ICM Implantation and Remote Follow‐Up Management by Trained Nurses in Italian Hospitals: Current Practice and Nurse Feedback
Rosario Cervellione, Simona Fetche, Marzia Simoncelli, Paola Frasnelli, Maurizio Vargiu, Cinzia Messina, Emanuele Contu, Anna Bertazzo, Eleonora Baccolo, Marco Carconi, Francesco Cropanese, Cristina Spina, Donato Montanaro, Annalisa Mercurio, Giuliana Facchetti

TL;DR
This study explores how trained nurses in Italy are currently managing implantable cardiac monitor implantations and remote follow-ups, highlighting both progress and challenges in standardizing these practices.
Contribution
The study provides insights into nurse-led ICM practices in Italy and identifies the lack of standardized protocols as a barrier to wider adoption.
Findings
60% of nurses reported being authorized to perform ICM implantations in their hospitals.
Only 33% of hospitals had written protocols for ICM implantation.
84% of implanter nurses achieved autonomy after fewer than 10 supervised implants.
Abstract
This project aimed to evaluate current practices of trained nurses performing implantable cardiac monitor (ICM) implantations and remote follow‐ups in Italy, assessing hospital protocols and nurses' perceptions. An anonymous survey was conducted among 163 trained nurses across 75 Italian hospitals, focusing on their ICM implantation and remote monitoring practices. Data collected included hospital characteristics and protocols, barriers to implementation, and nurses' feedback on their experiences. Of the 112 respondents (69% response rate), 60% reported that nurses in their hospitals are authorized to perform ICM implantations, and 70% said that they can manage all remote monitoring tasks. Thirty‐three (29%) nurses manage all aspects of ICM patient care, including implantation, programming, enrollment in remote monitoring, training, data review, and follow‐up. Fifty‐five percent of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
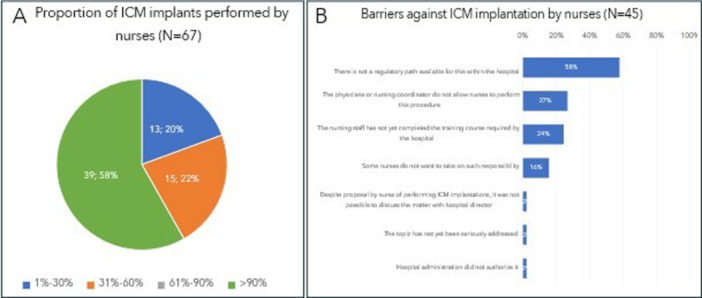 Figure 1
Figure 1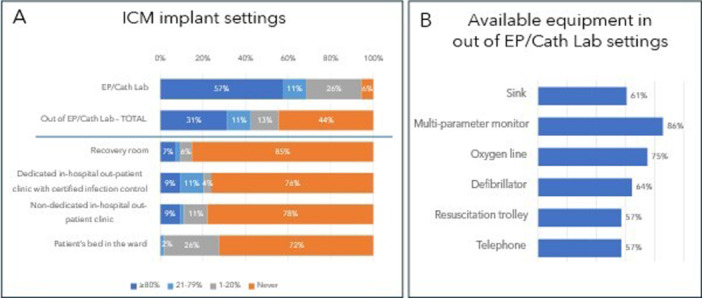 Figure 2
Figure 2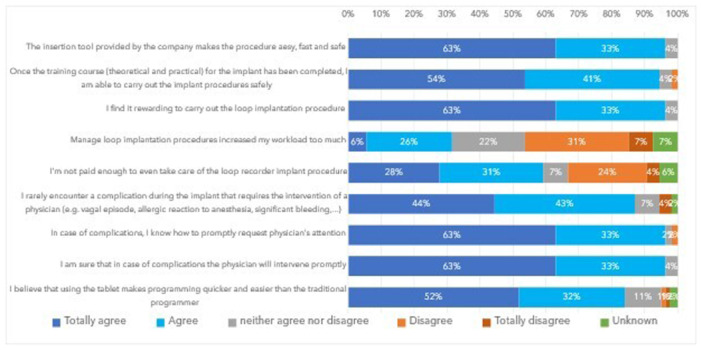 Figure 3
Figure 3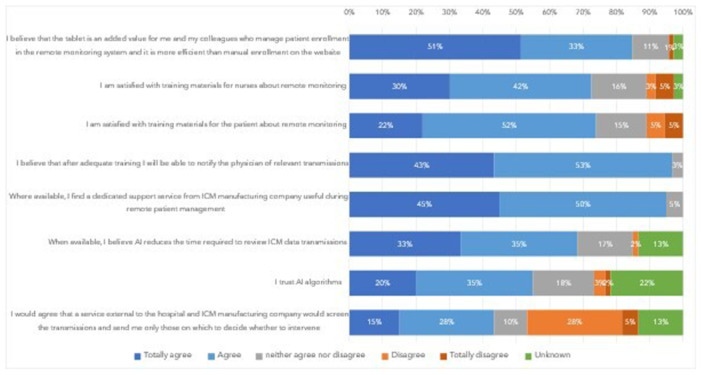 Figure 4
Figure 4| Item |
| % |
|---|---|---|
| Geographical area ( | ||
| Nord | 46 | 41 |
| Center | 9 | 8 |
| South and Island | 57 | 51 |
| Type of hospital where nurse works ( | ||
| Public | 100 | 89 |
| University public | 10 | 9 |
| Affiliated private | 2 | 2 |
| Number of ICM implants/year at hospital ( | ||
| 10–20 | 7 | 6 |
| 20–50 | 55 | 49 |
| > 50 | 47 | 42 |
| Unknown | 3 | 3 |
| ICM brand implanted at hospital ( | ||
| Medtronic | 109 | 97 |
| Biotronik | 73 | 65 |
| Abbott | 43 | 38 |
| Boston Scientific | 8 | 7 |
| ICM implanted by nurses at hospital ( | ||
