The influence of antenatal betamethasone timing on neonatal outcome in late preterm infants: a single-center cohort study
Thomas Brückner, Anke Redlich

TL;DR
This study examines how the timing of antenatal betamethasone affects late preterm infants and finds recent administration may reduce respiratory issues in high-risk cases.
Contribution
The study introduces a risk-adapted approach to antenatal corticosteroid use in late preterm pregnancies.
Findings
Recent antenatal corticosteroid administration reduced cardiorespiratory morbidities in high-risk late preterm infants.
The benefit of recent corticosteroid use depends on the prevalence of respiratory disease in the population.
Current evidence supports the need for better antenatal tools to predict respiratory risks before additional steroid courses.
Abstract
Many pregnancies continue after antenatal corticosteroid exposure. Since long-term effects on late preterm neonatal outcome remain controversial, it remains unknown whether pregnant women who are at risk for preterm birth during the late preterm period and had prior antenatal corticosteroid exposure would benefit from an additional course of antenatal corticosteroids. We evaluated the need for future trials on this topic by comparing short term effects from antenatal betamethasone to long-term effects. We also examined the value of a risk-adapted approach. We observed neonatal outcomes in late preterm infants (34/0–36/0 weeks of gestation) who were exposed to antenatal betamethasone either up to 10 days prior birth (n = 8) or earlier in pregnancy (n = 89). We examined a real world population from the University Hospital Magdeburg (Germany) between 01 January 2012 and 31 December 2018,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
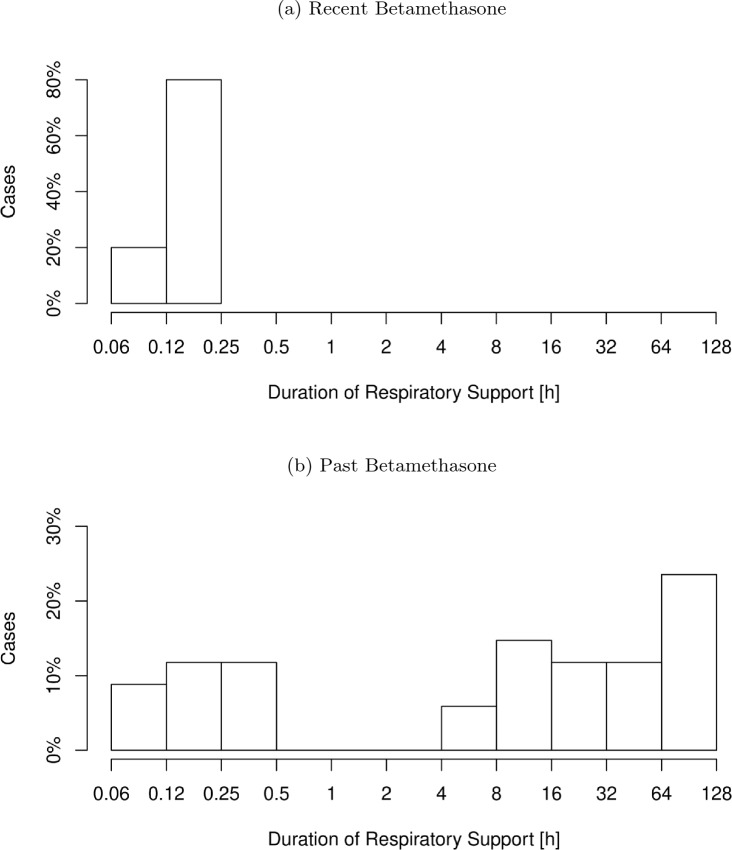 Figure 1
Figure 1- —Otto-von-Guericke-Universität Magdeburg (3121)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal Respiratory Health Research · Birth, Development, and Health · Infant Development and Preterm Care
What does this study add to the clinical work
In an unselected population, we cannot support the use of additional betamethasone courses during the late preterm period. However, in a high-risk population that is not defined yet an additional betamethasone course may prevent severe respiratory disease.
