An Adult Case of Diabetes With High Levels of GAD Antibodies Without Insulin Deficiency for More Than 10 Years
Hideyuki Takeuchi, Naoyuki Iso-O, Atsuko Takai, Takashi Mikamo, Kozue Nagumo, Masumi Hara

TL;DR
A 56-year-old woman with high GAD antibodies and diabetes maintained insulin production for over 10 years, challenging assumptions about autoimmune diabetes progression.
Contribution
This case shows that high GAD antibody levels do not always lead to rapid insulin deficiency in autoimmune diabetes.
Findings
The patient had high GAD antibodies but preserved insulin secretion for over a decade.
Positive GAD antibodies alone are not reliable predictors of insulin deficiency.
Early treatment should focus on weight management and CVD prevention when insulin secretion is preserved.
Abstract
Latent autoimmune diabetes in adults (LADA) or slowly progressive insulin-dependent diabetes mellitus (SPIDDM) is a form of autoimmune diabetes characterized by autoimmune destruction of pancreatic beta cells, leading to deficient insulin secretion. Here, we report a case of diabetes and obesity in a 56-year-old woman. She was diagnosed with severe obesity, impaired glucose tolerance (IGT), and a positive antiglutamic acid decarboxylase antibody (GADA) test result at the age of 39 years. She developed diabetes 7 years later, meeting the diagnostic criteria for SPIDDM (probable). Despite high GADA levels, her endogenous insulin secretion has been preserved for over a decade. GADA has been regarded as a marker of autoimmune destruction of pancreatic beta cells, and high levels of GADA are considered a risk factor for future insulin deficiency. However, the role of GADA in its pathogenesis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
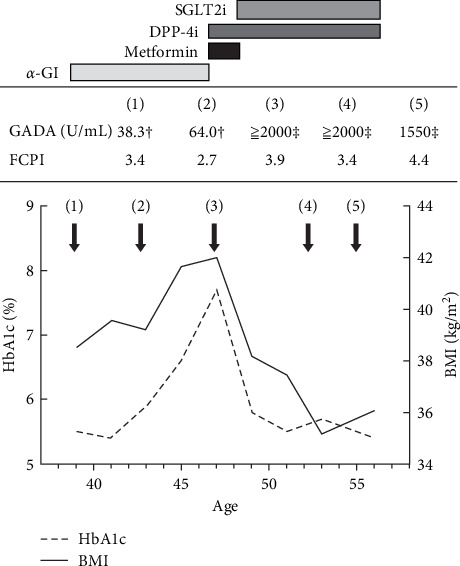 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes and associated disorders · Diabetes Management and Research · Pancreatic function and diabetes
1. Introduction
Latent autoimmune diabetes in adults (LADA) is one of the adult-onset autoimmune diabetes, characterized by autoimmune destruction of pancreatic beta cells, leading to deficient insulin secretion. A pathological condition similar to LADA is called slowly progressive insulin-dependent diabetes mellitus (SPIDDM) [1, 2]. SPIDDM differs from fulminant [3] and acute-onset [4] type 1 diabetes because it causes slow pancreatic beta cell destruction and has early clinical features similar to those of type 2 diabetes. Autoantibodies such as antiglutamic acid decarboxylase antibody (GADA), anti-insulinoma-associated antigen-2 (IA-2) antibody, anti-insulin autoantibody, and anti-zinc transporter protein 8 (ZnT8) antibody are often associated with the autoimmune destruction of pancreatic beta cells. Several risk factors for insulin deficiency in patients with autoimmune diabetes have been reported [5–7]. Among them, high GADA levels, especially as measured by enzyme-linked immunosorbent assay (ELISA), have been reported to be a risk factor for insulin deficiency.