| Yes | 67 | 60 |
| No | 45 | 40 |
| Additional operators involved in ICM implants performed by nurses ( | ||
| Implanter nurse is alone | 18 | 27 |
| 1 Allied healthcare professional (nurse/healthcare assistants or cardiology technicians) | 26 | 39 |
| 1 Physician | 7 | 10 |
| 1 Physician + 1 allied healthcare professional | 13 | 19 |
| 2 Allied healthcare professionals | 3 | 5 |
| ICM explanted by nurses at hospital ( | ||
| Yes | 34 | 30 |
| No | 78 | 70 |
| Availability of SOP on nurse‐led ICM implantation at the hospital where nurses can implant ( | ||
| Yes | 22 | 33 |
| No | 45 | 67 |
| Definition of minimum number of ICM implantation procedures by nurse before being considered autonomous ( | ||
| Yes | 24 | 36 |
| No, the supervisor decides when nurse autonomy is achieved | 43 | 64 |
| Defined minimum number of implants by nurse with a supervisor before autonomy ( | ||
| 3 | 2 | 8 |
| 5 | 8 | 34 |
| 10 | 2 | 8 |
| ≥ 20 | 12 | 50 |
| Written documentation of ICM performed by nurses under supervision + date of achieved autonomy at the hospital ( | ||
| Yes | 25 | 37 |
| No | 42 | 63 |
| Need for periodic reassessment of nurses to continue implanting ICMs ( | ||
| Yes | 15 | 22 |
| No | 52 | 78 |
| Written tracking system of peri‐procedural complications at the hospital ( | ||
| Yes | 56 | 50 |
| No | 56 | 50 |
| ICM complication monitoring methods ( | ||
| Education of patient about possible complications and ask him to report them by phone if they occur | 63 | 56 |
| Schedule a visit after implantation to check wound | 52 | 46 |
| Patient interview about ICM complication occurrence during in‐office or telephone follow‐ups | 30 | 27 |
| Nurse manages ICM programming (according to physician indications) at his hospital ( | ||
| Yes, alone | 77 | 69 |
| Yes, together with a cardiology technician | 8 | 7 |
| No, a cardiology technician manages it | 11 | 10 |
| No, a physician manages it | 16 | 14 |
| Item |
| % |
|---|---|---|
| Geographical area ( | ||
| Nord | 25 | 46 |
| Center | 7 | 13 |
| South and Island | 22 | 41 |
| Number of ICM implants/year at hospital ( | ||
| 10–20 | 4 | 7 |
| 20–50 | 24 | 44 |
| > 50 | 26 | 48 |
| Experience in cardiac pacing area ( | ||
| < 1 year | 2 | 4 |
| 1–3 years | 6 | 11 |
| > 3 years | 46 | 85 |
| Reason to be trained and involved as ICM implanter ( | ||
| It was an imposition by hospital | 1 | 2 |
| Other nurses do it and I do not want to be outdone | 0 | 0 |
| I consider it a professional growth | 49 | 91 |
| I do it, but I would like to be recognized | 24 | 44 |
| Number of ICM implants with supervisor before autonomy ( | ||
| < 5 | 28 | 52 |
| 5–10 | 17 | 32 |
| 10–20 | 4 | 7 |
| > 20 | 5 | 9 |
| Any implantation outside the EP/Cath Lab ( | ||
| Yes | 30 | 55 |
| No | 24 | 45 |
