Severe Hypocalcemia Leading to Trousseau's Sign
Tanique A Burke, Cesar M Almanza, Logan C Hager, Damian Casadesus

TL;DR
This case report discusses a young woman with severe low blood calcium after thyroid surgery, emphasizing the importance of education and follow-up care.
Contribution
The novelty lies in highlighting a rare physical finding and the need for patient education post-total thyroidectomy.
Findings
Severe hypocalcemia occurred after total thyroidectomy in a young woman.
Routine follow-up and patient education are crucial for postoperative management.
Complications include lifelong thyroid hormone needs and nerve injuries.
Abstract
Hypocalcemia is a common complication post-total thyroidectomy. This case report of a young woman with a rare finding on a physical examination highlights the need for patient education, routine laboratory work, and follow-up post-total thyroidectomy. Hypocalcemia is an electrolyte abnormality with numerous causes including chronic kidney disease, vitamin D deficiency, rhabdomyolysis, medications, and hyperventilation. In this report, we discuss the complications and management of hypocalcemia associated with total thyroidectomy. Significant complications include the lifelong need for T4, hypocalcemia, and recurrent and superior laryngeal nerve injuries. The study concludes with the importance of careful primary care follow-ups, medication adherence, and education in postoperative management.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
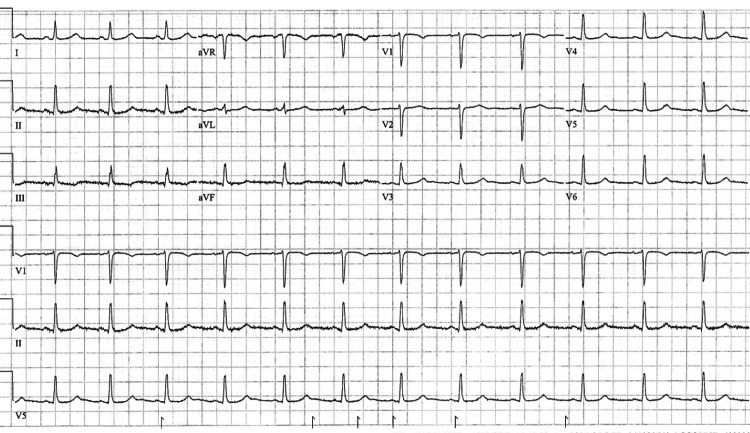 Figure 1
Figure 1| Measurement | Patient values | Normal values |
| Calcium | 5.7 mg/dL | 8.4-10.2 mg/dL |
| Ionized calcium | 0.93 mg/dL | 4.2-5.6 mg/dL |
| 25-hydroxyvitamin D | 19 ng/mL | 20-40 ng/mL |
| Parathyroid hormone | 3 pg/mL | 10-60 pg/mL |
| Thyroid-stimulating hormone | 2.92 μU/mL | 0.4-4.0 μU/mL |
| Magnesium | 1.2 mEq/L | 1.5-2.0 mEq/L |
| Potassium | 5.3 mEq/L | 3.5-5.0 mEq/L |
| Creatinine | 0.70 mg/dL | 0.6-1.2 mg/dL |
| Albumin | 3.6 g/dL | 3.5-5.5 g/dL |
| AST | 106 U/L | 10-40 U/L |
| ALT | 74 U/L | 12-38 U/L |
| Measurement | Patient values | Normal values |
| Calcium | 9.4 mg/dL | 8.4-10.2 mg/dL |
| Ionized calcium | 0.15 mg/dL | 4.2-5.6 mg/dL |
| 25-hydroxyvitamin D | 30 ng/mL | 20-40 ng/mL |
| Parathyroid hormone | 3 pg/mL | 10-60 pg/mL |
| Thyroid-stimulating hormone | 3.1 μU/mL | 0.4-4.0 μU/mL |
| Magnesium | 1.5 mEq/L | 1.5-2.0 mEq/L |
| Potassium | 4.7 mEq/L | 3.5-5.0 mEq/L |
| Creatinine | 1.00 mg/dL | 0.6-1.2 mg/dL |
| Albumin | 4.4 g/dL | 3.5-5.5 g/dL |
| ALT | 83 U/L | 10-40 U/L |
| AST | 51 U/L | 12-38 U/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid and Parathyroid Surgery · Sympathectomy and Hyperhidrosis Treatments · Trigeminal Neuralgia and Treatments
Introduction
Hypocalcemia is an electrolyte dysfunction characterized by corrected serum total calcium levels < 8.5 mg/dL or uncorrected < 2.12 mmol/L [1]. Hypocalcemia-related disorders are divided into parathyroid hormone (PTH)-mediated and non-PTH-mediated causes, which can be further subdivided into acquired and genetic components. Thyroidectomy is a surgical procedure that involves the removal of all or part of the thyroid gland. This procedure is typically performed to treat conditions such as thyroid cancer, benign thyroid nodules, hyperthyroidism, or goiters. A total thyroidectomy involves the removal of the entire thyroid, whereas a partial thyroidectomy is the removal of a portion of the thyroid. It is important to note that postsurgical hypoparathyroidism (PTH-mediated) is the most common cause of hypocalcemia overall [1].
