Concurrence of bird-related hypersensitivity pneumonitis and systemic sclerosis-associated interstitial lung disease
Mai Miyahara, Kazuki M Matsuda, Hirohito Kotani, Tomomi Miyake, Asako Yoshizaki-Ogawa, Ayumi Yoshizaki, Shinichi Sato

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
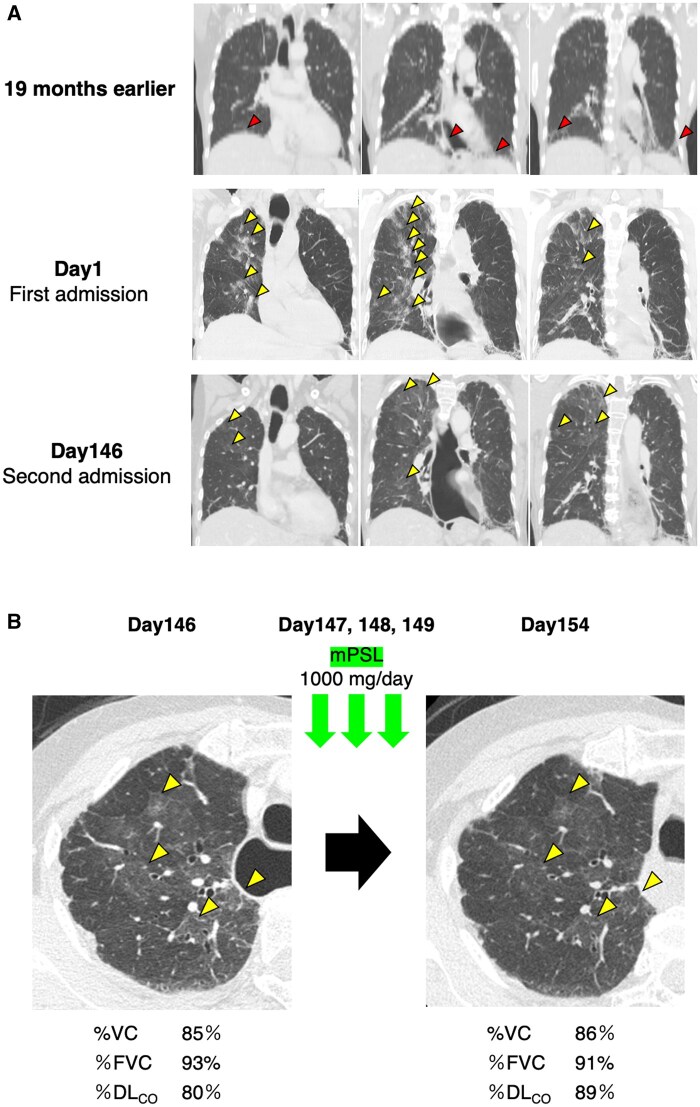 Figure 1
Figure 1- —JSPS KAKENHI
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Sclerosis and Related Diseases · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Allergic Rhinitis and Sensitization
Dear Editor, Hypersensitivity pneumonitis (HP) is an inflammatory syndrome affecting the lungs, resulting from repeated inhalation of a variety of antigens, as well as exposure to drugs such as antibiotics, anticancer drugs and immunosuppressants, including methotrexate [1, 2]. HP can present acutely, subacutely or chronically [3] and is classified into nonfibrotic and fibrotic phenotypes [2]. Diagnosing HP can be challenging, especially in the presence of overlapping conditions such as SSc-associated interstitial lung disease (ILD). This case report highlights the diagnostic process and management of bird-related HP in a patient with SSc-ILD.
A 73-year-old female with a 26-year history of limited cutaneous SSc (lcSSc) positive for anti-topoisomerase I antibody (ATA) on 5 mg/day of prednisolone (PSL) complained of worsening of dry cough lasting for 6 months with breathlessness. She was admitted urgently with a fever of 39°C and respiratory failure, with a percutaneous oxygen saturation of 83% on room air. High-resolution chest CT (HRCT) revealed numerous panlobular ground-glass opacities with intralobular reticular opacities (crazy-paving appearance) throughout the lungs, in addition to pre-existing mild subpleural reticular shadows at the bilateral lung bases, consistent with nonspecific interstitial pneumonia (NSIP) observed on HRCT performed 19 months earlier (Fig. 1A). There were no signs of active SSc, such as progression of skin sclerosis, peripheral circulatory disturbances, pulmonary hypertension or renal crisis. Additionally, the patient exhibited unresponsiveness to antimicrobial therapy (ceftriaxone 2 g/day for 3 days). At the time of presentation, her family history was unremarkable, and she had no known allergies. She had never been exposed to methotrexate.
Initial treatment with methylprednisolone (mPSL) pulse therapy (1000 mg/day for 3 consecutive days) and subsequent maintenance on 40 mg/day of PSL were provided under the assumption of SSc-ILD exacerbation (Fig. 1A). Her fever and respiratory condition improved with mPSL pulse therapy, and the newly developed panlobular ground-glass opacities with a crazy-paving appearance exhibited temporary improvement. However, her symptoms recurred with tapering doses of oral PSL, leading to her second admission. On admission, she was on PSL 20 mg/day and MMF 1000 mg/day. MMF was introduced in response to her worsening respiratory symptoms, which was presumed to be due to SSc-ILD. Physical examination showed stable vital signs, dry cough and bilateral fine crackles over the lower lung fields. Cutaneous examination revealed no worsening of skin sclerosis nor digital ulcers. Chest HRCT revealed subpleural reticular shadows at both lung bases typically seen in SSc-ILD, showing no progression from previous imaging. However, reticulation and centrilobular nodules were also observed throughout the lung fields, suggesting a different underlying aetiology (Fig. 1A). A thorough review for SSc-related and myositis-related autoantibodies utilizing A-Cube [4], a multiplex autoantibody array assay, revealed no additional findings.