Introduction
Antenatal corticosteroids (ACS) to prevent neonatal respiratory distress syndrome are standard of care for pregnant women at risk for immanent birth during the extreme (23/0–27/6 weeks of gestation), early (28/0–31/6) and moderate (32/0–33/6) preterm period. The use of ACS in the late preterm period (34/0–36/6 weeks) remains controversial. The upper limit to the appropriate gestational age was challenged by the Antenatal Late Preterm Steroid (ALPS) trial in 2016 [1], which reported significant effects on respiratory outcomes even after 34 weeks of gestation. The rate of late preterm and term infants exposed to ACS constantly increased in the aftermath of the ALPS trial [2, 3], although follow-up studies of randomized controlled trials (RCTs) reported increased risks for lower academic ability [4] and neurosensory deficits [5]. Ongoing concerns about mental and behavioral deficits result from large population studies, but are at serious risk for bias [6–9]. However, during the follow-up of the ALPS trial ACS was not associated with an adverse long-term developmental outcome [10]. Still, the current development towards a more liberate use of ACS raises the need for external evidence on safety and efficacy of ACS in different clinical scenarios. Besides pregestational diabetes pregnancies, major fetal malformations and twin pregnancies, the ALPS trial excluded women who received a prior course of ACS, to prevent contamination of the control group [1]. However, studies on the effect of prior ACS administrations on neonatal outcome in late preterm infants report conflicting results, ranging from dramatic improvement to worsening of respiratory morbidity [11–14]. None of these studies reported the time interval from ACS administration to birth.
For deliveries earlier than 34 weeks of gestation, ACS had an optimal effect on neonatal respiratory outcome when delivery occurred 2 to 7 days after administration [15–21]. However, the risk reduction for long-term sequelae seems to extend beyond that period [16–20], at least up to 10 days [22]. Thus the overall duration of protective ACS effects is difficult to determine. For ACS administration in the late preterm period there was no evidence for another increase of respiratory morbidity after 7 days [21]. Protective effects of prior ACS administrations may extend into the late preterm period, but prior ACS administrations may as well be an indicator for pregnancies, that are prone to adverse neonatal outcomes. In the clinical scenario of a pregnant woman at risk for preterm birth during the late preterm period, and prior ACS exposure, the risks and benefits from another ACS course remain unknown.
The objective of this study was to compare short-term with long-term effects of ACS on the neonatal outcome in a real-world late preterm population and in a simulated high-risk subpopulation. In this way, we wanted to determine the eligibility of future RCTs on additional ACS courses during the late preterm period in the context of prior ACS exposure. As a secondary objective we wanted to examine the value of a more individualized approach to ACS administrations in this context.
Materials and methods
Overview
We designed this study as an single-center cohort study at the University Hospital for Gynecology, Obstetrics and Reproductive Medicine in Magdeburg, Germany, in cooperation with the Neonatal Department.
We included all mother–child dyads of singleton pregnancies terminated at 34/0 to 36/6 weeks of gestation between 01 January 2012 and 31 December 2018 who received at least one course of intramuscular betamethasone anytime during pregnancy. Exclusion criteria were uncertainty of gestational age, major fetal malformations, other severe fetal inborn diseases and unpredictable corticosteroid effects. The full study protocol is available in the supplemental appendix.
We only used data previously generated in accordance with the patient’s written consent during hospital stay. The study was approved by the ethics committee of the Otto-von-Guericke University Magdeburg.
Patient selection and cohort definition
We searched the birth registry for singleton pregnancies terminated at 34/0 to 36/6 weeks. We identified 526 mother and child dyads. All corresponding electronically archived medical records were manually reviewed by the first author. Inclusion and exclusion criteria were checked, cohort membership assigned, and data was recorded manually in a spreadsheet, according to the study protocol. We included 151 dyads who received betamethasone anytime during pregnancy, and assigned each dyad to one of two cohorts. The Recent Betamethasone (RB) cohort included all dyads that completed a course of betamethasone not more than 10 days prior to birth. The Past Betamethasone (PB) cohort included all dyads, in which the last betamethasone course was completed more than 10 days before delivery.
