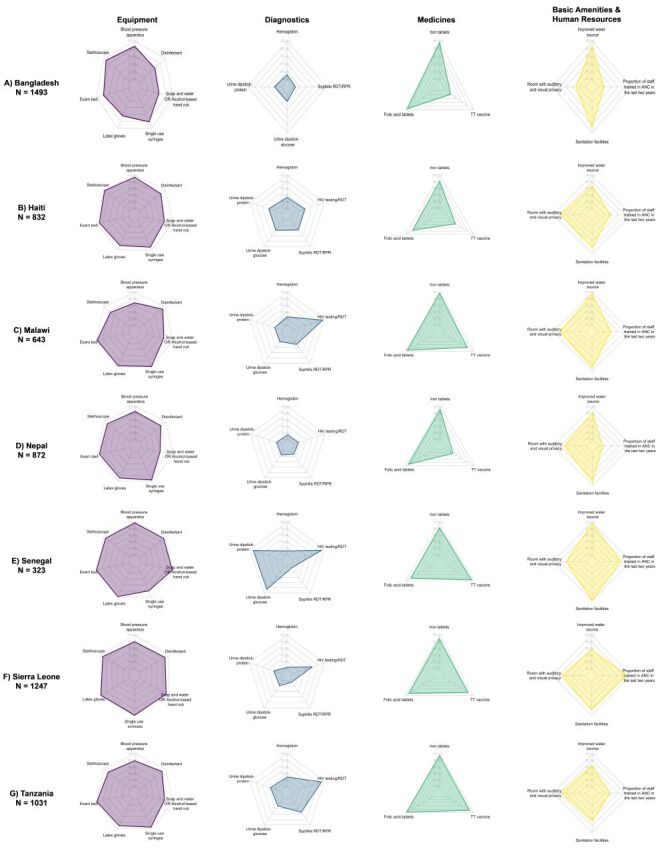 Figure 3
Figure 3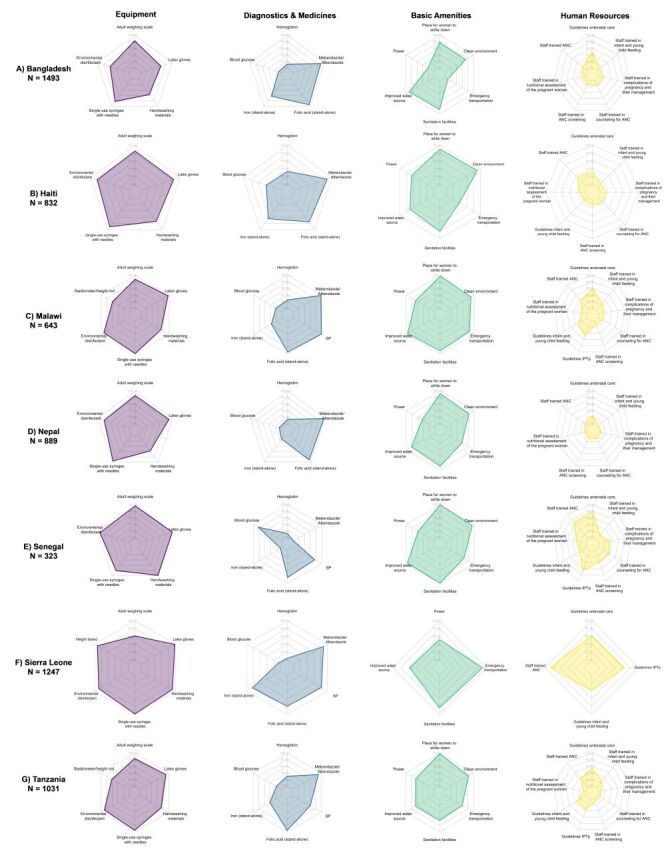 Figure 4
Figure 4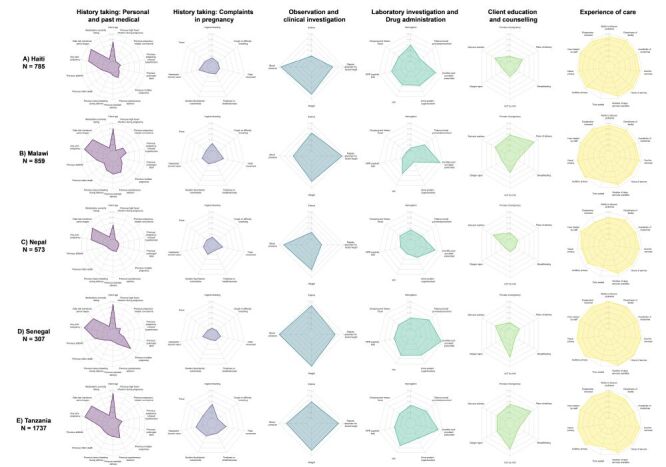 Figure 5
Figure 5 Figure 6
Figure 6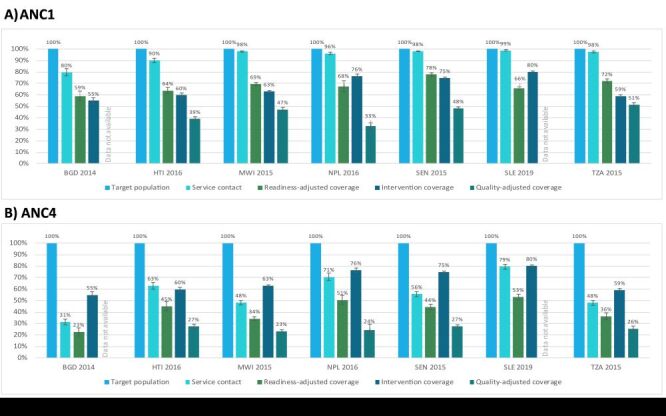 Figure 7
Figure 7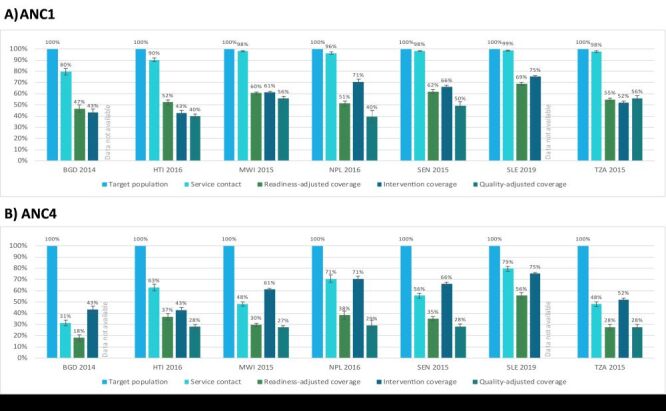 Figure 8
Figure 8| Cascade step | Theoretical definition | ANC/nutrition operational definition | Data source |
|---|---|---|---|
| Target population | All who need a service/ intervention | Women 15–49 years of age with a live birth in the last two years | HHS |
| Service contact coverage | Proportion of the target population who visit a health facility or qualified provider | Proportion of women 15–49 years of age with a live birth in the last two years who had at least 1/4/8 ANC contact(s) from a qualified provider during the most recent pregnancy. Note: Qualified provider was defined for each country and may include public sector, non-public sector, facility, and non-facility ( | HHS |
| Input- or readiness-adjusted coverage | Proportion of the target population who visited a health facility or qualified provider, given their mean readiness score | Proportion of women 15–49 years of age with a live birth in the last two years who received ANC from a health facility, scaled by the mean ANC/nutrition readiness score of the stratum. Note: Facility readiness was calculated on a scale of (0 to1) with 1 being perfect readiness and 0 being no readiness. Readiness was defined for each intervention, but typically accounts for basic amenities, equipment and supplies, medicines and commodities, diagnostics, and human resources needed to deliver the service or intervention according to standards. A mean readiness score was calculated for each stratum ( | HHS and HFA (facility audit) |
| Intervention coverage | Proportion of the target population who received the needed health intervention(s) or services | Proportion of women 15–49 years of age with a live birth in the last two years who reported receiving key interventions (average score of interventions received) during the most recent pregnancy. Note: Key interventions for ANC: tetanus toxoid vaccination (TT), sulfadoxine-pyrimethamine (SP) (where relevant), iron and folic acid supplementation (IFA), blood pressure measurement, urine sample, blood sample, and deworming; Key interventions for nutrition: SP (where relevant), IFA, blood sample, and deworming. | HHS |
| Quality-adjusted coverage | Proportion of the target population who visited a health facility or qualified provider, given the mean quality score | Proportion of women 15–49 years of age with a live birth in the last two years who received ANC from a health facility, scaled by the mean ANC/nutrition quality score ( | HHS and HFA (direct observation) |
| User adherence-adjusted coverage | Proportion of the target population receiving the intervention(s) or service according to recommended standards and adhering to the treatment guidelines | Not estimated. Note: Adherence is not relevant for all interventions; in cases where the intervention is entirely delivered by the provider and there is no home care, behaviour change, or continuing treatment needed, this component can be omitted. This is also difficult to define for a package of services such as ANC. | Not applicable |
| Outcome-adjusted coverage | Proportion of the target population experiencing the health gains from the service | Not estimated | Not applicable |
| Country | HHS | HFA |
|---|---|---|
| Bangladesh | DHS-VII 2014 | SPA 2014* |
| Haiti | DHS-VII 2016–17 | SPA 2013 |
| Malawi | DHS-VII 2015–16 | SPA 2013–14 |
| Nepal | DHS-VII 2016 | SPA 2015 |
| Senegal | DHS-VII 2017 | SPA 2016 |
| Sierra Leone | DHS-VI 2019 | SARA 2017* |
| Tanzania | DHS-VII 2015–16 | SPA 2014–15 |
| Country | Year | No. of women with a birth in the last two years | Total number of facilities | No. of facilities offering ANC | No. of ANC first visit clients |
|---|---|---|---|---|---|
| Bangladesh | DHS 2014, SPA 2014 | 3217 | 1596 | 1493 | NA* |
| Haiti | DHS 2016–17, SPA 2013 | 2583 | 907 | 832 | 785 |
| Malawi | DHS 2015–16, SPA 2013–14 | 6814 | 1060 | 643 | 859 |
| Nepal | DHS 2016, SPA 2015 | 2007 | 992 | 872 | 573 |