Given the patient’s continuous working in the cleaning industry for many years, which involved exposure to pigeon feathers and droppings, as well as the use of feather bedding, bird-related HP was suspected. Serum positivity of specific IgG antibodies against pigeon (26 mg_A_/l) and budgerigar antigens (23 mg_A_/l) were demonstrated by ImmunoCAP^®^ assay (ThermoFisher Scientific, Waltham, MA, USA). Repeated mPSL pulse therapy achieved clinical improvement, as well as resolution of upper lung ground-glass opacities, and the percent predicted diffusing capacity of the lungs for carbon monoxide (%DL_CO_) increased from 80% to 89% (Fig. 1B). The patient was discharged on oral PSL 20 mg/day. Despite detailed instructions on antigen avoidance, the patient’s dry cough exacerbated post-discharge, indicating ongoing exposure and recurrent HP. She confessed that she was still working as a cleaner and had not removed the feather bedding. After repeated instructions on antigen avoidance, her symptoms improved 11 months after the last mPSL pulse therapy. Currently, PSL has been tapered off without symptom flare-ups.
Diagnosing HP is challenging in patients with overlapping autoimmune diseases such as SSc, which can independently cause ILD. ATA-positive SSc patients often have severe ILD and diffuse skin sclerosis, leading to poor prognosis [5]. However, the patient’s long survival may reflect the better prognosis associated with ATA-positive lcSSc [6]. In this case, HRCT findings were one of the key clues for suspecting HP overlapping with SSc-ILD (Fig. 1B). While both HP and SSc-ILD exhibit lung fibrosis, HP is characterized by centrilobular reticulations predominantly in the upper lung fields, reflecting its transairway pathology, whereas SSc-ILD primarily affects the lower lung fields.
Recently, serological assays such as ImmunoCAP**^®^** assay have emerged as novel tools in the diagnosis of HP [4]. Although cross-reactivity with other bird species has been reported due to shared avian antigens [7], not all potential HP-associated antigens can currently be tested. Serology is also unavailable for drug-induced HP, such as cases caused by methotrexate. Furthermore, false-negative results are common [7, 8]; thus, a negative test does not exclude HP, while a positive test merely indicates past exposure. Therefore, clinicians must maintain a high index of suspicion, carefully considering the exposure history, clinical features, and radiologic findings. Comprehensive assessment incorporating all these elements remains essential for accurate diagnosis [1, 2].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tomioka H , Miyazaki Y, Inoue Y et al; Committee of Japanese Respiratory Society for Japanese Clinical Practice Guide 2022 for Hypersensitivity Pneumonitis. Japanese clinical practice guide 2022 for hypersensitivity pneumonitis. Respir Investig 2024;62:16–43.10.1016/j.resinv.2023.07.00737931427 · doi ↗ · pubmed ↗
- 2Raghu G , Remy-Jardin M, Ryerson CJ et al Diagnosis of hypersensitivity pneumonitis in adults: an official ATS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med 2020;202:e 36–e 69.32706311 10.1164/rccm.202005-2032 STPMC 7397797 · doi ↗ · pubmed ↗
- 3Lacasse Y , Selman M, Costabel U et al; HP Study Group. Classification of hypersensitivity pneumonitis: a hypothesis. Int. Arch. Allergy Immunol 2009;149:161–6.19127074 10.1159/000189200 · doi ↗ · pubmed ↗
- 4Kuzumi A , Norimatsu Y, Matsuda KM et al Comprehensive autoantibody profiling in systemic autoimmunity by a highly-sensitive multiplex protein array. Front Immunol 2023;14:1255540.37701440 10.3389/fimmu.2023.1255540 PMC 10493387 · doi ↗ · pubmed ↗
- 5Santos CS , Morales CM, Castro CÁ, Álvarez ED. Clinical phenotype in scleroderma patients based on autoantibodies. Rheumatol Adv Pract 2023;7:i 26–i 33.36968636 10.1093/rap/rkad 010PMC 10036993 · doi ↗ · pubmed ↗
- 6Kranenburg P , van den Hombergh WMT, Knaapen-Hans HKA et al Survival and organ involvement in patients with limited cutaneous systemic sclerosis and anti-topoisomerase-I antibodies: determined by skin subtype or auto-antibody subtype? A long-term follow-up study. Rheumatology 2016;55:2001–8.27520796 10.1093/rheumatology/kew 298 · doi ↗ · pubmed ↗
- 7Shirai T , Tanino Y, Nikaido T et al Screening and diagnosis of acute and chronic bird-related hypersensitivity pneumonitis by serum Ig G and Ig A antibodies to bird antigens with Immuno CAP®. Allergol Int 2021;70:208–14.33041192 10.1016/j.alit.2020.09.003 · doi ↗ · pubmed ↗
- 8Shiroshita A , Tanaka Y, Nakashima K, Furukawa Y, Kataoka Y. Diagnostic accuracy of specific Ig G antibodies for bird fancier’s lung: a systematic review and meta-analysis. Ann Transl Med 2019;7:655.31930056 10.21037/atm.2019.10.65PMC 6944612 · doi ↗ · pubmed ↗