The decision to administrate betamethasone was made by the treating physicians, based on clinical judgement and the hospital’s Standard Operating Procedure (SOP) for antenatal betamethasone administration. We excluded nine mother-child dyads with neonates suffering from major malformations or severe inherited diseases, seven with uncertainties concerning the gestational age dating and one with an incomplete betamethasone trial at delivery. In principle 134 dyads were considered eligible for further evaluation. Eight dyads belonged to the RB cohort and 126 dyads belonged to the PB cohort.
Since the hospital’s SOP covered routine-ACS administrations only until the age of 33/6 weeks, the RB cohort was more likely to be of younger gestational age. This was confirmed by our first comparison of pregnancy characteristics. We restricted the PB cohort to the maximum gestational age of the RB cohort to eliminate this important confounder. A total of 97 dyads with gestational ages ranging from 34/0 to 36/0 weeks were ultimately included in the final analysis. All dyads had completed at least one course (2 doses) of intramuscular betamethasone 12 mg, either 12 h (fast track) or 24 h apart. Four dyads in the PB cohort had completed a second course of betamethasone at 25/0, 25/1, 25/6 and 27/3 weeks, respectively. No dyad had more than 2 courses of antenatal betamethasone.
To simulate a high-risk population we selected those dyads with any need for respiratory support in the neonate from the original dataset.
Data abstraction
Personal data was pseudonymized during data recording and analysis, and anonymized for long-term storage. We defined 43 items to describe pregnancy characteristics and the maternal risk profiles, and 92 items to characterize the neonatal population and their outcomes. Details about item definition are described in the study protocol. Modes of delivery were grouped into cesarean section and other. However, all neonates were either subject to spontaneous vaginal delivery or cesarean section. The only neonate born by vacuum extraction dropped out during the restriction of the PB cohort to the maximum gestational age of 36/0 weeks. There was no neonate born by forceps. The neonatal outcome was divided into 10 different categories: neonatal outcome—biometric, death, cardiorespiratory, infection, neurologic, metabolic, icterus, feeding, temperature regulation and hospital stay. All items were manually recorded from electronically archived medical records by the first author. Unavailable item data were left empty, and the affected cases were excluded during the analysis of the individual item.
We refrained from assigning the disease labels “wet lung” or “respiratory distress syndrome”, because unambiguous definition criteria were difficult to meet. In this regard, the absence of chest X-rays in most cases was the main limiting factor. Instead, we focused on the duration of respiratory support and the use of surfactant as surrogate, but more valid parameters.
Composite outcomes
For all categories except Biometric, Infection and Icterus a composite outcome was generated to indicate any adverse events of special interest. Composite outcome-death was defined as stillbirth or neonatal death up to 28 days of life. Composite outcome-cardiorespiratory was defined as any of the following parameters: continuous positive airway pressure (CPAP) or high flow nasal cannula (HFNC) >2 h, need for inspired oxygen fraction (FiO_2_) >0.3 >4 h, mechanical ventilation, external membrane oxygenation (ECMO), surfactant application, pneumothorax, bronchopulmonal dysplasia (BPD) or arterial hypotension. Composite outcome-neurologic was defined as the incidence of any intracranial bleeding, encephalopathy or neonatal seizures. Composite outcome-metabolic was defined as either severe hypoglycemia or need for glucose containing i.v. solutions. Composite outcome-feeding was defined as either ablactation or need for additional formula feds at dismission/transfer to another hospital. Composite outcome-temperature regulation was defined as either need for external heat or the lack of rooming-in on the first day of life. Composite outcome-hospital stay was defined as Neonatal Intensive Care Unit (NICU) stay of any duration, hospital stay >21 days or transfer to another hospital (lost to follow-up). The composite outcome-combined was defined as the occurrence of any composite outcome. Composite outcome-BIAS was defined as any of the following: transfer to another hospital, discharge against physician’s advice or incomplete documentation.
Data analysis
For categorial data, we display the number of affected cases in total numbers and in percent. Differences between both cohorts were tested for significance with Fisher’s test. The effect size is described by the odds ratio. For all numeric variables we assumed a nonparametric model. For numeric data, we display median and range. To determine the effect size we calculated the difference in arithmetic means. Differences in numeric parameters between the two cohorts were tested for significance using the Brunner–Munzel test. A type I error <0.05 was considered to be significant.
