Running-Centred Injury Prevention Support: A Scoping Review on Current Injury Risk Reduction Practices for Runners
Linda Linton, Jane Culpan, Judith Lane

TL;DR
This review explores injury prevention strategies for runners, highlighting the need for individualized, supported approaches and the gap between expert advice and runner behavior.
Contribution
The study maps current injury risk reduction practices for runners and identifies key themes and disparities in expert and runner perspectives.
Findings
Supervision and support are critical for effective injury prevention in runners.
Key strategies include strengthening, gait re-education, wearables, and graduated running programs.
Runners often rely on self-efficacy rather than expert advice for injury risk reduction.
Abstract
Background: Runners have not benefited from the same reduction in injury rates seen in injury prevention studies conducted in other sports. Objectives: The purpose of this scoping review was to identify and map injury risk reduction practices for running-related injury (RRI), methods of delivery and understand the views of experts and runner's preferences in reducing RRI. Design: Scoping review. Methods: We conducted systematic database searches of MEDLINE, CINAHL and SPORTDiscus from 2000 to April 2024. Eligible studies included injury prevention strategies for RRI. Data synthesis was conducted according to PRISMA Extension for Scoping Reviews using Joanna Briggs Institute framework methodology. Extracted data were mapped and coded from intervention studies, expert opinions and reviews, and inductive thematic analysis created subthemes and themes from prospective cohorts,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
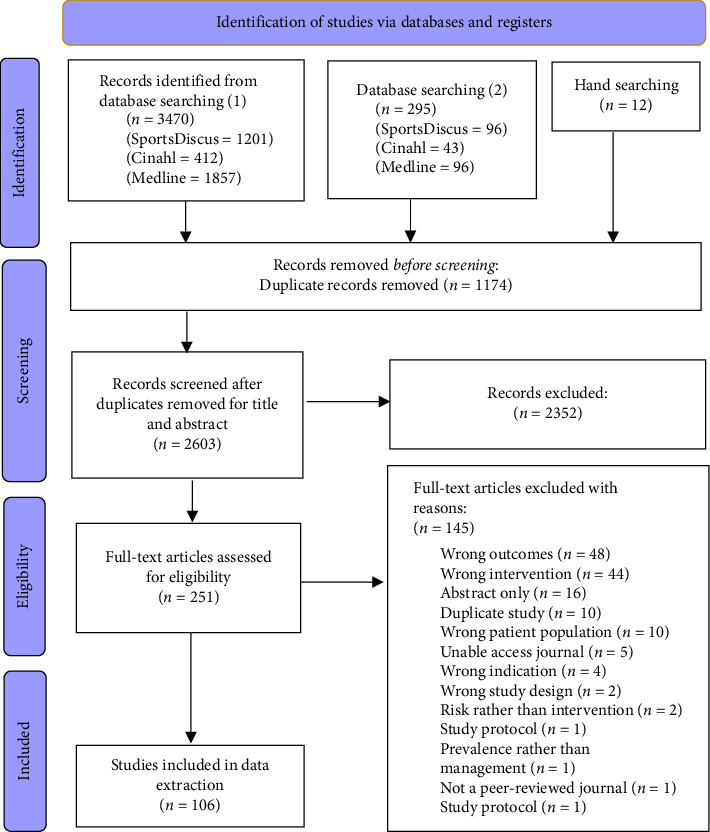 Figure 1
Figure 1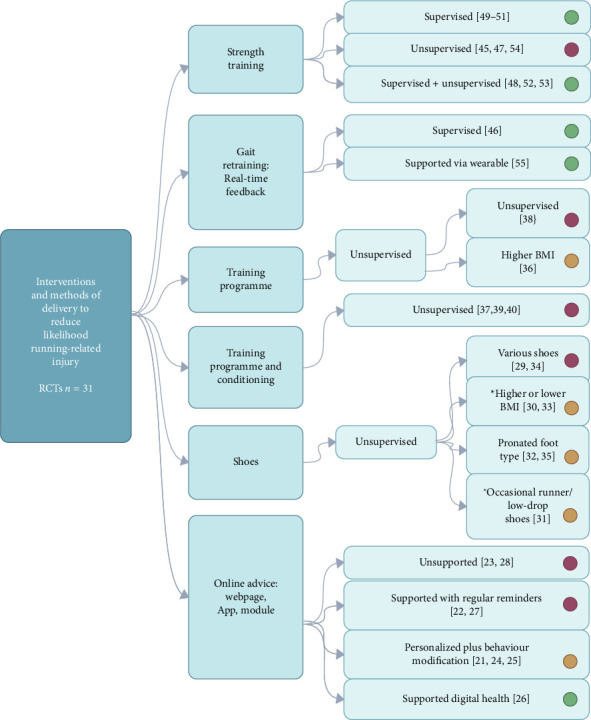 Figure 2
Figure 2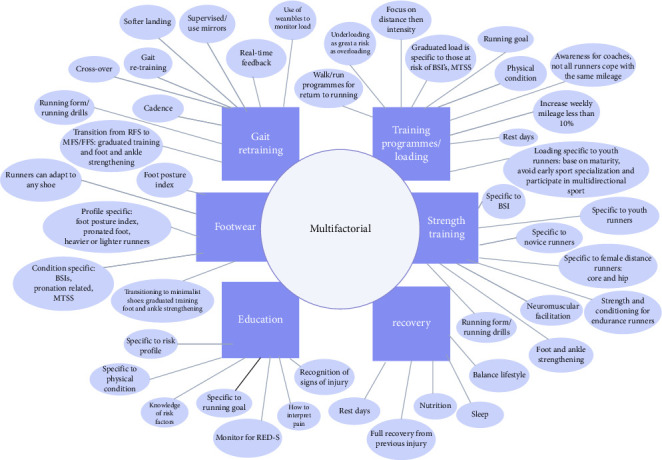 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLower Extremity Biomechanics and Pathologies · Sports injuries and prevention · Winter Sports Injuries and Performance
1. Introduction
Current injury risk reduction strategies for runners have had a variable impact on reducing overall running-related injuries (RRIs), with the incidence of injuries still higher than in most sports [1]. Risk factors for RRIs include relationships between runner's health, biomechanics, physical conditioning, running environment and training habits, current and previous experience, and behaviours [2]. This range of influences poses difficulties in determining an approach to injury risk reduction practices, where RRIs are predominantly overuse [1, 3], and the aetiology of injury follows a causal framework where loading alone cannot be responsible for injury without considering an interplay of factors such as runner's capacity for load [4, 5]. Additionally, runners have personalized responses to perception of pain, or views on risk