| Senegal | DHS 2017, SPA 2016 | 4926 | 484 | 323 | 307 |
| Sierra Leone | DHS 2019, SARA 2017 | 4057 | 1284 | 1247 | NA* |
| Tanzania | DHS 2015–16, SPA 2014–15 | 4283 | 1200 | 1031 | 1737 |
| Total | 27 887 | 7523 | 6441 | 4261 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Child Nutrition and Water Access · Healthcare Systems and Reforms
Improving maternal health and survival in low-income and middle-income countries (LMICs) remains at the forefront of the global health and development agenda [1]. While considerable progress has been made over the last two decades, the majority of maternal morbidity and mortality is preventable, yet remains unacceptably high and disproportionately occurring in LMICs. In 2020, the maternal mortality ratio (MMR) for the world’s least developed countries was nearly 30 times than that of the subregion Europe and Northern America [2]. In addition, the persistently high prevalence of maternal malnutrition in LMICs has remained unacceptably high – 450 million women in LMICs are estimated to have short stature, 240 million are underweight (body mass index (BMI)<18.5), and 468 million are anaemic [3] – and malnutrition has been exacerbated in recent years by the COVID-19 pandemic, increased conflict, and climate change resulting in further challenges to improving maternal health [4–9]. Key to improving maternal health is ensuring universal access to evidence-based interventions delivered with high quality [10–12].
Antenatal care (ANC) is an ideal platform on which to deliver and promote evidence-based, cost-effective interventions to improve maternal health within and beyond the pregnancy period. Antenatal care is important to maintaining a healthy pregnancy [13–15], promotes safe delivery and postnatal attendance, and is positively associated with an increase in facility-based deliveries [16–18]. In addition, ANC provides women with an important contact with the formal health system, leading to opportunities to access and utilise evidence-based interventions which promote maternal health and survival [19,20] including the delivery of vital maternal nutrition interventions as part of a comprehensive ANC service [21].
Global and national efforts to monitor the implementation of evidence-based, cost-effective interventions to improve maternal health have focused on measuring health service contact coverage, defined as the proportion of the target population in need of a service that received the service [22]. However, evidence of persistently high maternal mortality levels despite considerable improvements in coverage suggests that service contact coverage alone (e.g. at least one ANC visit) without accounting for service quality [23,24] can overestimate the health benefits of a service.
The concept of effective coverage aims to move beyond coverage to generate a better estimate of the benefit of a health service. Effective coverage indicators estimate the proportion of a population in need of a service that received the service with sufficient quality to achieve a positive health outcome [25–28]. The global health community has reached a general consensus that effective coverage for maternal health interventions can be conceptualised using a coverage cascade framework which outlines six steps:
-
service contact coverage
-
input-adjusted coverage
-
intervention coverage
-
quality-adjusted coverage (whereby quality refers to process quality or the provision and experience of care)
-
user adherence-adjusted coverage
Effective coverage has been defined as outcome-adjusted coverage, the final step of the cascade. However, for some interventions, quality-adjusted coverage may be a more suitable proxy measurement of effective coverage, particularly for routine preventative or promotive health services such as ANC during which multiple interventions are delivered [25]. In addition, readiness- and quality-adjusted coverage can be influenced through health system strengthening whereas there are a multitude of factors beyond the health system that can impact health outcomes, making readiness- and quality-adjusted coverage measures particularly important for improving the health system.