All analyses were performed using the “R” software environment version 3.6.3 (Linux Kernel 5.4.0-139-generic on an Intel Core i7 CPU).
Results
Pregnancy characteristics and risk profiles
Mothers in the PB cohort had a higher rate of abortions prior to the current pregnancy. We found no other differences in pregnancy characteristics (Tables 1, 2). In the RB cohort there were non-significant trends towards more deliveries by cesarean section, more deliveries for medical indication, Streptococcus B colonization, pregnancies with intrauterine growth retardation and higher rates of rhesus incompatibility with positive Coombs test.Table 1. Corrected maternal and pregnancy characteristicsRecent betamethasonePast betamethasone \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\Delta$$\end{document} meanp-valueMedian(Range) [n = 8]Median(Range) [n = 89]Maternal age [a]28.5(22–36)30(17–41)– 0.930.558Body mass index [kg/m^2^]25.7(15.1–29.4)23.1(17.9–42.3)– 0.860.798Gestational age [d]240.5(239–252)244(238–252)– 1.980.303Gravida [n]2(1–4)2(1–7)0.000.652Para [n]1(1–3)1(1–5)– 0.170.550Miscarriages [n]1(0–1)0(0–2)0.370.077Abortions [n]0(0–0)0(0–3)– 0.17<0.001Stillbirths [n]0(0–0)0(0–1)– 0.010.320Cesarean sections [n]1(0–3)1(0–4)0.120.675Latency to bethamethasone [d]7.5(0–10)34(11–80)– 33.73<0.001GA at betamethasone [d]235.5(230–252)209(170–236)31.39<0.001Table 2Pregnancy risk profilesRecent betamethasonePast betamethasoneOdds ratiop-valueNo.(%) [n = 8]No.(%) [n = 89]Cesarean section7(87.5)56(62.9)4.080.254Assisted reproduction0(0.0)7(7.9)0.001.000Smoking in pregnancy2(25.0)19(21.3)1.231.000Prior pregnancy complications1(12.5)26(29.2)0.350.437Prior birth complications1(12.5)22(24.7)0.440.676Pregnancy at risk8(100.0)86(96.6)Inf1.000Medically indicated delivery7(87.5)43(48.3)7.360.060Gestational diabetes0(0.0)15(16.9)0.000.351Insulin therapy0(0.0)7(7.9)0.001.000Makrosomia0(0.0)1(1.1)0.001.000Birth arrest/mismatch0(0.0)10(11.2)0.001.000Gestational hypertonus1(12.5)6(6.7)1.960.464Preeclampsia0(0.0)7(7.9)0.001.000HELLP-syndrome1(12.5)4(4.5)2.980.356Gestational hepatosis0(0.0)0(0.0)0.001.000Intrauterine growth retardation3(37.5)18(20.2)2.340.365Prior uterine operation1(12.5)26(29.2)0.350.437Uterine malformation0(0.0)5(5.6)0.001.000Chorionic villus sampling0(0.0)1(1.1)0.001.000Bleeding in pregnancy0(0.0)25(28.1)0.000.108Strapping0(0.0)3(3.4)0.001.000Anemia during pregnancy5(62.5)50(56.2)1.301.000Rhesus incompatibility1(12.5)6(6.7)1.960.464Coombs test positive1(33.3)1(12.5)3.060.491Amiotic infection syndrome0(0.0)1(1.1)0.001.000Suspected triple I0(0.0)0(0.0)0.001.000Confirmed triple I0(0.0)0(0.0)0.001.000STORCHL-infection0(0.0)2(2.2)0.001.000Streptococcus B colonization1(50.0)6(12.0)6.870.253Bleeding immediately prior to birth0(0.0)1(1.1)0.001.000Partial premature placental abruption0(0.0)4(4.5)0.001.000Premature placental abruption0(0.0)2(2.2)0.001.000
Characteristics of the neonatal population
