A Review of the Prospective Effects of Methadone on Peripheral Neuropathic Pain in Diabetic Patients
Javad Poursamimi

TL;DR
This review examines how methadone affects neuropathic pain in diabetic patients, highlighting its potential benefits and mechanisms.
Contribution
The paper provides a comprehensive review of methadone's effects on diabetic neuropathic pain and its immunomodulatory mechanisms.
Findings
Low-dose methadone reduced visual analog scale (VAS) scores and serum glucose levels in diabetic patients.
Methadone increased N-chlorotaurine production, which supports innate immunity.
Methadone elevated levels of TNF-α, IL-1β, IL-2, and CD14+ monocytes in a dose-dependent manner.
Abstract
Peripheral neuropathic pain (PNP) is a significant complication for diabetic patients, often linked to poor glycemic control and elevated levels of glycosylated hemoglobin (HbA1c). High serum levels of cytokines, such as interleukin (IL)-6, and an increase in T-lymphocytes are crucial factors in developing neuropathic complications. Research suggests that substances like opiates and methadone can provide pain relief for these patients. This literature review is aimed at exploring the advantages and disadvantages of prescribing methadone to individuals with diabetes. We conducted a search of several databases, including PubMed, Google Scholar, Medline, Embase, Web of Science, and Scopus. We used keywords such as “diabetes,” “neuropathic pain,” “methadone,” “opioids,” “inflammation,” and “neuroimmunomodulation.” Ultimately, we identified 19 articles suitable for a more detailed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
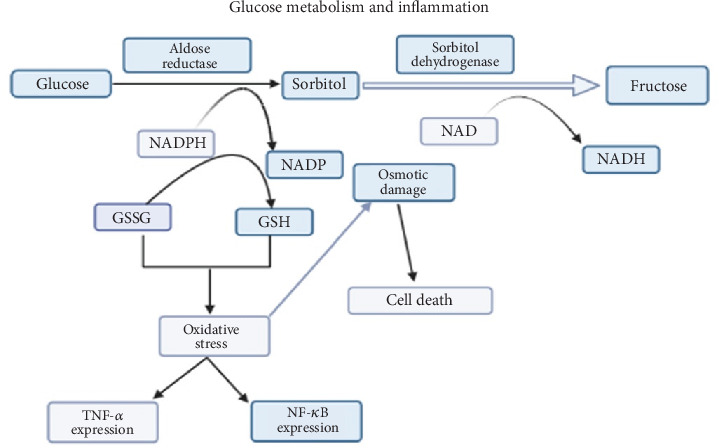 Figure 1
Figure 1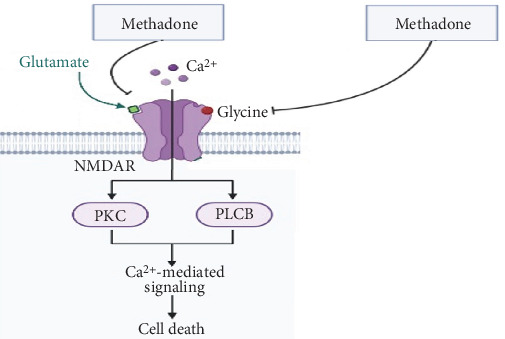 Figure 2
Figure 2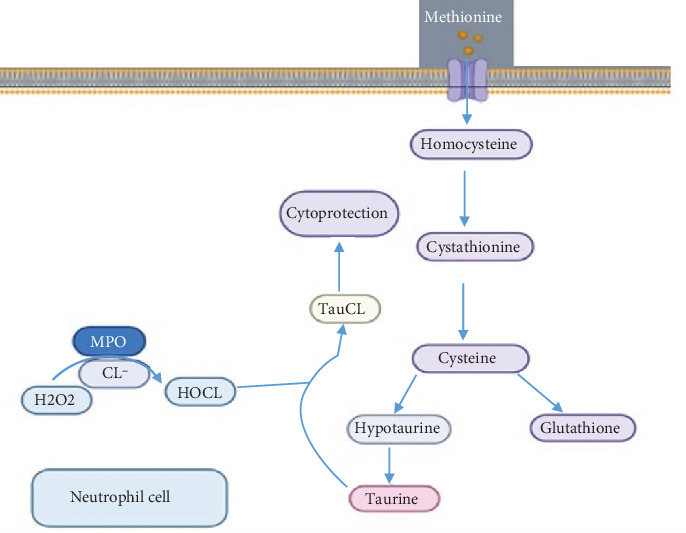 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAldose Reductase and Taurine · Pain Mechanisms and Treatments · Biochemical effects in animals
1. Introduction
Peripheral neuropathic pain (PNP) is a common complication that eventually affects all individuals with diabetes. Reports indicate that more than 2 million Americans suffer from PNP caused by diabetes [1]. Poor glycemic control and elevated glycosylated hemoglobin (HbA1c) levels are closely linked to complications [2, 3], making it essential for patients to manage these factors [4]. Additionally, hypertension, obesity, high blood lipid levels, and smoking are risk factors that can exacerbate symptoms in these patients [4].