which are both dependent on multiple influences characterized by current understanding of biomedical and biopsychosocial models of pain [6, 7] therefore may struggle to interpret and respond to symptoms. Indeed, runners report a range of sensations before classifying themselves as “injured” and describe injury only when they have got to the point of needing a consultation with a healthcare professional (HCP) or cessation of running [8]. This can make it hard for ‘uninjured' runners to engage with injury risk reduction practices. Footballers experiencing discomfort not affecting training were 2.8–5.9 times more likely to sustain a time loss injury the following week [9]. Therefore, having knowledge to intervene prior to this stage and ‘prevent' injury escalating is likely beneficial for injury risk reduction in runners, but very few studies explore runner's behaviours and beliefs [10, 11].
Exercise-based injury prevention programmes (IPPs) in particular have been highly successful across a range of sports and are effective at reducing the risk of injury on average by 29%, but generally not found effective if delivered as an unsupervised intervention [12]. Lauersen, Bertelsen, and Andersen reported a 47% reduction in overuse injury with IPPs implemented across a range of sports, but the overuse injuries reported were predominantly with military participants and no running-specific studies were included in their analysis [13]. Similarly, other studies have found a lack of conclusive evidence for the effectiveness of IPPs designed to address risk factors in runners [14], in endurance runners [15], and for knee injuries [16]. Wu et al. found only three out of nine studies conducted with endurance runners had supervised IPPs, although compliance was higher in these interventions [15]. The majority of supervised IPPs are in team sports [12, 13], where the training environment is supervised by coaches who can influence team participation in IPPs and enhance compliance with injury risk reduction practices [17, 18]. Other factors such as load monitoring can be controlled in team environments through technology such as GPS and coaching plans [19]. Runners participating in differing environments with individual risk profiles, abilities, running goals and beliefs may make universal injury risk reduction interventions more difficult to disseminate and adhere to [20]. Due to these difficulties in supporting exercise-based approaches for runners, running injury prevention research has adopted other approaches such as advice only [21–28], footwear-specific [29–35] and graduated training programmes [36–40]. Despite this growing body of research utilizing strategies other than IPPs, there has not been a reduction in RRI like the results seen with IPPs in other sports with over half of runners reporting RRI in a recent survey conducted over an 18-month period in 87 countries [41].