Despite consensus within the global health community on the concept of effective coverage cascades, research on how to operationalise these cascades for various services and data sources is limited. A recent review of effective coverage of maternal, newborn, and child health (MNCH) interventions found no consistent approach to the adjustments made to contact coverage [29]. However, evidence is growing on best practices for defining and generating effective coverage cascades using data from various sources. Munos et al recently set forth a set of best practices for generating estimates for effective coverage cascades using both household survey (HHS) data and health facility assessment (HFA) data [30]. Exley et al have explored operationalising the coverage cascade for facility-based childbirth interventions using HHS data and two sources of health facility data (HFA and routine health information data) [31] while Kim et al explored generating effective coverage estimates for maternal and newborn health services using HHS data [32]. The primary aim of this study was to operationalise effective coverage cascades for ANC and maternal nutrition services delivered during ANC in LMICs. By leveraging nationally representative, publicly available data, we sought to clearly define each step of the effective coverage cascade and to address the unique challenges associated with estimating each cascade step.
METHODS
Overview
Using publicly available HHS data and HFA data from seven LMICs (specified below), we estimated effective coverage cascades for ANC and maternal nutrition interventions delivered through ANC visits. We developed theoretical coverage cascades for ANC and maternal nutrition, defined facility readiness and provision/experience of care scores for each service using facility survey data, linked those scores to HHS data based on household location and reported type of facility utilised, and estimated the steps of the coverage cascade for each service and country. We adhered to best practices for generating estimates for effective coverage cascades as detailed in Munos et al and further described below [30].
Conceptualising the effective coverage cascade
We utilised the coverage cascade framework proposed by Amouzou et al. and adapted by the Effective Coverage Think Tank Group – a group of experts led by the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) – to develop a theoretical care cascade for ANC and maternal nutrition (Figure 1) [25,26]. We defined effective coverage as the proportion of all pregnant women (the target population) who progressed through six steps:
Theoretical effective coverage cascade for antenatal care and maternal nutrition. The last two steps of the cascade are shaded because they were considered not relevant/feasible for antenatal care.
-
attended a health facility for ANC (service contact coverage)
-
attended a health facility for ANC that had the appropriate inputs available (readiness-adjusted coverage)
-
received the appropriate interventions (intervention coverage)
-
attended a health facility for ANC where providers followed recommended standards or processes of care (quality-adjusted coverage)
-
adhered to selected interventions at home (user-adjusted coverage)
-
had positive pregnancy outcomes (outcome-adjusted coverage).
Table 1 provides operational definitions of each step of the coverage cascade for this analysis, using existing data from select countries. Further information on how to calculate each step of the cascade is provided subsequently in the methods section.
In 2016, WHO released new guidelines on ANC for a positive pregnancy experience, which recommends a minimum of eight ANC contacts (ANC8) as opposed to the earlier focused ANC model with its four recommended visits (ANC4) [19,20,33]. Due to the nature of multiple contacts with the health care system required for ANC, and variability in the expected timing of sequential visits, we have chosen to present three separate ANC cascades, defining service contact by the number of ANC visits (i.e. ANC1, ANC4+, ANC8+). We present the ANC8 cascade for all countries to reflect the implications of the new policy, although the majority of HHSs included in this analysis were conducted prior to 2016.
For this analysis, we explored both the complete package of services delivered through the ANC platform and the maternal nutrition interventions that are delivered during pregnancy. Although nutrition interventions are often delivered through a multi-faceted, multi-sectoral approach, antenatal consultations are an important platform for the delivery of nutrition interventions in pregnancy, especially as ANC attendance increases in LMICs [34,35]. In addition, HHSs and HFAs primarily collect data on maternal nutrition interventions delivered through ANC. As such, for the maternal nutrition cascade analysis, we focused on nutrition interventions delivered through the ANC platform.
Country selection
The seven countries included in this analysis are Bangladesh, Haiti, Malawi, Nepal, Senegal, Sierra Leone, and Tanzania. We selected countries based on regional geographic diversity (representation from East Africa, Latin American and the Caribbean, South Asia, and West Africa) and on the availability of both HHS and HFA data. Ideally the HFA would have occurred within the two years before the HHS, and we would limit the analysis of household survey respondents to those with births in the last two years. We selected this reference period for several reasons. First, the two-year reference period is aligned with the Multiple Indicator Cluster Survey (MICS) and the Demographic and Health Surveys (DHS) version VIII approaches, which acknowledge the limitations of a long recall period [36–38]. While the DHS-7 asks questions related to ANC for births in the last five years, the DHS-8 asks about births in the last three years and restricts the analysis to births in the last two years. Second, for effective coverage estimation, if a five-year reference period were selected, the HHS data for births that occurred over a five-year period would be linked to HFA data representative of a period of a few months. To reduce the potential mismatch between the HHS and HFA reference periods, the HHS reference period was limited to two years. This allows for a sufficient sample size of women while better reflecting the potential care received based on the HFA data. The exception is Haiti, which has a three-year gap between the HHS and HFA. We relaxed our inclusion criteria for this country in order to include representation of Latin America and the Caribbean as no surveys met the two-year criteria.
At the time of data analysis, we found that very few countries had recent HFAs that measured the quality of service provision. Even fewer had a recent HFA and HHS that could be linked (i.e. where the HFA fell within the reference period for the HHS) [30]. As a result, we included two countries with no ANC service quality data (i.e. no direct observation of care) – Bangladesh and Sierra Leone. Thus, the endpoint for the coverage cascade for these two countries was intervention coverage.
Data sources
For HHS data, we utilised data from the DHS program [39]. For the HFA data, we utilised data from the Service Provision Assessment (SPA) and the Service Availability and Readiness Assessment (SARA) [40,41]. The DHS and SPA are publicly available data. We obtained permission from the Sierra Leone Ministry of Health to use the 2017 SARA data. Table 2 presents the countries and data sources included in the analysis.
Household survey data
Data on care-seeking and intervention coverage among women with recent births were obtained from DHS. DHS are nationally representative HHSs with a large sample size that collect data on a wide range of population, health, and nutrition indicators. DHS survey data [36] was chosen over other available HHS data such as the MICS [38] because DHS collects information on the source of ANC care, which is needed for appropriate linkage of the HHS and HFA data sets [30]. Information on each HHS selected for this analysis can be found in Table S1 in the Online Supplementary Document.