As adipose tissue develops, macrophages (MQs) infiltrate it and release proinflammatory cytokines such as tumor necrosis factor alpha (TNF-α), interleukin-6 (IL-6), and interleukin-1 beta (IL-1β), which have harmful effects on the longevity of beta cells in the Langerhans islets [5–7]. When drug abuse occurs in diabetic patients, T helper 1 (Th1) cells work together with MQs to produce higher levels of TNF-α, IL-6, and IL-1β. On the other hand, an increase in T helper 2 (Th2) cells and serum levels of anti-inflammatory cytokines (such as interleukin-4 [IL-4]) is likely to reduce diabetic complications [7]. Nowadays, diabetics are considering the use of synthetic or natural drugs such as opioids like methadone and heroin to alleviate pain [5, 7, 8]. This is achieved through the binding of common receptors such as mu (μ), delta (δ), and kappa (κ) with their ligands like methadone [5]. In vivo studies have suggested that these receptors are also expressed in immune cells. However, their interaction with the μ receptor on immune cells can have antagonistic effects such as suppressing nuclear factor kappa B (NF-κB) gene expression, interferon (IFN)-γ secretion, and antibody production [7, 9]. On the other hand, intracellular synthesis of 3′,5′-cyclic adenosine monophosphate (c-AMP) and secretion of anti-inflammatory cytokines (interleukin-10 [IL-10] and IL-4) are induced [7].
The activity of opioid receptors is dependent on the dose. High doses lead to inhibition of adenylate cyclase and lower intracellular c-AMP levels. This can increase the expression of IFN-γ and NF-κB [10]. In this critical review, we aim to clarify these controversial findings.
2. Methodology
In this review, 52 articles were extracted from scientific electronic databases including Web of Science, Scopus, Embase, Google Scholar, and PubMed using keywords such as methadone, opiates, diabetes, neuropathy, peripheral neuropathy, immune system, cytokines, innate immunity, cellular immunity, signal transduction, and opioid receptors. Finally, 19 articles were found that can be used for more a precise examination (Table 1).
3. Methadone and PNP
The exact mechanism of PNP is unclear. However, the sensation of pain experienced differs from that of cuts or bruises. In neuropathy, damage to the nervous system is not caused by cuts or bruises but rather by a thickening of the capillary membrane in diabetes [27–31].
Microangiopathy or dysfunction of blood capillaries in diabetes may contribute to pain. This occurs when blood glucose levels are not controlled [29]. In such cases, metabolic pathways such as the sorbitol or polyol pathway, oxidative stress, and the production of proinflammatory cytokines are more activated [32] (Figure 1).
Glucose is converted to fructose through the two main enzymes, aldose reductase (AR) and sorbitol dehydrogenase (SDH), of the polyol pathway. When hyperglycemia occurs, the polyol pathway is overactivated, causing an increase in the body's fructose levels and resulting in more free radical production [33].