The plethora of different types of injury risk reduction practices coupled with the complexity of RRIs and the diversity of runners [4, 5] provide difficulty in navigating the literature and identifying the direction of future research and dissemination of injury risk reduction practices to runners. Therefore, this scoping review aimed to collate literature on injury prevention strategies used with runners and establish the types of interventions which have been implemented or discussed in the literature to reduce the risk of injury. To provide context to current research, a secondary aim sought to explore how these strategies have been delivered to and received by runners, and what views other stakeholders and experts consider as best practice. The objectives were to review the literature to (i) identify current types of interventions that have been used in the literature for injury risk reduction in runners, what methods have been used to deliver these strategies to runners and what effect have they had (ii) understand experts' knowledge and recommendations on injury risk profiles for reducing risk of RRI, and (iii) explore the behaviours, and beliefs of runners and other stakeholders for what they view to be effective and the factors influencing this. Findings can influence future RRI risk reduction practices for HCPs, runners and other stakeholders.
2. Methods
Scoping review methodology was chosen to review current knowledge and practice within this emerging body of literature on injury risk reduction practices and methods of delivery. This provides a broader and deeper understanding not just of current literature from researchers and experts, but the ability to encompass the views of the main stakeholders the runners themselves, running coaches and HCPs, and was conducted according to the Preferred Reporting Items for Systematic Reviews and meta-Analyses extension for Scoping Reviews (PRISMA-ScR) statement [42] and used the Joanna Briggs Institute (JBI) framework methodology for scoping reviews as described by Peters et al. [43]. The scoping review protocol was discussed by all three authors and registered and published on 30th June 2023 with Open Science Framework (OSF) (https://osf.io/2jtqn).
2.1. Literature Search Strategy
Prior to the main search and on advice from the University Librarian, a preliminary search was conducted using the database EMBASE to develop keywords and phrases. The final literature search was conducted from inception to July 2023 and then updated from July 2023 to April 2024 through databases MEDLINE, CINAHL and SPORTDiscus. Details of search strategy, subject headings and keywords can be found in Supporting File 1. All citations were uploaded onto the platform Zotero (version 6.0.13), and duplicates were removed. The remaining studies were uploaded to Covidence (https://www.covidence.org/) for screening.
2.2. Study Selection
Titles and abstracts were independently screened by two authors (L.L. and J.L.). Criteria for inclusion were set as follows: any type of running, any age, English language, RRI prevention all interventions, RRI prevention all methods of delivery and all stakeholders involved with injury risk reduction in runners such as coaches and HCPs. Literature included could be in the form of studies directly related to RRI prevention approaches. Research studies such as surveys, randomized controlled trials (RCTs), cross-sectional and longitudinal cohort studies and qualitative studies were all considered, alongside reviews, and papers such as reports, commentaries, editorials and opinion pieces. The exclusion criteria included animal and military studies, and reviews which included studies with participant groups other than runners such as the military. Studies focusing only on risk factors that focus on the management of injury rather than injury prevention or epidemiology studies not directly related to injury prevention interventions or prevalence were excluded. A third reviewer (J.C.) was on hand for discussion should any disagreement arise.
On completion of abstract and title screening, full-text studies were retrieved by L.L. and assessed for eligibility by two reviewers (L.L. and J.L.) using the inclusion and exclusion criteria. Reasons for excluding ineligible studies were recorded, and if consensus could not be made at this stage, a third reviewer (J.C.) was available to be consulted.
2.3. Data Extraction
A form was developed and customized for the purposes of this study on Covidence to record data extracted from each of the studies. The entities agreed for data extraction were as follows: author and year of publication, type of study or methodology, type of running, study participants' age and sex. For prospective longitudinal and retrospective intervention studies and cross-sectional studies, injury prevention interventions and the type of injury(s) the study aimed to collate, the methods of delivery and efficacy were extracted. For surveys and qualitative studies, reviews, expert opinion papers, editorials, and systematic reviews and meta-analysis, the main themes and outcomes were recorded. All three authors (L.L., J.L. and J.C.) independently extracted all entities for 10 studies to ensure consensus was reached for all information recorded and to assess the practicality of the customized form on Covidence. Following this, two data extractors (L.L. and J.L.) independently extracted data from all remaining studies and met to discuss those studies that Covidence highlighted as having a conflict of agreement. At this stage, reference lists from the current studies were hand-searched for any remaining sources to be added to the data extraction stage.