Health facility assessment data
Data on health facilities and services were obtained from SPA and SARA surveys, which are HFAs that have many similarities and a few key differences [42]. SPA and SARA surveys both employ either a census or sample survey approach. Both surveys collect data on facility readiness through an inventory questionnaire, and the SPA and SARA programmes have harmonised a core set of service readiness indicators that can be collected with either tool. Service Provision Assessment surveys include additional modules including a provider interview, client observations for ANC visits, and exit interviews of ANC clients. However, these modules are not implemented in every country. Information on each HFA selected for this analysis can be found in Table S2 in the Online Supplementary Document.
While the SPA and SARA surveys are both HFAs, there are differences both between these surveys and within a survey programme across countries. First, unlike SPA, the SARA does not capture any information on provision/experience of care. In addition, certain SPAs (e.g. Bangladesh 2014) did not include observation/exit interview modules and therefore did not collect provision/experience of care data. There are also differences in the readiness items captured, and in the service areas in which readiness items are recorded. Some readiness items are captured only in the SPA, not the SARA (e.g. examination bed). The SPA assesses the presence of equipment and infection prevention and control items in multiple service areas while the SARA focuses solely on the outpatient department. In addition, the SPA utilises a staff roster to collect information on training for individual health workers while the SARA asks the service area in-charge whether at least one staff member providing the service has had training in the last two years. The SARA also focuses on broad areas of training (e.g. ANC training) while the SPA captures both broad training topics as well as more specific training areas (e.g. ANC screening, counselling for ANC, nutritional assessment of the pregnant woman). The SPA also has notable differences across countries. Some items are country-specific and therefore not collected in all SPAs (e.g. stadiometer only collected in Tanzania and Malawi). Finally, there are some services which are not part of the basic package of essential services in various countries due to the disease burden (e.g. HIV in Bangladesh; malaria in Bangladesh, Haiti, Nepal). As a result, these countries do not include items related to those services (e.g. HIV diagnostic capacity, SP tablets, guidelines for IPTp). Details on HFA data availability are in Table S3–4 in the Online Supplementary Document.
Defining and estimating coverage cascade steps
Table S5 in the Online Supplementary Document provides an overview of the indicators and data sources used to define each step of the coverage cascade for both ANC and maternal nutrition services delivered through ANC.
Target population
The target population, those in need of a service, was defined in the same way for both ANC and maternal nutrition cascades and was based on HHS data: women 15–49 years of age with a live birth in the last two years. The target population is the starting point for the effective coverage cascade, reflecting the population in need of the service or intervention which serves as the denominator for the cascade, and is therefore set at 100%.
Defining/estimating service contact
Service contact was defined in the same way for both ANC and maternal nutrition using three indicators and calculated from the HHS data: the proportion of women 15–49 years of age with a live birth in the last two years who had at least one ANC contact (ANC1), four or more ANC contacts (ANC4), and eight or more ANC contacts (ANC8) during the most recent pregnancy. In determining the number of ANC contacts a woman received, women who reported receiving ANC but who were unsure of the number of contacts were assumed to have had at least one contact and therefore we imputed one contact.
Defining/estimating intervention coverage
Intervention coverage was defined as the proportion of women 15–49 years of age with a live birth in the last two years who reported receiving key interventions (average score of interventions received) during the most recent pregnancy (Table 1), where the key interventions were defined separately for ANC and maternal nutrition. Similar to the content-qualified ANC coverage indicator (ANCq) approach proposed by Arroyave et al, intervention coverage estimates were generated at national level for each country by taking the average number of interventions received by each woman and then calculating the mean number of interventions across all women [43]. Indicator definitions for each of the key interventions are in Table S5 in the Online Supplementary Document. Not all key interventions were collected in all countries: Bangladesh excluded TT, SP for IPTp, IFA, and deworming; and Haiti and Nepal excluded SP for IPTp.
Defining/estimating readiness-adjusted and quality-adjusted coverage
Readiness-adjusted coverage was defined as the proportion of women 15–49 years of age with a live birth in the last two years who received ANC from a health facility, scaled by the mean ANC/nutrition readiness score of the stratum, where ANC readiness and nutrition readiness were defined separately for ANC and for maternal nutrition. Quality-adjusted coverage was defined similarly as the proportion of women 15–49 years of age with a live birth in the last two years who received ANC from a health facility, scaled by the mean ANC/nutrition quality score (i.e. provision/experience of care) of the stratum, where ANC quality and maternal nutrition quality during ANC visits were defined separately for ANC and for maternal nutrition. To calculate readiness-adjusted coverage and quality-adjusted coverage, we first defined facility readiness and provision/experience of care for both ANC and maternal nutrition.
Selection of ANC and nutrition readiness and provision and experience of care items was guided by WHO guidelines and recommendations [19,20,33], expert surveys conducted by Sheffel et al. [44] and King et al. [45], and data availability based on selected HFA questionnaires [41,46]. The ANC and maternal nutrition readiness and provision/experience of care indices were developed independently with independent expert surveys, prioritisation, and index development processes. This resulted in a few differences in intervention inclusion (e.g. the maternal nutrition index includes IPTp and deworming, while the ANC index does not) and more substantial differences in readiness and provision of care items included for each intervention (Table S3–4 in the Online Supplementary Document). We restricted the provision of care items to those required for a first ANC visit because for subsequent visits, the appropriate provision of care items are contingent on care received at previous visits and that information is not available in a cross-sectional facility survey. We also restricted the readiness analysis to items required for a first ANC visit to align with the selected provision of care items.
Because most of the readiness items were collected in the ANC module of the HFA questionnaire, we limited our analysis to facilities offering ANC services. For each facility or client included in the analysis, we defined binary (0/1) indicators for each item indicating whether the item was available at the time of the HFA. Binary indicators were created for all readiness items except for training, which was calculated from the health provider sections of the HFAs. Training indicators were defined as the proportion of health providers providing ANC services that had been trained in a particular intervention. A simple additive approach was utilised to generate an overall readiness score (unweighted average of the service readiness items available) and an overall provision/experience of care score (unweighted average of the provision/experience of care items received by a woman) for ANC and for maternal nutrition. For both ANC and maternal nutrition readiness indices and provision/experience of care indices, we found that items were relatively evenly distributed across domains and therefore the simple additive approach was appropriate for combining items into a single index score. This approach is consistent with a study on ANC which found small differences in the quality scores produced by three different approaches to combining items [44] as well as other studies which have taken a similar approach for developing quality of care indices for maternal and child health [45,47–49]. For the provision/experience of care index, we averaged all ANC client observations within a stratum (i.e. category of qualified provider or health facility in each region/district) rather than averaging ANC clients within individual facilities because we wanted to upweight higher caseload facilities within a stratum so that averages were representative of patient experience rather than representative of facilities. Averaging observations within a stratum implicitly weights the provision/experience of care indices by caseload (as caseload is correlated with number of observations in an HFA [50]).