The lower head circumferences in the RB cohort reached significance, but not the dedicated z scores. There were non-significant trends towards lower birthweight and length, as well as more Small-for-Gestational-age children in the RB cohort (Table 3).Table 3. Neonatal characteristicsRecent betamethasonePast betamethasone \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\Delta$$\end{document} Meanp-valueMedian(Range) [n = 8]Median(Range) [n = 89]Birthweight [g]2020(1200–2720)2320(1390–3420)– 307.320.151Birthweight z-score– 0.82(– 2.76 to 0.42)– 0.46(– 2.47 to 1.33)– 0.520.422Length at birth [cm]44(29.5–50)46.5(38–51)– 2.890.257Length at birth z-score– 0.83(– 5.9 to 0.96)– 0.45(– 3.39 to 1.32)– 0.870.464Head circumference [cm]30.25(26.5–33)32(28–36)– 1.610.047Head circumference z-score– 1.46(– 3.46 to 0.24)– 0.56(– 3.35 to 2.17)– 0.860.169No.(%) [n = 8]No.(%) [n = 89]Odds ratiop-valueAssigned sex (m:f)4:4(50:50)48:41(54:46)0.861.000Small-for-gestational-age3(37.5)19(21.3)2.190.376
Neonatal outcome-cardiorespiratory
The RB cohort had significantly less days on caffeine treatment, but with a barely relevant effect size. Non-significant trends showed an increased number of neonates with respiratory distress during the first 2 h of life in the RB cohort (62.5% vs. 44.9%) with a reduction of mean respiratory support duration in the RB cohort by about 11 h at the same time. Not a single case in the RB cohort needed respiratory support longer than 2 h in contrast to 24.7% in the PB cohort. A relevant adverse cardiorespiratory outcome, as indicated by the Cardiorespiratory Composite Outcome, occured in 27% in the PB cohort, while there was not a single case in the RB cohort (Table 4). The distribution of respiratory support duration shows two clusters in the PB cohort, probably referring to different etiologic entities. In the RB cohort the cluster with longer respiratory support vanished (Fig. 1).Fig. 1a) Distribution of respiratory support duration, when betamethasone was administered up to 10 days prior birth. b) Distribution of respiratory support duration, when betamethasone was administered more than 10 days prior birth. The second peak of respiratory support duration > 4 h vanished, when betamethasone was administered up to 10 days prior birth
In the simulated high-risk population there was a significant reduction of respiratory support duration by 28.8 h (p< 0.001). Need for CPAP/HFNC >2 h did not occur in the RB cohort subpopulation compared to 64.7% in the PB cohort (p = 0.011). This results in a decrease of the Cardiorespiratory Composite Outcome from 67.6% to 0.0% (p = 0.008), compared to 27.0% to 0.0% (p = 0.194) in the general late preterm population (Table 5). This translates into a reduction of the Number Needed to Treat (NNT) from 3.7 to 1.5, when ACS administration would be provided only for infants with postnatal need for respiratory support.Table 4. Neonatal outcome-cardiorespiratoryRecent betamethasonePast betamethasoneOdds ratiop-valueNo.(%) [n = 8]No.(%) [n = 89]Supported transition4(50)27(30.3)2.270.263Respiratory transition disorder5(62.5)40(44.9)2.030.466Intubation0(0)2(2.2)0.001.000HighFlow nasal cannula0(0)3(3.4)0.001.000Continuous positive airway pressure5(62.5)33(37.1)2.800.256Inspired oxygen fraction> 0.31(12.5)18(20.2)0.571.000Any respiratory support5(62.5)34(38.2)2.670.261CPAP/HFNC > 2 h0(0)22(24.7)0.000.192CPAP/HFNC > 12 h0(0)16(18)0.000.346FiO_2_ > 0.3 longer than 4 h0(0)3(3.4)0.001.000FiO_2_ > 0.3 longer than 24 h0(0)0(0)0.001.000Extracorporal membrane oxygenation0(0)0(0)0.001.000Surfactant0(0)1(1.1)0.001.000Apnoe2(25)19(21.3)1.231.000Pneumothorax0(0)0(0)0.001.000Mekonium aspiration syndrome0(0)0(0)0.001.000Bronchopulmonary dysplasia0(0)0(0)0.001.000PPHN0(0)0(0)0.001.000Persistent fetal circulation0(0)0(0)0.001.000Arterial hypotension0(0)4(4.5)0.001.000Hemodynamically relevant PDA0(0)0(0)0.001.000PDA: ibuprofene therapy0(0)0(0)0.001.000Composite outcome: cardiorespiratory0(0)24(27)0.000.194Median(Range) [n = 8]No.