2.4. Data Charting
On completion of data extraction and agreement between extractors L.L. and J.L., all data extracted were uploaded from Covidence to Excel (Microsoft Office Professional Plus 2016) for data synthesis. The primary goal was to analyse studies and chart the data for injury prevention strategies, their methods of delivery and establish views of researchers, runners, HCPs, experts and other stakeholders, and ensure all involved parties' engagement, beliefs and participation and role in injury risk reduction for runners were captured. Due to the diversity in the literature, there is no generic quality assessment tool available that was deemed as applicable, and assessment of quality is not considered essential for a scoping review [43]. However, to provide context to the level of quality of intervention studies, the Physiotherapy Evidence Database (PEDro) scale (https://pedro.org.au/) was used to assess the methodological quality of all RCTs.
Three summary tables were compiled to improve the ease of analysis based on the study design. Each group was analysed separately in order to adequately interpret and map data. Group 1 studies comprised RCTs and were analysed for the type of injury risk reduction strategy used during the intervention, and whether the method of delivery was supervised or unsupervised. Based on the type of intervention and method of delivery, the outcome was summarized as either effective and reduced injury (coded green) or not was not effective at reducing injury (coded red). If the outcome between studies with the same method of delivery of the intervention did not agree between studies (effective and reduced injury/not effective at reducing injury), or the findings reported there was some effect from subgroup analysis, the outcome was coded neutral or undecided (amber). Group 2 studies were narrative reviews, editorials, opinion papers, commentaries, and systematic reviews and meta-analysis and were analysed deductively where initial themes were developed based on the themes or entities which had arisen from Group 1 on interventions recommended for injury prevention. Mapping and grouping these themes guided corresponding attributes or subthemes which emerged from the data and were collated. This approach is described elsewhere by Naem et al., as a ‘top-down approach', guided by existing theories (current interventions) [44]. Group 3 included feasibility studies, cross-sectional and prospective and retrospective longitudinal cohort studies, qualitative studies and surveys. Thematic analysis was used for this group following an inductive approach. Summarized outcomes of studies provided codes which created subthemes, and themes emerged, allowing the runners and other stakeholders a voice and aligning with a constructivist paradigm and therefore deeper exploration of the data [44].
3. Results
The literature search identified 3470 potential studies from January 2000 to July 2023. After duplicates were removed, 2388 studies underwent title and abstract screening excluding a further 2170 studies, leaving 218 studies to undergo full-text screening. A total of 99 studies were eligible for data extraction which included 12 from hand-searching. The second literature search conducted included 295 studies from July 2023 to April 2024. After duplicates were removed and studies excluded during title, abstract and full-text screening, a further 7 studies were included in the final review. This provided 106 studies in total for analysis. Figure 1 illustrates an overview of this process and details reasons for full article exclusions. Specific exclusions include abstracts (n = 16) published for conferences only, and when unable to access a journal, the corresponding author was contacted via email. If there was no reply following a reminder email, the study was excluded (n = 5).
Studies were categorized into three groups for data visualization and analysis and summarized in Tables 1-3 (full details of data extraction can be found in Supporting File 2, and quality assessment for Group 1 studies in Supporting File 3). Overall, intervention studies, reviews and expert opinion papers focused on novice or recreational runners. Elite runners tended to be youth, collegiate or younger adults.
3.1. Types of Interventions and Methods of Delivery for Injury Risk Reduction in Runners
Group 1 had 31 RCTs, with a total of 14,414 participants: 6878 were females (48%), ranging from 22 to 4050. Mean age of overall runners was 35.45 years (age range 12.8–48.2). A variety of techniques were used to distribute information and facilitate interventions throughout each study. In brief, interventions either included some level of supervision or digital support from the project teams, or the participants self-managed with minimal face-to-face interaction or remote support. Each RCT investigating an intervention for injury risk reduction focused on individual injury risk practices. Strength training was delivered as either supervised sessions [48–53] or programmes were provided for participants to perform independently [45, 47, 54]. Gait retraining studies used real-time feedback to facilitate change and were either supervised [46] or provided through digital feedback via wearables [55]. Graduated training programmes were predominantly unsupervised [36–40]. Footwear studies provided shoes for participants, and they trained independently with no further supervision [29–35]. Online interventions varied with some providing access to the website or app that had generic information for the participants to access independently throughout the study [22, 23]. Others provided regular reminders to access the website or app using techniques via email reminder or newsletter [25, 27]. Others used online techniques to establish individual profiles of the runners and tailor their information to their specific needs [21, 24, 27]. Another study provided online modules on digital health for participants to access and, as this was in youth runners, parents were involved in accessing information [26]. Studies collated RRI as all injuries related to running [21, 26–29, 34, 36, 39, 40, 46, 49, 52, 54, 55], injuries of the lower extremity [25, 33, 48, 51], lower extremity and lower back [22, 23, 30, 32, 35, 37, 38, 45, 47, 50, 53] and all injuries related to running, integumentary systems and concussion [24]. Only one study intervention specifically targeted an injury type and anatomical area, and this was ankle injuries [48]. Types of interventions, their methods of delivery and levels of effectiveness are summarized in Table 1 and illustrated in Figure 2. We excluded Kemler, Cornelissen and Gouttebarge from Group 1 analysis as they did not report an injury rate Kemler et al., [122], and details of this study have been summarized in Table 3.