We used an ecological approach, which has been validated in three previous studies [51–53], to link each woman 15–49 years of age with a live birth in the last two years in the HHS to stratum-specific overall readiness scores and provision/experience of care scores calculated from the HFA.
We first mapped health facility categories (level and managing authority) in the HFA (SARA/SPA) to response options for place of ANC in the HHS (DHS). The HHS response options for place of ANC sometimes differed substantially from the HFA facility type categories. Where it was unclear how these aligned, we consulted with colleagues with country-specific expertise. In addition, not all qualified sources of care reported in the HHS were represented in the HFA, particularly for community health workers (CHWs) and mobile clinics. For each HHS, we reviewed the HHS questionnaire along with country-specific guidelines to determine which qualified providers were not captured in the HFA, and to assess the most appropriate approach for mapping these providers to facility types.
We then assigned each woman 15–49 years of age with a live birth in the last two years in the HHS to a stratum based on the place of ANC services (health facility type/managing authority) and place of residence (region in BGD, HTI, NPL, SEN, and TZA; district in MWI and SLE). Average readiness and provision/experience of care scores were calculated for each stratum of health facilities in the HFA. These scores ranged from 0 (no required items present) to 1 (all required items present). Each ANC care-seeking episode in the HHS was then assigned stratum average readiness and provision/experience of care scores based on the type of facility the woman reported attending for ANC. If a woman sought care from more than one provider, we took the average of the scores for the provider/facility types recorded and assigned that value to the woman (care-seeking from non-qualified sources was ignored). For example, a woman who received ANC at a public health centre in Simiyu region, Tanzania, would be assigned the average readiness score for all public health centres in Simiyu region and the average provision/experience of care score for all women receiving ANC at public health centres in Simiyu region. In cases where no data was collected in the HFA for a facility type in a particular administrative area, the national average readiness score and provision/experience of care score for the corresponding health facility type was assigned to that stratum. Women who received ANC solely from unqualified providers were assigned a readiness score and provision/experience of care score of zero.
To estimate readiness-adjusted and quality-adjusted coverage in each country, we multiplied the binary ANC service contact coverage indicator (0/1) by the readiness score for each woman and the provision/experience of care score for each woman, respectively. We then calculated readiness-adjusted and quality-adjusted coverage at national level by taking an average of these values.
Analysis
We assessed each service contact coverage and intervention coverage indicator in each country for missing data and found that only Sierra Leone 2019 had missingness greater than 5% for IFA (for the number of times IFA was taken during the pregnancy). Missing data was not imputed. All service contact coverage, intervention coverage, and readiness- and quality- adjusted coverage estimates were generated using a design-based analysis to account for survey design. The mean readiness and provision of care scores were weighted using the SPA-calculated facility and client weights, respectively. The readiness-adjusted coverage and quality-adjusted coverage estimates were weighted using the DHS-calculated women’s weights. We used Taylor linearisation to estimate the variance for service contact coverage and intervention coverage accounting for clustering and stratification in the HHSs. For readiness- and quality- adjusted coverage, we used a jackknife approach to account for the variance from both HHSs and HFAs, where the variance was derived from the distribution generated by withholding each household cluster and each health facility and re-estimating readiness- and quality-adjusted coverage [54]. All analyses were completed using R, version 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria) and RStudio, version 2022.07.2 + 576 (RStudio, PBC, Boston, MA, USA). To assist others who would like to implement the methods and/or replicate these results, the statistical code written for these analyses is publicly available at: https://doi.org/10.5281/zenodo.7671806.
Ethical approval
This was a secondary analysis of publicly available, de-identified data sets and as such did not require ethical approval.
RESULTS
Background characteristics of surveys
The total analytical sample included interviews from 27 887 women with a birth in the last two years, audits from 7523 health facilities of which 6441 provided ANC services, and direct observation of 4261 ANC first visits across seven countries (Table 3).
Source of care
Public primary-level facilities were the most often utilised source of care in every country except Bangladesh, where private hospitals were the most common source of ANC (Figure 2). Public hospitals were also an important source of ANC in Haiti, Nepal, and Sierra Leone, where over one-third of women also sought care from a public hospital. Use of private facilities for ANC was low in all countries except Bangladesh where 50% of women sought care from a private hospital. Unqualified sources of care were utilised by less than 6% of women in all countries.
Variation in sources of antenatal care, by country. Panel A. Bangladesh. Panel B. Haiti. Panel C. Malawi. Panel D. Nepal. Panel E. Senegal. Panel F. Sierra Leone. Panel G. Tanzania. Women may have visited more than once source of care for ANC across the course of pregnancy thus percentages do not add up to 100% within a country. ANC – antenatal care, CHAM – Christian Health Association of Malawi, DIST – district, MCWC –maternal and child welfare centre, NATL – national, NGO – non-governmental organisation, UHC – upazila health complex, UNHFWC – union health and family welfare centre.
Readiness and provision/experience of care
Readiness
In general, ANC readiness decreased by level of facility within a managing authority (Figure S1 in the Online Supplementary Document). For example, in Haiti, in the public sector there was a 20-point gap in average ANC readiness between hospitals and primary health facilities, with a similar pattern for the private sector and mixed facilities (26-point and 20-point gaps, respectively, in ANC readiness between hospitals and primary health facilities). Facilities of the same level but different managing authorities tended to have similar levels of readiness. There was a similar pattern for maternal nutrition readiness (Figure S2 in the Online Supplementary Document), although the gaps were somewhat smaller than for ANC.
Across countries, for both ANC and maternal nutrition, the domains of diagnostics and human resources had the lowest availability (Figure 3, Figure 4; Table S6–7 in the Online Supplementary Document**)**. For ANC, medicines and equipment tended to have higher availability while for maternal nutrition, equipment and basic amenities tended to have higher availability. Within the human resources domain, countries tended to perform better on the availability of general ANC guidelines and staff trained broadly in ANC but scored poorly on nutrition topic-specific guidelines and staff training. Individual item availability for ANC readiness was variable with some items being nearly universally available, such as iron and folic acid and adult weighing scale, while other items had more limited availability, such as haemoglobin testing capacity and staff trained in ANC screening and ANC counselling.