(Range) [n = 89] \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\Delta$$\end{document} Meanp-valueUmbilical artery pH7.34(7.23–7.37)7.32(7.16–7.46)0.000.898Umbilical vein pH7.38(7.29–7.40)7.38(7.21–7.55)– 0.010.908APGAR min. 18(5–9)9(4–10)– 0.720.140APGAR min. 59(7–10)10(6–10)– 0.230.503APGAR min. 1010(9–10)10(7–10)0.210.451Invasive ventilation [h]0(0–0)0(0–92)– 1.070.158HFNC [h]0(0–0)0(0–51)– 0.820.083CPAP [h]0.11(0–0.2)0(0–95.5)– 9.080.613Overall need for respiratory support [h]0.11(0–0.2)0(0–109.25)– 10.970.693Inspired oxygen fraction >0.3 [h]0(0–0.02)0(0–22.75)– 0.580.375Treatment with caffeine [d]0(0–0)0(0–15)– 0.98< 0.001Need for volume administration [n]0(0–0)0(0–1)– 0.030.083Need for catecholamine treatment [d]0(0–0)0(0–4)– 0.040.320Table 5Subgroup analysis–neonates with adverse respiratory outcomeRecent betamethasonePast betamethasoneOdds ratiop-valueNo.(%) [n = 5]No.(%) [n = 34]Supported transition4(80)27(79.4)1.041.000Respiratory transition disorder5(100)32(94.1)Inf1.000Intubation0(0)2(5.9)0.001.000HighFlow nasal cannula0(0)3(8.8)0.001.000Continuous positive airway pressure5(100)33(97.1)Inf1.000Inspired oxygen fraction > 0.31(20)18(52.9)0.230.342Any respiratory support5(100)34(100)0.001.000CPAP/HFNC > 2 h0(0)22(64.7)0.000.011CPAP/HFNC > 12 h0(0)16(47.1)0.000.066FiO_2_ > 0.3 longer than 4 h0(0)3(8.8)0.001.000FiO_2_ > 0.3 longer than 24 h0(0)0(0)0.001.000Extracorporal membrane oxygenation0(0)0(0)0.001.000Surfactant0(0)1(2.9)0.001.000Apnoe2(40)14(41.2)0.951.000Pneumothorax0(0)0(0)0.001.000Mekonium aspiration syndrome0(0)0(0)0.001.000Bronchopulmonary dysplasia0(0)0(0)0.001.000PPHN0(0)0(0)0.001.000Persistent fetal circulation0(0)0(0)0.001.000Arterial hypotension0(0)3(8.8)0.001.000Hemodynamically relevant PDA0(0)0(0)0.001.000PDA: ibuprofene therapy0(0)0(0)0.001.000Composite outcome: cardiorespiratory0(0)23(67.6)0.000.008Median(Range) [n = 5]Median(Range) [n = 34] \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\Delta$$\end{document} Meanp-valueUmbilical artery pH7.34(7.23–7.37)7.32(7.22–7.46)– 0.010.895Umbilical vein pH7.36(7.29–7.40)7.38(7.27–7.55)– 0.030.372APGAR min. 17(5–8)7(4–10)– 0.550.429APGAR min. 58(7–9)8(6–10)0.110.789APGAR min. 1010(9–10)9(7–10)0.660.057Invasive ventilation [h]0(0–0)0(0–92)– 2.800.160HFNC [h]0(0–0)0(0–51)– 2.140.083CPAP [h]0.17(0.08–0.2)10.54(0–95.5)– 23.86< 0.001Overall need for respiratory support [h]0.17(0.08–0.2)12.38(0.07–109.25)– 28.80< 0.001Inspired oxygen fraction > 0.3 [h]0(0–0.02)0.05(0–22.75)– 1.530.007Treatment with caffeine [d]0(0–0)0(0–15)– 1.85< 0.001Need for volume administration [n]0(0–0)0(0–1)– 0.060.160Need for katecholamine treatment [d]0(0–0)0(0 - 4)– 0.120.325
Neonatal outcome-metabolic
The analysis for hypoglycemia related problems showed significantly longer administration of glucose containing intravenous solutions in the RB cohort. There was a non-significant trend towards more hypoglycemia, severe hypoglycemia and need for glucose substitution. No neurologic sequelae of hypoglycemia was reported during the neonatal period.