It has been reported that the early introduction of insulin therapy for LADA and SPIDDM may preserve pancreatic beta cell function [8, 9]. However, some patients with autoimmune diabetes do not progress to insulin deficiency over long periods [10, 11]. Many of these patients are obese and share clinical features with those with type 2 diabetes. Early introduction of insulin therapy in these patients may lead to weight gain, worsen long-term glycemic management, and increase the incidence of atherosclerotic cardiovascular disease (ASCVD). Although there are no treatment guidelines for LADA or SPIDDM, the consensus statement by an international expert panel [12] and the report by the Japan Diabetes Society that presents the diagnostic criteria for SPIDDM [2] recommend that, in cases where endogenous insulin secretion is maintained, a treatment plan should be formulated in accordance with the guidelines for type 2 diabetes, with the exception of the use of sulfonylurea agents.
Here, we report a case that met the diagnostic criteria for SPIDDM (probable) with persistently high GADA levels measured by ELISA, although the patient had obese type 2 diabetes-like clinical features with no insulin deficiency for more than 10 years after being diagnosed with impaired glucose tolerance (IGT).
2. Case Presentation
The patient was a 56-year-old Japanese woman with severe obesity and a history of Graves' disease. At the age of 39, she came to our hospital with suspicion of IGT. At the time of her first visit, her BMI was 38.5 kg/m^2^, and a 75 g oral glucose tolerance test (OGTT) indicated IGT and insulin resistance (Table 1). No dyslipidemia or hypertension was observed. At the same time, the patient tested positive for GADA. The subsequent clinical course is shown in Figure 1. She had a history of autoimmune thyroid diseases (AITDs); she had Graves' disease in her twenties but was in remission at the time of her first visit and was positive for anti-TPO and antithyroglobulin antibodies. Her thyroid function had been within normal limits since her first visit. After several months of lifestyle modifications, the patient was started on an alpha-glucosidase inhibitor to prevent progression to diabetes mellitus. At the age of 46, she progressed from IGT to diabetes based on elevated fasting blood glucose and HbA1c levels. Her GADA levels remained extremely high (≥2000 U/mL in ELISA), but fasting C-peptide levels did not indicate a decrease in endogenous insulin secretion. Tests for other islet-associated autoantibodies, such as anti-IA-2, anti-ZnT8, and anti-insulin antibodies, were negative. Metformin was started in place of an alpha-glucosidase inhibitor, followed by the addition of a DPP-4 inhibitor. In 2016, the method of measuring GADA changed from radioimmunoassay (RIA) to ELISA in Japan. Since then, her GADA levels have remained high, above 2000 U/mL. At the age of 47 years, an SGLT2 inhibitor was started for the purpose of weight loss, and metformin was withdrawn because of good glycemic control. At the age of 56 years, she was obese with a BMI of 35 but maintained good glycemic management with an HbA1c level of ~6% on DPP-4 and SGLT2 inhibitors. Fasting blood CPR did not decrease, at ~4 ng/mL, and GADA values slightly decreased but remained high at 1300–1600 U/mL.
3. Discussion
LADA is defined as diabetes that develops in people aged 30 years or older, who have at least one islet cell-associated autoantibody, and who are insulin-independent for at least 6 months after diagnosis [13]. This case fits the definition because the patient developed diabetes at the age of 46 years and did not require insulin treatment for a long time, despite having high GADA levels. In addition, this case met the diagnostic criteria for “SPIDDM (probable)” set by the Japan Diabetes Society. Considering the patient's significant obesity and preserved insulin secretion, this case should rather be diagnosed as SPIDDM (probable) and should be followed up while assessing the degree of insulin secretion ability.
This case provides two implications for determining treatment strategies for autoimmune diabetes. First, a single positive GADA result, even if measured by ELISA and a high titer, is not sufficient to predict the risk of insulin deficiency in an individual case. Second, for people with autoimmune diabetes who are obese and exhibit the clinical features of type 2 diabetes, the prevention of body weight gain and development of cardiovascular diseases (CVDs) are important treatment goals. Periodic evaluation of endogenous insulin secretion is necessary, and basic pharmacotherapy should be performed in accordance with the treatment guidelines for type 2 diabetes, except for the use of sulfonylurea agents.