3.2. Opinions of Experts, and Reviews and Best Practice for Injury Risk Reduction
Strategies described by experts for injury risk reduction were summarized in Group 2 studies, and themes are mapped and coded in Table 2. There were 20 expert view/editorial/opinion papers, seven narrative reviews, five reviews, four systematic reviews with meta-analysis, two commentaries, one Cochrane review and one scoping review. Themes were initially influenced by interventions used in RCTs but closer inspection of Group 2 studies revealed recovery, and education as 2 further entities. Six entities or themes related to injury prevention strategies emerged: gait re-education [5, 16, 56, 57, 60, 63–66, 73, 75–77, 80, 83, 85–89], training/loading [5, 16, 20, 56, 57, 60, 62–64, 67–69, 74–78, 81, 84, 85, 87–89], footwear [16, 56, 60–62, 68–77, 82, 86, 123], strength training [11, 15, 56, 58–64, 66–69, 78–80, 82, 86–88], education [5, 11, 56, 60, 70, 72, 73, 78, 79, 82, 85–88] and recovery [5, 11, 20, 60, 69, 76, 78, 79, 88]. Corresponding attributes or subthemes from each theme detail experts' conclusions and influencers for strategies for the reduction of RRI. Overall, most studies advocated a multifactorial approach of more than one strategy to reduce the likelihood of RRI. The visualization of themes and subthemes is illustrated in Figure 3.
3.3. Influencers for Injury Risk Reduction Practice
Group 3 comprised 14 surveys, 10 prospective cohort studies, six qualitative studies, two feasibility studies and one RCT, retrospective cohort study and cross-sectional study. The views and perspectives of runners and a range of key stakeholders are summarized in Table 3. Themes emerged as follows: guidance and supervision, education, technology, beliefs behaviours and self-efficacy, and injury risk profiles. These provide depth to the contextual factors involved in the delivery of injury prevention intervention and specific drivers influencing implementation.
In summary, coaches and HCPs are in the position to provide education to runners [96–103, 122], with guidance and supervision recommended for facilitation [90–95]. Coaches look to HCPs for advice on best practice on injury risk reduction practices [93], and runners look towards HPCs, coaches, running stores or online sources for information [98, 100, 101, 103, 122]. Knowledge on the purpose and benefits of specific injury risk reduction strategies is likely to provide enhanced benefit [95, 97]. Not all runners train with a coach, but welcome a group environment with a professional to seek further education [100]. Despite access to coaches and HCPs, runners exhibit behaviours and beliefs which underpin their choices and veer towards passive, accessible strategies [10, 106, 107, 109–113]. HCPs should respect a runner's autonomy but can support a runner's decision-making [108, 111], and technology could be an area runners may adopt for injury prevention that could provide self-efficacy but needs to provide personalization [104, 105, 108]. As runners have specific unique injury risk profiles, identifying and responding to these when choosing or incorporating IPPs and advice could enhance a runner's response to injury [114–121, 124].
4. Discussion
This scoping review found injury prevention approaches for the reduction of RRI have different outcomes dependent on methods of facilitation. Interventions such as strength training are more effective when supervised, and support plus behaviour modification is needed when runners are provided online educational advice. In addition, runners have an individual injury risk profile, and this may be in part why generic, singular IPPs for large cohorts of runners have had limited effect to date. For example, footwear appears to be most effective for specific foot type, and higher or lower BMI, and a graduated training approach was only found beneficial for a specific cohort of runners with higher BMI. Our results found a disparity between current research and the views of experts, with experts favouring a multifactorial approach to injury risk reduction strategies. There is generally more engagement from previously injured runners, and thus, future research must aim to make all runners the centre of injury risk reduction practice with their views and preferences helping shape best practice. Promising injury risk reduction strategies recommended by experts such as recovery and gait re-education need more robust investigation, but may be more appealing to runners as they require the least time or effort to adopt and have a limited impact on other parts of daily life.