Some of the free radicals (related to oxidative stress) are synthesized by the enzymatic activity of the reactive oxygen species (ROS) complex in diabetes-induced hyperglycemia [34]. Furthermore, blood levels of free fatty acids (FFAs) and damaged macromolecules such as DNA, lipids, and proteins may also be elevated [34]. Conversely, the antioxidative activity of enzymes such as glutathione peroxidase (GPx) also decreases [35], while serum levels of IL-1β, TNF-α, and IL-6 increase [36] (Figure 1).
In the following, the sensitivity of adipose and muscular tissues to insulin is compromised. In addition to hyperglycemia, there is also an overactivation of the NADPH oxidase and the protein kinase C (PKC).
PKC leads to the activation of p38 mitogen-activated protein kinase (MAPK), extracellular signal–regulated protein kinase (ERK)-1 and extracellular signal–regulated protein kinase (ERK)-2, and NF-κB transcription factor, ultimately increasing the secretion of proinflammatory cytokines [36]. Overall, the pain levels of patients increase. The visual analog scale (VAS) index is typically used for pain assessment. When patients take methadone at a dosage of 2–5 mg daily, it may help alleviate pain and result in a decrease in the VAS score [11, 37]. Methadone occupies the binding sites of N-methyl-D-aspartate (NMDA) receptors related to the amino acids glycine and glutamate, as shown in Figure 2 [11, 38]. Compared to other medications, a low dose of methadone provides a more effective sense of pain control [9, 12, 39] (Figure 2).
4. Methadone, Glucose, and Taurine
Metabolism of the amino acid methionine ultimately results in the production of taurine, which plays a role in bile formation, cholesterol excretion, cell volume regulation, ionic transporter activity, inhibition of protein phosphorylation, and innate immunity, even during fetal and neonatal development [40]. Halogen derivatives such as hypochlorous acid (HOCL), produced by white blood cells, may have harmful effects on intracellular organelles. The effects can be neutralized when taurine is converted to N-chlorotaurine [41, 42]. The process of N-chlorotaurine production is illustrated in Figure 3.
If there is a defect in glucose metabolism, such as AR deficiency, sorbitol will accumulate. This accumulation can lead to taurine deficiency, which exacerbates diabetic complications [43]. Studies conducted in vivo have shown that taurine supplements can reduce inflammation in individuals with diabetes [44, 45]. Taurine possesses anti-inflammatory properties by lowering high serum levels of malondialdehyde (MDA), C-reactive protein (CRP), and TNF-α and enhancing the activity of antioxidant enzymes such as superoxide dismutase (SOD) and catalase (CAT) [43] (Figure 3).
In addition to diabetes, the sulfur-containing amino acid (taurine) is also secreted into the serum of other conditions including anoxia, myocardial infarction, hepatic encephalopathy, and diseases with osmotic changes. It is interesting to note that serum levels of taurine increase after opioids are taken [17].
Some in vivo studies have shown that methadone and other opioids, which share in the use of μ-opioid receptors, have different acts in terms of glycemia. This function was revealed in the use of methadone and tramadol compared with others such as codeine, hydrocodone, oxycodone, hydromorphone, morphine, and fentanyl [46, 47]. Pancreatic insulin release; suppression of counterregulatory mechanisms such as glucagon, epinephrine, and sympathoadrenal responses to hypoglycemia; and impairment of glycogenolysis and gluconeogenesis are some of the likely mechanisms [48]. Furthermore, serum levels of MDA, CRP, and TNF-α decreased, while the antioxidant activity of SOD and CAT increased [13, 22, 43].
5. Methadone and Osmoregulation
Extracellular and intracellular osmotic perturbations are critical problems faced by all cells leading to cellular swelling and shrinking. Membrane transport processes are essential functions that cells utilize to establish a balance between intra- and extracellular pressure [49]. Ion transport channels such as K^+^ and CL^−^ and Na^+^ and CL^−^ as well as organic osmolytes like polyols (sorbitol and myo-inositol), amino acids and their derivatives (alanine and taurine), and methylamines (betaine) play crucial roles in this process [49]. For instance, when the serum levels of myo-inositol and taurine increase in diabetics, cataracts may develop, as this is related to cellular turgescence in lens cells. Methadone consumption exacerbates the turgescence of lens cells by causing an accumulation of myo-inositol and taurine. This is due to the inactivation of enzymes such as hexokinase, phosphofructokinase-1, and pyruvate kinase, which play essential roles in glucose metabolism [14]. Conversely, heroin inhibits cellular turgescence and reduces neuronal destruction, unlike methadone [17].