Availability of antenatal care readiness items, by domain and country. Panel A. Bangladesh. Panel B. Haiti. Panel C. Malawi. Panel D. Nepal. Panel E. Senegal. Panel F. Sierra Leone. Panel G. Tanzania
Availability of maternal nutrition readiness items, by domain and country. Panel A. Bangladesh. Panel B. Haiti. Panel C. Malawi. Panel D. Nepal. Panel E. Senegal. Panel F. Sierra Leone. Panel G. Tanzania.
Provision/experience of care
Across countries for both ANC and maternal nutrition, we found that providers at all levels of facilities across managing authorities provided services with a similar level of quality, and there was little variability within a country (Figure S3–4 in the Online Supplementary Document). Individual ANC and maternal nutrition provision/experience of care items by domain are presented by country (Figure 5, Figure 6; Table S8–9 in the Online Supplementary Document). Across countries, providers were least likely to perform history-taking for complaints in pregnancy and client education and counselling while providers were more likely to perform observation and clinical investigation. In addition, clients reported a high level of satisfaction with the experience of care received. Some aspects of clinical care, such as weight and blood pressure assessment and provision of iron and/or folic acid, were almost universal, while syphilis testing, history-taking for a previous infant death, counselling on diet and nutrition, and counselling on exclusive breastfeeding were more limited.
Antenatal care provision/experience of care items, by domain and country. Panel A. Haiti. Panel B. Malawi. Panel C. Nepal. Panel D. Senegal. Panel E. Tanzania
Maternal nutrition provision/experience of care items, by domain and country. Panel A. Haiti. Panel B. Malawi. Panel C. Nepal. Panel D. Senegal. Panel E. Tanzania.
Effective coverage cascades
ANC
For the ANC1 cascade, as expected, coverage generally decreased across the cascade from service contact to quality-adjusted coverage (Figure 7). Service contact for at least one ANC visit was high across countries ranging from 80% in Bangladesh to 99% in Sierra Leone indicating high access to ANC services (Figure S5 and Table S10 in the Online Supplementary Document**)**. The drop in coverage from service contact to readiness-adjusted coverage ranged from 20 percentage points (pp) in Senegal to 33 pp in Sierra Leone, highlighting a gap in ANC service readiness across countries. Intervention coverage was not consistently lower than readiness-adjusted coverage, indicating that some women reported receiving ANC services despite the level of service readiness at facilities. In Nepal and Sierra Leone, intervention coverage was 9 pp and 14 pp higher than readiness-adjusted coverage respectively. In the other countries, intervention coverage was 3–13 pp lower than readiness-adjusted coverage and represents a missed opportunity to deliver ANC services. Finally, quality-adjusted coverage was the lowest in all countries with the gap from intervention coverage to quality-adjusted coverage, representing inadequate service process, ranging from 7 pp in Tanzania to 44 pp in Nepal. Across the cascade, there was an average net decline in coverage of 52 pp (55% relative decrease) from service contact to quality-adjusted coverage, while the average net decline from service contact to intervention coverage was 28 pp (29% relative decrease).
Antenatal care effective coverage cascades, by country. Panel A. At least one antenatal care visit. Panel B. Four or more antenatal care visits. BDG – Bangladesh, HTI –Haiti, MWI – Malawi, NPL – Nepal, SEN – Senegal, SLE – Sierra Leone, TZA – Tanzania.
The ANC4 and ANC8 coverage cascades followed a similar pattern as the ANC1 coverage cascades but with a few key differences (Figure 7; Figure S5 in the Online Supplementary Document). First, service contact was substantially lower in the ANC4 and ANC8 cascades, indicating lower access to four or more ANC visits. The proportion of women receiving at least four ANC visits ranged from 31% in Bangladesh to 79% in Sierra Leone while the proportion of women receiving at least eight ANC visits ranged from 0% in Senegal to 22% in Sierra Leone. The steep drop from target population to service contact in the ANC8 cascade left little room for further declines in readiness-adjusted and quality-adjusted coverage: on average, the net decline in coverage across the ANC8 cascade from service contact to quality-adjusted coverage was 3 pp (54% relative decrease). Second, intervention coverage was higher than readiness- and quality-adjusted coverage, because it was not restricted to women with 4+ or 8+ ANC visits. As a result, on average, the net increase in coverage across the cascade from service contact to intervention coverage was 10 pp for the ANC4 cascade (24% relative increase) and 59 pp for the ANC8 cascade.
Maternal nutrition
For the ANC1 maternal nutrition cascade, the drop in coverage from service contact to readiness-adjusted coverage ranged from 30 pp in Sierra Leone to 45 pp in Nepal, reflecting a larger gap in service readiness for nutrition interventions than for general ANC interventions (Figure 8; Figure S6 and Table S11 in the Online Supplementary Document. Similar to the overall ANC cascades, intervention coverage was not consistently lower than readiness-adjusted coverage, indicating that some women reported receiving maternal nutrition services despite low levels of service readiness at facilities. Quality-adjusted coverage for maternal nutrition was slightly higher than quality-adjusted coverage for ANC in all countries. On average there was a net decline in coverage of 48 pp (50% relative difference) across the ANC1 maternal nutrition cascade from service contact to quality-adjusted coverage and 38 pp (38% relative difference) from service contact to intervention coverage, similar to the gap in the overall ANC1 cascades. The ANC4 and ANC8 maternal nutrition coverage cascades were similar to the ANC1 maternal nutrition coverage cascades (Figure 8; Figure S7 in the Online Supplementary Document**)**. The key differences between the ANC4 and ANC8 maternal nutrition coverage cascades and ANC1 maternal nutrition cascades mirror those found for the ANC cascades.
Maternal nutrition effective coverage cascades, by country. Panel A. At least one antenatal care visit. Panel B. Four or more antenatal care visits. BDG – Bangladesh, HTI –Haiti, MWI – Malawi, NPL – Nepal, SEN – Senegal, SLE – Sierra Leone, TZA – Tanzania.
DISCUSSION
Our effective coverage cascade operationalisation for ANC and maternal nutrition services provides a rigorous approach to estimating effective coverage for these services by linking data sources commonly available in LMICs. Applying a set of best practices for effective coverage estimation, we found that effective coverage cascades provided a summary measure of service coverage and quality [30]. While the aim of this work was to identify the challenges in operationalising these cascades rather than to estimate ‘effective coverage’ for a particular country, we generally observed a substantial drop from service contact to readiness-adjusted coverage and a further drop to quality-adjusted coverage across countries and service areas. Our findings align with existing evidence demonstrating significant reductions in coverage when adjustments for service quality (readiness and process dimensions) are accounted for [26], emphasising the critical role of service quality in producing better health outcomes [10,55]. However, we also encountered challenges in operationalising the effective coverage cascades, including limited data availability, standardisation and comparability, and methodological complexity.