4.1. Runner's Behaviours on Injury Risk Reduction
Supports or shoes are frequently chosen by runners for injury risk reduction [10, 96, 97, 106, 107, 112, 124]. They provide minimal impact on training habits and are dependent on a runner's injury risk profile, and some studies have found shoes effective in reducing injury [30, 33, 35]. Shoe choice is personalized to individual runners, and this demonstrates behaviours of autonomy and motivation for injury prevention as described by Chan et al., which is important for health and well-being [125]. Despite demonstrating self-efficacy with choosing running shoes and high compliance rates in studies in comparison with other injury risk reduction interventions [74], we found runners lacked knowledge or ignored “additional” measures advised when adapting to minimalist shoes [56, 64, 66, 67]. Therefore, runners have confidence in choosing shoes but may not necessarily make time for supplementary actions. A survey on runners and expert's knowledge on running shoes found their views changed after completing an online module [97], highlighting the value of education in ensuring an understanding of best practice on footwear, reasons for change and how to transition safely.
The current scoping review found gait retraining was frequently advocated by expert opinions, reviews and qualitative studies, and runners expressed that this is a strategy they would like to incorporate into their running to reduce the risk of injury [5, 16, 56, 57, 60, 63–66, 73, 75–77, 80, 83, 85–89, 92, 100]. With only two RCTs to date on the effect of gait re-education for the reduction of RRI [46, 55], more research is needed in this area. Easy application of running cues may be especially appealing to novice runners inexperienced in running [126], or developing a comfortable running style similar to running shoe comfort may positively influence engagement with gait re-education techniques [75]. With advances in wearable technology for gait retraining, this digital form of feedback providing runners with motivation and load monitoring may demonstrate improved compliance with interventions in future studies and influence long-term adherence thereafter [105]. However, one study reported wearables increased RRI by inducing competitiveness and influencing poor decision-making, highlighting wearables should also provide personalized support to reduce risk-taking behaviours [104].
4.2. The Effect of Supervision and Support for Injury Risk Reduction
Runners are keen to adopt strategies such as shoes, supports and gait re-education which are easy to implement within running training, and also invest extra time on stretching despite a lack of evidence of an effect on injury rate [112, 113, 127, 128]. In contrast to stretching, there is some efficacy for strengthening which runners claim to know, but knowledge alone is not enough to influence behaviour [100]. Focusing on strategies to overcome the obstacles such as reminders, monitoring and providing support has been shown to be more effective in influencing behaviours [129]. This concurs with findings from this current study where strength training was only effective as a supervised programme [48–53]. Runners may be open to replace stretching with strengthening if they know why experts recommend this for reducing the risk of RRI [11, 15, 56, 58–64, 66–69, 78–80, 82, 86–88], and have access to educational workshops or runner-specific strength training [10, 100], or can participate in a running group where coaches are able to incorporate strength training into a warm-up [93, 101].
Educating running coaches to utilize coaching skills to influence behavioural change in runners could be beneficial for implementing injury risk reduction practices, especially as runners conversely look to coaches for advice [93, 103]. This has previously been trialled with workshops for coaches in other sports to improve the dissemination of exercise-based IPPs [130]. Coaches are highly influential for athlete's knowledge and beliefs, therefore ensuring that coaches are engaged with the concept of injury prevention and equipped with best practice using a ‘train-the-trainer' approach has been recently highlighted in the literature [131]. Future research should focus on ways of facilitating runners to engage with running groups, an online community, organized workshops or supported digital health modules.
4.3. Specific Injury Risk Profiles and Education
In other sports, IPPs have been tailored to target injuries such as hamstring injuries [17], but only one intervention study discussed in this scoping review targeted a specific injury: ankle injuries in orienteers [48]. Runners too have risk profiles for specific injuries such as BSIs [88], but our current study found a lack of research on condition-specific or runner-specific programmes. Youth distance runners are a running cohort where experts endorse specific practices to reduce RRI such as strength training, avoiding early specialization in distance running and ensuring runners perform multidirectional sports [69, 82, 88, 91], particularly in females, who are at higher risk of experiencing changes to bone architecture during youth leading to bone health problems in later life [88, 118, 121, 132, 133]. With only two RCTs in this youth age group, there is scope for further research [26, 51]. One study disseminated a digital health intervention and involving everyone in the youth runner's welfare showed that an approach providing a wider support group was effective in injury risk reduction [26]. This particular study included participants from 12 to 15 years old, and although Tenforde et al. defined the youth runner as any age below 18 years old, most injuries appear to be reported between ages 12 and 14 highlighting specific needs at this age as critical for longevity in running [82]. Similar to youth sport, there is a dearth of RRI risk reduction intervention studies on elite runners [48, 60, 94], possibly reflective of a smaller, younger cohort, with easier access to support staff but potentially different needs. We found experts advocated benefits of recovery in both elite and recreational running such as sleep, balancing lifestyle, rest days, nutrition and ensuring full recovery from injury [5, 11, 20, 60, 69, 76, 78, 79, 88], but it is not clear from runners how often they utilize such practices, especially as these often occur out with actual running training and future studies should try to capture this information. As there are complex reasons, runners engage with running [134], providing runners flexibility to adapt training and recovery within daily life and gaining understanding of runner's viewpoints may improve compliance [134].