A single positive GADA, even at a high titer, is not sufficient to predict the risk of insulin deficiency in individual cases. The diagnosis of LADA and SPIDDM requires the presence of positive islet-specific autoantibodies, such as GADA, anti-IA-2 antibody, anti-insulin autoantibody, and anti-ZnT8 antibody. Although these autoantibodies are detected in association with autoimmune injury to pancreatic beta cells, the autoantibodies themselves may not be the direct cause of pancreatic beta cell injury but rather merely markers of the autoimmune response to pancreatic beta cells [14]. Furthermore, GADA is known to be positive in other autoimmune diseases such as AITD and stiff-person syndrome [15]. GADA is also known to be positive in some people with phenotypic type 2 diabetes and even in healthy individuals [16]. Therefore, GADA is not a specific marker of pancreatic beta cell injury.
In contrast, GADA is the most commonly used sensitive marker for diagnosing LADA and SPIDDM, and high GADA titers have been reported to be associated with a subsequent decrease in endogenous insulin secretion [5, 7, 17, 18]. In a Swedish population study using GADA 250 IU/mL as a cutoff and dividing the patients into high or low, the percentage of patients requiring insulin therapy at 6 months was 42.2% for the high-titer group compared with 3.7% for phenotypic type 2 diabetes [19]. In particular, the clinical utility of GADA has improved since the change of the assay system from RIA to ELISA [20]. However, in some cases, such as the present case, endogenous insulin secretion is not reduced for a long period of time [10]. According to the American Diabetes Association (ADA) stage classification of type 1 diabetes, presymptomatic type 1 diabetes (stage 1) is defined as having two or more type 1 diabetes-associated islet autoantibodies [21]. Similarly, in LADA and SPIDDM, the presence of multiple islet-associated autoantibodies may be helpful in assessing the risk of future insulin deficiency. For the report on GADA measured by RIA, there is also a report that patients who tested positive for multiple antibodies were at a higher risk of requiring insulin therapy than those who tested positive for GADA alone [22].
In addition to GADA, various other risk factors for insulin deficiency in patients with autoimmune diabetes have been reported (Table 2). Although the GADA level was extremely high in the present case, many other aspects suggested a low risk of insulin deficiency. No islet-associated autoantibodies other than GADA were detected, the BMI was high, and there was no evidence of decreased endogenous insulin secretion. This patient did not have any HLA genotypes reported to be susceptible to type 1 diabetes in the Japanese population but had DRB1^∗^15:02 and DQB1^∗^06:01, which are considered protective [5, 26]. Based on the above, the risk of developing insulin deficiency in this case was estimated to be low, even considering the high GADA level. Although this is only a case report, in patients who do not develop insulin deficiency even after a certain period after the diagnosis of autoimmune diabetes, as in the present case, HLA genotype analyses may be useful for risk assessment of insulin deficiency and subsequent treatment decisions. A positive anti-TPO antibody result has been reported to be a risk factor for insulin deficiency in LADA [24]. However, GADA is sometimes positive in AITD, although its relationship with the pathogenesis is not clear. Therefore, when GADA is the only positive islet cell-related autoantibody in patients with AITD, the possibility of a GADA-positive result other than islet-associated autoimmunity should be considered.
At present, there are no treatment guidelines for LADA or SPIDDM; however, a consensus statement by an international expert panel [12] and diagnostic criteria for SPIDDM [2] have been presented. In these reports, while endogenous insulin secretion was preserved and the risk of insulin deficiency was low, it is recommended that treatment be carried out in accordance with the guidelines for type 2 diabetes, except for the use of sulfonylurea agents. Early introduction of insulin therapy tends to be the treatment of choice after the diagnosis of autoimmune diabetes, as there are reports [9, 25] that early introduction of insulin therapy for LADA and SPIDDM has contributed to the preservation of endogenous insulin secretion compared with sulfonylurea. However, in obese patients, as in the present case, early insulin induction increases weight gain, thereby worsening long-term glycemic management and increasing the risk of ASCVD due to hyperinsulinemia. The risk of death in patients with LADA has been reported to be as high as that in patients with type 2 diabetes, and the CVD risk is particularly high when the GADA levels are high, as in this case [19].