The diagnosis of postoperative hypocalcemia involves assessing clinical symptoms and confirming the diagnosis with laboratory tests while ruling out other potential causes of hypocalcemia. Clinical symptoms include paresthesias, muscle cramps and spasms, carpopedal spasms, Chvostek's sign, Trousseau's sign, seizures, prolonged QT interval, arrhythmias, and generalized muscle weakness and fatigue. Laboratory values that support postoperative hypocalcemia include reduced serum ionized calcium and PTH levels. Vitamin D levels and renal function tests can be assessed to rule out other causes of hypocalcemia. Hypocalcemic patients often present with tetany, latent tetany, and seizures. Trousseau's sign can be elicited in patients with latent tetany on physical examination with a simple non-invasive maneuver [1].
In this case report, we present a young female patient with significant hypocalcemia complicated by multiple chronic conditions who demonstrated Trousseau's sign on initial physical examination. Hypocalcemia is a relatively common condition observed in hospitalized patients. It is imperative to not only treat hypocalcemia directly, but source determination can significantly alter the modality of treatment.
Case presentation
A 21-year-old woman with a history of hypoparathyroidism and Graves' disease was admitted to the hospital for evaluation of nausea, vomiting, and numbness in her hands and feet. The patient, who underwent a total thyroidectomy four months prior to admission, was on her eighth admission since the procedure. Her past medical history, recent surgery, and current presentation raised concerns about postsurgical complications and electrolyte imbalance. A carpopedal spasm was elicited while attempting to measure her blood pressure, indicating Trousseau's sign (Video 1).
Trousseau's sign
The patient's laboratory findings on admission are shown in Table 1.
Elevated liver aspartate aminotransferase (AST) and alanine aminotransferase (ALT) enzymes prompted an abdominal ultrasound, revealing a slightly echogenic appearance of the liver, suggesting hepatosteatosis.
The patient was diagnosed with symptomatic hypocalcemia, a postsurgical complication associated with total thyroidectomy. Upon admission, she began receiving intravenous calcium gluconate, and within the first 24 hours, the paresthesia in her hands and feet subsided. Although she continued to experience nausea at discharge, her vomiting episodes later resolved. To manage her nausea, the patient was prescribed 4 mg of ondansetron. While ondansetron has the potential to cause QT interval prolongation, which is also linked to hypomagnesemia [2], the patient did not exhibit any signs of QT prolongation (Figure 1).
Patient's 12-lead EKGEKG: electrocardiogram
The patient was admitted for 12 days, during which a few laboratory values were evaluated upon discharge. At that time, the patient's total calcium, 25-hydroxyvitamin D, thyroid-stimulating hormone (TSH), magnesium, potassium, creatinine, and albumin levels were all within normal limits. Although her aspartate aminotransferase (AST) and alanine aminotransferase (ALT) showed improvement, they remained elevated. The parathyroid hormone level remained unchanged, and a slight improvement was noted in the ionized calcium level, which still fell below the minimum standard (Table 2).