6. Methadone and Overweight (Metabolic Syndrome)
Although the prevalence of metabolic syndrome has been estimated to be high in heroin or methadone addicts, it also depends on the region, whether it is an urban or rural setting, and the population composition in terms of sex, age, and ethnicity [50]. It is evident that there is a close association between opioid intake, being overweight, and impaired glucose metabolism [19]. The overweight condition in opioid addicts is often due to consuming excessive amounts of sweets, which can also be linked to keeping opioid receptors and channels, such as G protein receptors and ion channels, open. Additionally, methadone can lead to weight gain by activating the μ receptors [15, 19].
7. Methadone and Sexual Dysfunction
Some sexual dysfunctions, such as low serum levels of testosterone and erectile dysfunction, are commonly observed in subjects taking morphine or methadone [16]. However, some studies have shown that erectile dysfunction in nondiabetics who have taken methadone is not related to serum testosterone levels. This may occur in a dose-dependent manner, so that after reducing methadone consumption, erectile dysfunction improves [18]. Additionally, other factors such as age, hormones, duration of treatment, medical and psychiatric status, and familial conditions can affect erectile function [51].
8. Methadone and Immunologic Functions
In a clinical trial involving outpatients with heroin abuse and low immune function, researchers discovered low concentrations of plasma levels of TNF-α, IL-1β, and interleukin-2 (IL-2) and a low number of monocyte CD14^+^. However, after administering methadone, these factors increased [25]. One of the chemokine receptors found on monocyte cells is CCR5, and it serves as a cofactor in enhancing the pathogenesis of HIV. Studies have shown that individuals who have substance abuse issues or use methadone tend to express high levels of CCR5 on monocytes and dendritic cells. As a result, they often display severe symptoms of HIV infection. This is likely due to the dose-dependent nature of methadone [52]. An in vivo study on the effects of methadone on experimental autoimmune encephalomyelitis (EAE) revealed a reduction in Th1 and T helper 17 (Th17) cell infiltration in the spinal cord, as well as a decrease in levels of IL-2, interleukin-17 (IL-17), IFN-γ, and IL-6 in the serum. Conversely, levels of anti-inflammatory cytokines like IL-4 increased [21].
The use of methadone caused a shift in the balance of Th1 to Th2 cells and their respective cytokines. This shift led to a decrease in inflammatory cytokines such as TNF-α and matrix metalloproteinase-9 (MMP-9), as well as an increase in the gene expression of anti-inflammatory cytokines and antioxidant enzymes such as CAT and SOD [22].
There are close relationships between hyperglycemia, ischemia, and oxidative stress in diabetic neuropathic pain (DNP). Ischemia occurs as a result of reduced blood flow to the tissue [53]. Reduced peripheral nervous perfusion leads to the release of capillary plasma proteins into the endoneurium, a delicate connective tissue layer surrounding the myelin sheath, causing an increase in capillary wall thickness. This process can lead to hyalinization of the vessel basal lamina and nerve ischemia [54], which can be inhibited using methadone. Therefore, methadone has the potential to reduce the risk of nerve ischemia in diabetes [20]. These conflicting results may be attributed to the dose-dependent manner of methadone.
In general, maintaining homeostasis in diabetes requires the apoptosis process. However, when it is overactivated, it can damage the body. Decreased expression of the BCL-2 gene is a key factor in the apoptosis pathway [55], which may be triggered in monocytes, CD4^+^ T cells, and CD8^+^ T cells using methadone [55].
One of the main components of the immune response is antigen-presenting cells [56], which are weakened in individuals who use opioids [23]. This can lead to low lymphoproliferation and an imbalance in the Th1/Th2 ratio in heroin addicts compared to methadone users [23]. The differentiation, maturation, and activation of dendritic cells are disrupted in opioid addicts [24].