The primary goals in the treatment of this patient were to prevent body weight gain and CVD. After being diagnosed with diabetes mellitus, the patient was started on metformin and SGLT2 inhibitors, followed by lifestyle modification guidance and good glycemic management. DPP-4 inhibitors were also administered because small clinical trials have suggested that they may retard insulin deficiency in patients with autoimmune diabetes [27–30]. Administration of GLP-1 or GLP-1/GIP might also be helpful if glycemic management worsens or if weight loss is difficult [31].
4. Conclusion
We report a case of obese diabetes that met the diagnostic criteria for SPIDDM (probable), with GADA levels remaining extremely high for over 10 years, but without a decline in endogenous insulin secretion. Even if GADA is high in a highly specific ELISA assay, a positive result for GADA alone is not sufficient to predict insulin deficiency in an individual case. Therefore, multiple islet-associated autoantibodies and endogenous insulin secretion should be evaluated. Obese patients with autoimmune diabetes and preserved endogenous insulin secretion should be treated according to the guidelines for type 2 diabetes with regular assessment of endogenous insulin secretion, except for the use of sulfonylurea agents.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nishimura A. Matsumura K. Kikuno S. Slowly Progressive Type 1 Diabetes Mellitus: Current Knowledge And Future Perspectives, Diabetes Metab Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy 2019122461247710.2147/DMSO.S 19100731819572 PMC 6886592 · doi ↗ · pubmed ↗
- 2Shimada A. Kawasaki E. Abiru N. New Diagnostic Criteria, 2023 for Slowly Progressive Type 1 Diabetes (SPIDDM): Report From Committee on Type 1 Diabetes of the Japan Diabetes Society (English Version) Journal of Diabetes Investigation 202415225425710.1111/jdi.1412138184802 PMC 10804889 · doi ↗ · pubmed ↗
- 3Imagawa A. Hanafusa T. Miyagawa J.-I. Matsuzawa Y. A Novel Subtype of Type 1 Diabetes Mellitus Characterized by a Rapid Onset and an Absence of Diabetes-Related Antibodies New England Journal of Medicine 2000342530130710.1056/NEJM 2000020334205012-s 2.0-003459876110655528 · doi ↗ · pubmed ↗
- 4El Sayed N. A. Aleppo G. Aroda V. R. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes—2023 Diabetes Care 202346 S 19S 403650764910.2337/dc 23-S 002PMC 9810477 · doi ↗ · pubmed ↗
- 5Yasui J. Kawasaki E. Tanaka S. Clinical and Genetic Characteristics of Non-Insulin-Requiring Glutamic Acid Decarboxylase (GAD) Autoantibody-Positive Diabetes: A Nationwide Survey in Japan P Lo S ONE 201611510.1371/journal.pone.01556432-s 2.0-84971265367 e 0155643 PMC 486669127177031 · doi ↗ · pubmed ↗
- 6Wada E. Onoue T. Kinoshita T. Adult-Onset Autoimmune Diabetes Identified by Glutamic Acid Decarboxylase Autoantibodies: A Retrospective Cohort Study Diabetologia 202164102183219210.1007/s 00125-021-05516-134268631 · doi ↗ · pubmed ↗
- 7Buzzetti R. Di Pietro S. Giaccari A. High Titer of Autoantibodies to GAD Identifies a Specific Phenotype of Adult-Onset Autoimmune Diabetes Diabetes Care 200730493293810.2337/dc 06-16962-s 2.0-3414714006017392553 · doi ↗ · pubmed ↗
- 8Maruyama T. Tanaka S. Shimada A. Insulin Intervention in Slowly Progressive Insulin-Dependent (Type 1) Diabetes Mellitus The Journal of Clinical Endocrinology & Metabolism 20089362115212110.1210/jc.2007-22672-s 2.0-4514910963118397986 · doi ↗ · pubmed ↗