The patient was prescribed oral calcitriol 0.75 mcg twice daily and a four-week course of oral cholecalciferol 625 mcg once weekly. Upon discharge, the patient was noted to be relatively asymptomatic, with persistent abnormalities in ionized calcium, parathyroid hormone, AST, and ALT levels. A follow-up with her primary care physician was scheduled to ensure continuity of care and ongoing monitoring of her electrolyte levels and liver function.
Discussion
Trousseau's sign is a carpopedal spasm induced by inflating a sphygmomanometer cuff 20 mmHg above a patient's systolic blood pressure for three minutes and is commonly observed in hypocalcemic patients [3]. While Trousseau's sign may occasionally appear in healthy individuals, its sensitivity and specificity in hypocalcemic patients are 94% and 99%, respectively [4,5]. Calcium is the most abundant mineral in the body, and low levels of it can cause a plethora of symptoms. Many of the warning signs overlap with other conditions: dry skin, muscle cramps, and tingling in the fingers, toes, and around the mouth.
Post-thyroidectomy patients may be completely asymptomatic or may develop symptoms related to hypocalcemia. Symptoms include tetany, carpopedal spasms, perioral and or digital numbness, seizures, and QT prolongation [6-8]. It has been shown that postoperative vitamin D and calcium supplementation can significantly decrease the risk of transitory hypocalcemia [9] and its associated symptoms.
The patient's elevated liver enzymes and ultrasound findings suggest possible liver dysfunction that could reduce serum protein levels, resulting in less protein-bound calcium and decreased total serum calcium. However, normal albumin levels were confirmed upon admission and discharge, indicating that liver protein production remains adequate. Normal albumin levels lowered concerns about decreased calcium binding and total serum calcium. However, follow-up was recommended to monitor hepatic and calcium status.
Conclusions
In conclusion, due to the test's high sensitivity and specificity, Trousseau's sign is a common indicator of significant hypocalcemia. Patients with a history of total thyroidectomy should be monitored closely for continued fluctuations in calcium values due to postsurgical primary hypoparathyroidism. Patients should initially undergo calcium checks every 3-6 months. Depending on the outcomes, patients can transition to annual checks. Ultimately, a multidisciplinary approach is necessary to manage their condition correctly, thus reducing symptoms and increasing quality of life.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnosis and management of hypocalcemia Endocrine Pepe J Colangelo L Biamonte F 4854956920203236733510.1007/s 12020-020-02324-2 · doi ↗ · pubmed ↗
- 2Prolonged Q-Tc interval and decreased lymphocyte magnesium in congestive heart failure Magnesium Cohen L Laor A Kitzes R 16416831984 https://pubmed.ncbi.nlm.nih.gov/65135996513599 · pubmed ↗
- 3[Armand Trousseau (1801-1867), his history and the signs of hypocalcemia]Rev Med Chil Young P Bravo MA González MG Finn BC Quezel MA Bruetman JE 1341134714220142560112110.4067/S 0034-98872014001000017 · doi ↗ · pubmed ↗
- 4Trousseau's sign at the emergency department BMJ Case Rep van Bussel BC Koopmans RP 2016201610.1136/bcr-2016-216270 PMC 498600827481262 · doi ↗ · pubmed ↗
- 5Images in clinical medicine. Chvostek's and Trousseau's signs N Engl J Med Jesus JE Landry A 0367201210.1056/NEJ Micm 111056922970971 · doi ↗ · pubmed ↗
- 6Single intravenous dose ondansetron induces QT prolongation in adult emergency department patients: a prospective observational study Int J Emerg Med Rezaei Zadeh Rukerd M Shahrbabaki FR Movahedi M Honarmand A Pourzand P Mirafzal A 491720243856600810.1186/s 12245-024-00621-5PMC 10988934 · doi ↗ · pubmed ↗
- 7Rate of drop in serum calcium as a predictor of hypocalcemic symptoms post total thyroidectomy Osteoporos Int Saad RK Boueiz NG Akiki VC Fuleihan GA 249525043020193146358810.1007/s 00198-019-05040-4 · doi ↗ · pubmed ↗
- 8Hypocalcemia-induced QT interval prolongation Cardiology Tang JK Rabkin SW 19119514720223507820410.1159/000515985 · doi ↗ · pubmed ↗