Neonatal outcome-icterus
The RB cohort received significantly less photo therapy. Lower maximum bilirubin levels in the RB cohort closely missed significance.
Neonatal outcome-feeding
There were no significant differences in the feeding category. Non-significant trends suggested prolonged gastric tube feeding and gastroesophageal reflux in the RB cohort.
Neonatal outcome-temperature regulation
The need for incubator stay was evenly distributed between both cohorts. On average, neonates in the RB cohort stayed 2.81 days longer in warm beds/under heat lamps, closely failing significance.
Neonatal outcome-hospital stay
A significant difference between both cohorts was detected for weight at discharge. On average, neonates in the RB cohort were 271.2 g lighter than the PB cohort at similar gestational ages. All other items did not reach significance. Not a single neonate in the RB cohort was eligible for rooming-in on the first day of life in contrast to 25.8% of neonates in the PB cohort. The need for a neonatal intensive care unit (NICU) stay was 50% in the RB cohort vs. 30.3% in the PB cohort. The mean duration of NICU stay was similar between both cohorts.
Neonatal outcome-other
There were no stillbirths or deaths during the neonatal period in either cohort. There was no significant difference in the rate of infections or infection related diseases. No serious neurological events were reported.
Neonatal outcome—composite outcomes
Composite Outcome parameters (see Composite Outcomes) did not show any significant differences in the original population (Table 6). The cardiorespiratory composite outcome was significantly in favor of the RB cohort in the simulated high-risk cohort as mentioned above (see Neonatal outcome—composite outcomes).Table 6. Neonatal outcome—composite outcomesRecent betamethasonePast betamethasoneOdds ratiop-valueNo.(%) [n = 8]No.(%) [n = 89]Composite outcome: death0(0.0)0(0.0)0.001.000Composite outcome: cardiorespiratory0(0.0)24(27.0)0.000.194Composite outcome: neurologic0(0.0)2(2.2)0.001.000Composite outcome: metabolic6(75.0)45(50.6)2.900.274Composite outcome: feeding5(62.5)55(61.8)1.031.000Composite outcome: temperature regulation8(100.0)66(74.2)Inf0.192Composite outcome: hospital stay4(50.0)33(37.1)1.690.476Composite outcome: combined8(100.0)79(88.8)Inf1.000
Comment
Principal findings
The composite outcome parameters, indicating relevant adverse events, did not show any significant differences between both cohorts.
In our simulated high-risk population recent ACS administration was associated with a significant and relevant reduction of severe respiratory disease, and a reduced Number Needed to Treat. However, we are not yet able to reliably identify this subpopulation in the antenatal setting.
Context
Known risk-factors for adverse neonatal outcome in late preterm infants are lower gestational age [23–25], low birthweight [24, 26–28], male fetus [27, 29], gestational diabetes and large-for-gestational-age [24, 30, 31], chorioamnionitis [31], medically indicated delivery [32] and cesarean section [24, 33–35]. As reported in Section "Pregnancy Characteristics and Risk Profiles" we did not find any significant group differences, concerning these possible confounders. Considering non-significant trends, the RB cohort was affected by a higher prevalence of these risk-factors, except for gestational diabetes. Given the lower rate of Composite Cardiorespiratory Outcome in the RB cohort, we do not believe in a relevant confounding influence. We were not able to show a significant correlation between recent ACS administration and hypoglycemia, but the prolonged need for glucose containing intravenous solutions in the RB cohort may indicate an impaired glucose metabolism. Gulersen et al. demonstrated that the risk for hypoglycemia is highest in the group of late preterm infants delivered timely after ACS administration [21]. Many of the trends reported, including hypoglycemia, may be confounded by low birthweights. Low birthweights were reported to occur in the context of ACS [36, 37] and even the most recent reviews still include trends towards lower birthweights similar to our findings [38, 39]. We were not able to determine whether low birth biometrics resulted from recent ACS administration or were a preexisting condition. As low birthweight may not be independent of ACS, a corrected analysis was omitted.