9. Methadone and Its Interactions With Other Drugs
The way methadone is processed by the body varies significantly from person to person. Even when given the same dose, different individuals will have different concentrations of methadone in their system. As a result, some patients may not experience enough of the intended effects, while others may have too strong and prolonged of a reaction. Methadone is mainly broken down in the liver to an inactive form. Several cytochrome P450 enzymes are involved in methadone metabolism: CYP3A4, CYP2B6, and CYP2C19. Specifically, certain antiretroviral drugs can lower the levels of methadone in the body. The known drug interactions that affect how methadone is processed usually do not pose life-threatening risks to patients. However, they often lead to lower drug concentrations and effects [57]. The classes of drugs that may be used during methadone maintenance treatment and could potentially interact with methadone include benzodiazepines, antidepressants, anticonvulsants, macrolide antibiotics, and antifungals. Some of the most common ones are listed in Table 2.
10. Summary and Conclusions
This study was designed to investigate the effects of methadone on immune responses and signal transduction pathways in diabetic patients. In summary, methadone and other opioids have a variety of effects on the immune system. These effects included the conversion of Th1/Th2 balance to Th2, enhancement of cytokines, reduction of IFN-γ and NF-κB expression, and induced intracellular c-AMP synthesis at low opioid and methadone doses. Additionally, there was a decrease in the VAS index, an increase in N-chlorotaurine production in leukocytes, and a decrease in serum glucose levels with low doses of methadone. Other functions of low-dose methadone included amelioration of spinal cord disease and reduction of infiltration of Th1 and Th17 cells into the spinal cord. Methadone and low-dose opioids had anti-inflammatory effects by lowering serum levels of biochemical enzymes such as glutathione (GSH) and mediators (TNF-α, MMP-9) and normalizing dendritic cell function.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tesfaye S. Advances in the management of diabetic peripheral neuropathy Current Opinion in Supportive and Palliative Care 20093213614310.1097/SPC.0b 013e 32832 b 7df 52-s 2.0-6765123562619421063 · doi ↗ · pubmed ↗
- 2Argoff C. E. Cole B. E. Fishbain D. A. Irving G. A. Diabetic peripheral neuropathic pain: clinical and quality-of-life issues Mayo Clinic Proceedings 2006814 S 3S 1110.1016/S 0025-6196(11)61474-216608048 · doi ↗ · pubmed ↗
- 3Casadei G. Filippini M. Brognara L. Glycated hemoglobin (Hb A 1c) as a biomarker for diabetic foot peripheral neuropathy Diseases 202191 p. 1610.3390/diseases 9010016 PMC 800604733671807 · doi ↗ · pubmed ↗
- 4Tesfaye S. Chaturvedi N. Eaton S. E. M. Vascular risk factors and diabetic neuropathy New England Journal of Medicine 2005352434135010.1056/NEJ Moa 0327822-s 2.0-1994443369415673800 · doi ↗ · pubmed ↗
- 5Liou J. T. Liu F. C. Mao C. C. Lai Y. S. Day Y. J. Inflammation confers dual effects on nociceptive processing in chronic neuropathic pain model Anesthesiology 2011114366067210.1097/ALN.0b 013e 31820 b 8b 1e 2-s 2.0-7995204340021307767 · doi ↗ · pubmed ↗
- 6Tzanavari T. Giannogonas P. Karalis K. P. TNF-α and obesity Current Directions in Autoimmunity 20101114515610.1159/0002892032-s 2.0-7794944262120173393 · doi ↗ · pubmed ↗
- 7Amirshahrokhi K. Dehpour A. R. Hadjati J. Sotoudeh M. Ghazi-Khansari M. Methadone ameliorates multiple-low-dose streptozotocin-induced type 1 diabetes in mice Toxicology and Applied Pharmacology 2008232111912410.1016/j.taap.2008.06.0202-s 2.0-5154910275918671992 · doi ↗ · pubmed ↗
- 8Hays L. Reid C. Doran M. Geary K. Use of methadone for the treatment of diabetic neuropathy Diabetes Care 200528248548710.2337/diacare.28.2.4852-s 2.0-1284425490915677822 · doi ↗ · pubmed ↗