Added value of effective coverage cascades
Our analyses exemplify how the coverage cascade approach can highlight critical gaps in service access, readiness, and quality of care, offering actionable insights for policymakers aiming to strengthen health systems. By identifying specific bottlenecks in health service delivery, this approach facilitates the development of targeted interventions tailored to address setting-specific challenges [25,26]. For example, an analysis of facility readiness may reveal the need for investments in essential equipment, supplies, or trained personnel to address readiness gaps. Moreover, readiness-adjusted and quality-adjusted coverage measures provide a more nuanced understanding of facility quality, considering not only overall service quality but also the types of facilities where women most frequently seek care. This helps policymakers prioritise interventions and allocate resources to high-volume facilities where improvements could have the greatest impact on maternal health outcomes. While the coverage cascade approach can serve as a powerful tool for aligning interventions with the real-world contexts and needs of the population, evidence of the use of coverage cascades in guiding policy decisions remains limited. Despite the actionable findings demonstrated in our analysis, there is insufficient evidence on how countries are currently leveraging coverage cascades in practice. Further research is needed to better understand how policymakers in LMICs are utilising coverage cascades to inform and shape health policies.
Our operationalisation of the ANC and maternal nutrition cascades shed light on which steps of the cascade can be estimated. We did not estimate step 5 or step 6, user- or outcome-adjusted coverage, for ANC or maternal nutrition. Some ANC interventions do not require user adherence (e.g. TT injection) and among those that do, limited data on user adherence is collected. For example, adherence is required for IFA and calcium supplementation during pregnancy. Recent studies have found poor validity of IFA supplementation coverage and adherence questions in HHSs [56], and there is no data on calcium supplementation coverage or adherence in DHS or MICS. Outcome-adjusted coverage is not the ideal measure of ANC effective coverage as health outcomes such as reduced maternal mortality, neonatal mortality, and stillbirth are more strongly associated with the quality of labour and delivery care than ANC [13,57,58]. As such, the endpoint of the ANC care cascade and the preferred measure of effective coverage for ANC is step four, quality-adjusted coverage [25].
Challenge 1: Limited data availability, particularly for maternal nutrition
Data availability proved to be a challenge for operationalising the ANC and maternal nutrition effective coverage cascades. While the data for ANC is quite complete, we found more data gaps related to maternal nutrition, whereby some interventions were not represented in our analysis (e.g. calcium supplementation during pregnancy) [45]. In addition, recommended nutrition interventions provided during ANC are largely counselling-based, which is not captured well across data sources including HHSs and HFAs.
We also found discrepancies between data available in HHSs to estimate intervention coverage as compared to data available in HFAs to estimate readiness and provision of care. The measure of intervention coverage used for this analysis relies on reported receipt of seven interventions which pertain to observation and clinical investigation, laboratory investigation, and drug administration. Including only these seven ANC interventions assumes that these items are a good tracer for other interventions comprising a high-quality ANC service. Of these seven interventions, two (tetanus toxoid and iron-folic acid supplementation) can be delivered through multiple channels and not necessarily only during ANC. This is particularly true of tetanus toxoid vaccination coverage which is based on lifetime doses, meaning that a woman and her baby can be protected without having received any TT doses during the most recent pregnancy. In addition, this set of interventions does not capture important aspects of an ANC visit including history taking, counselling, and the client experience of care, which are equally important and well detailed in ANC clinical care guidelines but are difficult to ask about in an HHS. Based on our analysis of SPA observation data, we also found that these elements are the service components most likely to be excluded from an ANC visit. As a result, the intervention coverage measure may not accurately reflect the service quality received by pregnant women. The DHS-8 has added in four additional validated measures of content of care to assess the content of care more comprehensively, including listening to the baby’s heartbeat, nutrition counselling, breastfeeding counselling, and discussion of pregnancy danger signs (i.e. vaginal bleeding) [37]. Future HHSs thus may have a more comprehensive measure of intervention coverage, although using these additional questions will create challenges with historical comparability and cross-country comparability (when some countries have an older DHS survey and others have a new DHS survey).
Our experience of care measures incorporate aspects of respectful care; however previous studies have noted methodological challenges such as courtesy bias resulting in universally high levels of client satisfaction [44,59]. Validated measures of respectful ANC are in the early stages of development [60–62] and a validated 8-item scale measuring person centred ANC has been incorporated into the 2022 SPA questionnaires which may improve data availability going forward [63].
Finally, data on clinical quality of ANC and maternal nutrition is only available in a limited number of countries – namely those that have implemented a SPA survey. Future survey implementation of the Harmonized Health Facility Assessment (the successor to the SARA) may provide measures of clinical quality through a record review approach [64]. However, innovative methods to measure process quality on a more routine basis are needed to ensure availability of data across countries and at regular intervals. Effective coverage cascades are thus not a panacea for data gaps, and in fact highlight the need to improve the availability of data across LMICs to ensure countries have the data they need to track the ability of their health systems to deliver high quality care to all in need and make decisions on priority investments or improved intervention implementation.
Challenge 2: Standardisation and comparability
This analysis highlighted that effective coverage, while conceptually attractive, is quite complex and may prove challenging to implement on a larger scale while ensuring standardisation and comparability of cascades between countries. The lack of standardised definitions and indicators for measuring maternal health service quality continues to pose a challenge to constructing effective coverage cascades, particularly for global monitoring or cross-country comparison [29,65,66]. While work has been done to propose indicators and indices of service readiness and quality of care for ANC and maternal nutrition, there remains no consensus on standardised indicators of maternal quality of care [44,45,67]. Within our own analysis, we found that HFA tools were not fully harmonised resulting in different data availability depending on the type of survey used for the analysis and country-specific tool adaptations. This has implications for trying to generate effective coverage estimates that are comparable over time or across countries. The cascades that we generated are not therefore directly comparable across countries but may still be useful for within country monitoring and service delivery improvement. We chose not to standardise items to only those available across countries as this may not be indicative of a ‘high quality’ service in a particular country. While there was some variation in data availability across countries, data availability overall was relatively high as compared to other service areas, such as postnatal care and small and sick newborns [68,69]. ANC was one of the first service packages to be standardised with the focused ANC guidelines [19] which has enabled the development of tools designed to capture aspects of quality for the full package of interventions. In addition, as ANC is a preventative care platform, standardising the required items and tools is more straightforward.
Challenge 3: Methodological complexity
Numerous methodological decisions must be made to generate effective coverage estimates. While we followed a standard approach as per Munos et al., there were additional considerations for ANC and maternal nutrition specifically [30]. First, women may have multiple ANC visits across the course of the pregnancy and therefore may seek care from multiple sources. In these cases, we chose to take the average readiness score from the multiple sources of care to reflect the average client experience. Alternative approaches include utilising the source of care with the highest or lowest readiness which would result in maximum or minimum measures of service quality but might be less reflective of the client service delivery experience.