Despite higher rates of rhesus incompatibility and positive Coombs tests, the maximum bilirubin levels were significantly lower in the RB cohort, and those neonates needed less phototherapy. Positive effects of ACS on the need for phototherapy were shown previously by Porto et al. [40].
We found no adverse neurologic effects of hypoglycemia in the neonatal period, but we cannot tell about possible long-term effects.
Clinical and research implications
We cannot support unselected rescue-ACS administrations in the late preterm period on the current data basis. Positive effects on the respiratory morbidity in late preterm infants strongly depend on the prevalence of respiratory disease. Therefore, randomized controlled trials on rescue ACS administrations in the late preterm period should focus on high-risk populations. We suggest to put more efforts into the development of clinical prediction tools to determine the risk of respiratory disease late preterm infants.
Strengths and limitations
One strength of our study is the comparability of both cohorts. After correction for gestational age, both cohorts were considered to be comparable. The higher rate of abortions prior to the current pregnancy in the PB cohort was judged to be irrelevant to the neonatal outcome.The generalizability of our results benefits from the real world population with low dropout rates, but is limited by the single-center approach. The main limitation of our study is the low number of cases in the RB cohort, because ACS administrations were handled very strict at our center. Therefore real significances may easily be missed. On the other hand we wanted to display a wide range of outcome parameters of possible interest, that may interact with each other in different ways. This makes our study prone to the risk of false-significant results due to alpha-error accumulation. The condensation of single parameters into composite outcome parameters, indicating relevant adverse outcomes, somewhat attenuates the impact of alpha-error accumulation, if we strictly focus on the composite outcome parameters in the final interpretation. As our objective was to give guidance to future study design, we prioritized the identification of relevant outcome parameters over the avoidance of alpha-error accumulation. Another limitation is the retrospective study design, that limited data quality and availability. We were unable to obtain data about the individual indication for ACS administration and estimated birthweights, and we had only limited access to Body Mass Indices (BMI) in the early pregnancy (44.3% of all cases with missing data).
Conclusion
A risk-adapted approach to additional ACS-administrations in the late preterm period may yield the potential to address adverse long-term neurodevelopmental effects resulting from neonatal respiratory disease, while lowering the number of ACS exposures. Before considering clinical trials on additional antenatal corticosteroid courses in the late preterm period, antenatal assessment tools to predict respiratory morbidity need to be developed.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file 1 (pdf 0 KB)Supplementary file 2 (pdf 0 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Battarbee AN, Glover AV, Vladutiu CJ, Gyamfi-Bannerman C, Aliaga S, Manuck TA et al. (2019) Risk factors associated with prolonged neonatal intensive care unit stay after threatened late preterm birth. The Journal of Maternal-Fetal & Neonatal Medicine: The Official Journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 1–610.1080/14767058.2019.1623777 PMC 700897431170845 · doi ↗ · pubmed ↗
- 2Schmidt EM, Powell JM, Garg B, Caughey AB (2024) Association between gestational age and perinatal outcomes in women with late preterm premature rupture of membranes. Am J Perinatol 2024 (efirst)10.1055/a-2328-619238754462 · doi ↗ · pubmed ↗
- 3Crowther CA, Mc Kinlay CJ, Middleton P, Harding JE (2015) Repeat doses of prenatal corticosteroids for women at risk of preterm birth for improving neonatal health outcomes. Cochrane Database of Systematic Reviews (7) CD 003935. Publisher: John Wiley & Sons, Ltd. Available from: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD 003935.pub 4/full 10.1002/14651858.CD 003935.pub 4PMC 710452526142898 · doi ↗ · pubmed ↗
- 4Mc Goldrick E, Stewart F, Parker R, Dalziel SR (2020) Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database of Systematic Reviews (12) CD 004454. Publisher: John Wiley & Sons, Ltd. Available from: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD 004454.pub 4/full 10.1002/14651858.CD 004454.pub 4PMC 809462633368142 · doi ↗ · pubmed ↗