There is minimal research on the effects of educating runners on injury definition despite studies in this scoping review reporting this is important [5, 11, 56, 70, 79, 85, 87, 88]. As identified in this scoping review (Table 1), studies investigating interventions to reduce the likelihood of RRI had different criteria on defining RRI location, and therefore, agreement is needed between researchers on what is classified as an RRI. Runners in turn have a different understanding of when they should respond to pain based on their interpretation that they are only injured if needing to seek professional help or are unable to run [8]. Yet, intervening prior to the cessation of running may prevent further injury. Education on pain monitoring tools for adapting training loads in response to pain has been suggested in the literature as a strategy to reduce likelihood of RRI [93, 135, 136]. It appears experienced runners have more strategies than novice runners to adapt and flex their training programme in response to musculoskeletal pain [137], which novice runners lack awareness of [115, 119, 138]. Interestingly, graduated running programmes on their own have had little traction in reducing RRI risk for runners new to running, with no clear benefit for shorter or longer walk-run training programmes [36, 38, 115, 119], or with additional conditioning [37, 39, 40]. With new runners having different responses to loading dependent on body weight, age, running pace and previous injury [36, 37, 40, 114, 115, 119], this highlights the need for further research to investigate the effect of a multifactorial approach involving personalized running programmes and education.
Researchers have shown promising developments with online tailored programmes, but only if individualized, and provide reminders. The use of outcome measures for behavioural modification in response to educational interventions appears promising [11, 21, 24, 28]. Runners rarely access content unless injured [23, 25] and generally show more interest and investment in injury reduction practices than noninjured runners, reflecting their injury never fully resolved and they seek prehabilitation as a means for rehabilitation [100, 107]. As the previous injury is a strong predictor for future injury and with approximately 50% of runners currently running with some elements of discomfort [41, 139], giving runners support with strategies that are evidence-based and easily incorporated into usual running training will help aid longevity with running. Therefore, all determinants and injury risk profiles need to be considered when engaging in a new activity particularly running, with appropriate supported education given alongside a graduated running programme.
4.4. Limitations
This scoping review is one of the first to consider the wide range of injury prevention strategies available to runners, coaches and HCPs giving deeper insight into the multifactorial nature of injury prevention. Data collected within this scoping review should be taken in the context of the broad range of types of studies identified and accessed. We did not consider studies prior to 2000, and this was based on the majority of studies before this having been conducted on military participants which were considered to have variables other than running to have an effect on injury and types of injury, hence the exclusion of Pope et al. and Yeung et al. [140, 141]. Methods used in the included studies were heterogeneous, but we believe this has provided a broad range of diverse views, and the inclusion of surveys and qualitative studies added a deeper more meaningful significance to experts' viewpoints and findings from quantitative studies. A number of reviews summarized in Table 2 and illustrated in Figure 3 may have included the same original research studies, and thus, the conclusions drawn from this may be over-represented. In view of this, weighting was not applied to each specific intervention highlighted in Table 2.
Epidemiology studies were excluded as although these provide associations and risk factors and hypotheses on what could or should prevent injury, they were not included unless they looked specifically at interventions and associations with preventing RRI. Studies directly investigating risk factors for RRI were also excluded where possible to avoid making assumptions based solely on risk factors and to ensure the relevant literature discussing proactive strategies to reduce the likelihood of injury was highlighted. The average age of runners in this current scoping review including novice runners appears higher than other studies conducted in different sports on injury risk reduction practices [12], and this may need to be investigated in future studies to identify whether there are specific risk profiles for people taking up running later in life, perhaps following a previously sedentary lifestyle.