Second, this approach to effective coverage estimation does not capture non-facility-based interventions such as community-based care and informal sources of care such as pharmacies [30]. This is particularly a relevant issue for maternal nutrition as these interventions often have a community-based delivery platform in addition to facility-based care. Our measures of intervention coverage were sometimes higher than readiness-adjusted coverage; the receipt of ANC and maternal nutrition interventions outside of facility-based care that were not captured in this analysis may be a contributing factor to this finding.
Third, as the index development processes for ANC and maternal nutrition were independent and relied on independent groups of experts, in some cases an item was included in the nutrition readiness index but excluded in the ANC index (e.g. emergency transportation) [44,45]. We note that these decisions on what to include and exclude in the indices may lead to differences in the readiness and quality of care estimates and therefore the readiness-adjusted and quality-adjusted estimates. This can make it difficult to compare effective coverage across services and analyses and highlights the difficulty and importance of index development for use in effective coverage cascades.
Finally, utilising a HFA which incorporates direct observation of care and client exit interviews to estimate quality-adjusted coverage generates a measure of service quality that more accurately reflects the true quality of ANC a woman received. Direct observation allows for capturing information on provider adherence to clinical guidelines during service delivery, and the client exit interview allows for incorporation of aspects of client experience. However, there are some limitations to using this data in an effective coverage analysis. Using an ecological approach to link HFA and HHS data does not provide information on what a specific woman got at a particular visit; individual health records would be needed for this type of analysis. In addition, if the timing of the HHS and HFA are not well aligned, the time lag may result in quality-adjusted coverage measures that may not accurately reflect the service quality received by pregnant women in the household survey. The additional validated ANC content of care measures added to the DHS-8 have improved the feasibility of measuring ANC service quality from a HHS, which may diminish the added value of quality-adjusted coverage for ANC given these methodological challenges [43]. However future research is needed to enhance our understanding of whether the ‘new’ intervention coverage measures are good proxies for ANC service quality as measured through direct observations [43].
Limitations
Our study has some limitations. Because of data limitations, we used ecological linking of HHS and HFA data sets which means that women were not linked to the specific facility in which they sought care but rather a facility average for the type of facility in the region which they sought care. There are studies that suggest that this approach produces valid estimates, but there is a possibility of bias under certain conditions such as when there is a lot of variability in readiness and quality and/or high levels of preferential care-seeking [52,70]. In addition, due to data limitations, we linked data sets with a two to three year time difference. However, we utilised the most robust methods available for the data that was available to us. These methodological choices and resulting limitations should be taken into consideration when deciding when and how to use effective coverage measures of ANC and maternal nutrition. In addition, this work relied on survey data and did not utilise routine health information system data for measures of service readiness or service quality. More research is needed to determine the availability and feasibility of using routine data for effective coverage estimation. Our readiness and quality measures were based on expert surveys, the WHO quality of care framework, and data availability and were not always comparable across countries. However, our approach to index development followed a rigorous process and was supported by evidence that overall ANC readiness and quality scores are not greatly affected by the addition or removal of a few items [44]. Finally, this study did not include country consultation on the item inclusion for readiness and quality indices, as the aim of this work was to identify the challenges in operationalising these cascades rather than to estimate ‘effective coverage’ for a particular country. However, this method’s application has shown that much country adaptation is required to make these analyses relevant to a given country context, and more work is needed to understand the utility of these measures for country stakeholders.
CONCLUSIONS
The coverage cascade approach yielded summary measures that were useful for identifying high-level barriers to effective coverage of antenatal care and maternal nutrition; however, detailed measures within the cascade – such as source of care, readiness and quality scores by domain, or the availability of individual items – may be needed for evidence-based decision making. This exercise highlights how an effective coverage cascade may illustrate the potential bottlenecks in achieving expected health benefits from services and the inter-connectedness of service access and service quality in achieving improvements in health status. Increased collection and standardisation of ANC and maternal nutrition quality of care data are needed to improve measurability and comparability of effective coverage cascades. Future work on usability of routine data along with analyses focusing on subregional effective coverage and disaggregation based on level of health facility may improve the usefulness of effective coverage estimates for targeting interventions and resource allocation.
Additional material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1United Nations. SDG 3: Ensure healthy lives and promote wellbeing for all at all ages. Available: https://sdgs.un.org/goals/goal 3. Accessed: 28 June 2022.
- 2Christian P Smith ER Zaidi A Addressing inequities in the global burden of maternal undernutrition: the role of targeting. BMJ Glob Health. 2020;5:e 002186. 10.1136/bmjgh-2019-00218632231793 PMC 7101036 · doi ↗ · pubmed ↗
- 3Victora CG Christian P Vidaletti LP Gatica-Domínguez G Menon P Black RE Revisiting maternal and child undernutrition in low-income and middle-income countries: variable progress towards an unfinished agenda. Lancet. 2021;397:1388–99. 10.1016/S 0140-6736(21)00394-933691094 PMC 7613170 · doi ↗ · pubmed ↗
- 4Mark HE Dias da Costa G Pagliari C Unger SA Malnutrition: the silent pandemic. BMJ. 2020;371:m 4593. 10.1136/bmj.m 459333262147 PMC 7705612 · doi ↗ · pubmed ↗
- 5Popkin BM Corvalan C Grummer-Strawn LM Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet. 2020;395:65–74. 10.1016/S 0140-6736(19)32497-331852602 PMC 7179702 · doi ↗ · pubmed ↗
- 6Seferidi P Hone T Duran AC Bernabe-Ortiz A Millett C Global inequalities in the double burden of malnutrition and associations with globalisation: a multilevel analysis of Demographic and Health Surveys from 55 low-income and middle-income countries, 1992–2018. Lancet Glob Health. 2022;10:e 482–90. 10.1016/S 2214-109X(21)00594-535148831 PMC 8924053 · doi ↗ · pubmed ↗
- 7Kruk ME Gage AD Arsenault C Jordan K Leslie HH Roder-De Wan S High-quality health systems in the Sustainable Development Goals era: time for a revolution. Lancet Glob Health. 2018;6:e 1196–252. 10.1016/S 2214-109X(18)30386-330196093 PMC 7734391 · doi ↗ · pubmed ↗
- 8TunçalpӦWere WM Mac Lennan C Oladapo OT Gulmezoglu AM Bahl R Quality of care for pregnant women and newborns-the WHO vision. BJOG. 2015;122:1045–9. 10.1111/1471-0528.1345125929823 PMC 5029576 · doi ↗ · pubmed ↗