5. Conclusion
This scoping review identified strength training, gait re-education, graduated running programmes, footwear and online education as the main strategies investigated in intervention studies on injury risk reduction practices in runners. Additionally, recovery strategies have been recommended by experts, but no research studies have yet investigated this. Current practices reducing the risk of injury have been largely unsuccessful, not because they have not addressed risk factors, but possibly due to the method of delivery. It appears key that where more supervision and support have been provided alongside interventions, the outcome for reducing RRI is more effective. Also, in contrast to the linear approach to injury risk reduction practices in research studies, experts believe a multifactorial approach as most beneficial. Through this approach, runners may be provided and supported with the capacity to make informed decisions when adopting injury risk reduction strategies, influence goal setting and learn more about their own individualized injury risk profile. If this entails runners choosing the most convenient options or strategies that enforce a sense of self-efficacy, then we should ensure they have knowledge for best practice. Further research on runner's preferences and areas such as recovery and wearables, and specific risk profiles such as youth or interventions for specific injuries is needed ensuring that the runners' views and needs are at the centre of the development of future injury risk reduction research and that changes in behaviour modification are just as an important an outcome measure as a reduction in injury. Having support from peers within a group environment, supervision from HCPs and coaches, using wearables with personalized feedback or developing educational digital health is likely the most effective means for facilitating injury risk reduction practices in runners.
6. Perspectives and Recommendations for Future Research
Runners are interested in learning about injury prevention approaches, particularly following previous injury, but runners should be given choice, and approaches must be easily incorporated into usual training habits. Promising strategies such as gait re-education, use of wearables and recovery that runners can adopt with little impact on usual running habits need further research to demonstrate efficacy. Research should use outcome measures such as effect on behaviour change as well as reduction in injury to understand runner's response to injury prevention interventions better. Educational personalized online modules addressing runners' individualized injury risk profiles and digital health need further exploration with different populations of runners; however, coaches may be best placed to provide a supervised approach if they have the knowledge. A train-the-trainer approach could provide scope to reach the wider running community. We found experts propose a range of injury risk reduction strategies for runners to address the multifactorial nature of RRI, but current injury prevention RCTs tend to focus on specific risk factors or do not provide supervision for interventions which may explain in part that RRIs remain high in comparison with other sports. There is heterogeneity across the studies selected in this scoping review, which includes all types of running and a range of methodologies. Researchers and HCPs can use the findings to develop more robust research and to help runners engage with strategies to reduce their risk of RRI.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kakouris N. Yener N. Fong D. A Systematic Review of Running-Related Musculoskeletal Injuries in Runners Journal of Sport and health Science 202110551352210.1016/j.jshs.2021.04.00133862272 PMC 8500811 · doi ↗ · pubmed ↗
- 2van Poppel D. van der Worp M. Slabbekoorn A. Risk Factors for Overuse Injuries in Short- and Long-Distance Running: A Systematic Review Journal of Sport and Health Science 2021101142810.1016/j.jshs.2020.06.00632535271 PMC 7856562 · doi ↗ · pubmed ↗
- 3Frandsen J. S. B. Siminsen N. S. Hulme A. Jocobsen J. S. Nielsen R. O. A Paradigm Shift in Understanding Overuse Running-Related Injuries: Findings From the Garmin-RUNSAFE Study Point to a Sudden Not Gradual Onset JOSPT In press 10.2519/josptopen.2024.0075 · doi ↗
- 4Bertelsen M. L. Hulme A. Petersen J. A Framework for the Etiology of Running-Related Injuries Scandinavian Journal of Medicine & Science in Sports 201727111170118010.1111/sms.128832-s 2.0-8501865391128329441 · doi ↗ · pubmed ↗
- 5Napier C. Willy R. W. The Prevention and Treatment of Running Injuries: A State of the Art International Journal of Sports Physical Therapy 202116496897010.26603/001c.2575434386275 PMC 8329326 · doi ↗ · pubmed ↗
- 6Alaiti R. K. Reis F. J. J. Pain in Athletes: Current Knowledge and Challenges International Journal of Sports Physical Therapy 202217698198310.26603/001c.3767536237643 PMC 9528677 · doi ↗ · pubmed ↗
- 7Smart K. M. The Biopsychosocial Model of Pain in Physiotherapy: Past, Present and Future Physical Therapy Reviews 2023282617010.1080/10833196.2023.2177792 · doi ↗
- 8Lacey A. Whyte E. O’Keeffe S. O’Connor S. Burke A. Moran K. The Running Injury Continuum: A Qualitative Examination of Recreational Runners’ Description and Management of Injury P Lo S One 20231810 p. e 029236910.1371/journal.pone.0292369 PMC 1055019137792711 · doi ↗ · pubmed ↗