| Physician location during ICM implantation ( | ||
| Same room | 13 | 24 |
| Nearby room | 17 | 31 |
| On the same floor | 21 | 39 |
| In another floor | 3 | 6 |
| Implanter nurse clothing during ICM implantation ( | ||
| Cap | 48 | 89 |
| Surgical mask | 54 | 100 |
| Aseptic gown | 50 | 93 |
| A pair of sterile gloves | 47 | 87 |
| 2 Pairs of sterile gloves | 7 | 13 |
| Protective glasses | 15 | 28 |
| EKG patient monitoring during ICM implantation ( | ||
| Yes | 38 | 73 |
| No | 16 | 27 |
| Patient venous access creation before ICM implantation ( | ||
| Yes | 36 | 69 |
| No | 18 | 31 |
| Temporary stop OAC therapy ( | ||
| No | 31 | 57 |
| Yes, 12 h before ICM implantation | 4 | 7 |
| Yes, 24 h before ICM implantation | 16 | 30 |
| Yes, 48 h before ICM implantation | 3 | 6 |
| Peri‐procedural antibiotic therapy ( | ||
| No | 27 | 50 |
| Yes, in all patients | 19 | 35 |
| Yes, in patients with high infection risk | 8 | 15 |
| Local anesthetic drugs ( | ||
| Mepivacaine | 28 | 52 |
| Lidocaine | 24 | 44 |
| Ropivacaine | 4 | 7 |
| Sodium bicarbonate | 1 | 2 |
| Use of the injection kit provided by the manufacturer ( | ||
| Only the injection kit | 50 | 93 |
| Injection kit + additional scalpel | 4 | 7 |
| Adherence to ICM implant position and orientation in the patient chest manufacturer guidelines ( | ||
| Yes, if patient's anatomy allows it | 29 | 54 |
| Yes, if patient anatomy allows it, but with exception of women with breast implants | 18 | 33 |
| No, pre‐implant ECG mapping is performed | 4 | 7 |
| No, decision per implanter discretion | 3 | 6 |
| Wound closure methods ( | ||
| Steri‐Strips | 30 | 56 |
| Absorbable stitches | 25 | 46 |
| Nonabsorbable stitches | 18 | 33 |
| Skin glue | 5 | 9 |
| Wound dressings ( | ||
| Medicated transdermal patches | 45 | 83 |
| Medicated transdermal patches + application of ice and weight | 1 | 2 |
| Advanced dressings (e.g., silver‐impregnated dressings) | 4 | 7 |
| Compressive dressings | 8 | 15 |
| Common gauze and plaster | 1 | 2 |
| Item |
| % |
|---|---|---|
| Number of ICMs managed through remote monitoring at hospital ( | ||
| < 50 | 31 | 28 |
| 50–200 | 51 | 45 |
| 200–500 | 23 | 21 |
| > 500 | 7 | 6 |
| % of implanted ICM provided with remote monitoring ( | ||
| < 25% | 7 | 6 |
| 25%–50% | 3 | 3 |
| 50%–75% | 5 | 4 |
| 75%–95% | 10 | 9 |
| > 95% | 87 | 78 |
| The nurse manages patient enrollment in remote monitoring system at the hospital ( | ||
| Yes | 83 | 74 |
| No, a cardiology technician manages it | 13 | 12 |
| No, a physician manages it | 16 | 14 |
| Enrollment of patient in remote monitoring system at hospital ( | ||
| At implant | 99 | 88 |
| After implant, but pre‐discharge | 13 | 12 |
| The nurse manages patient training about remote monitoring and symptom recording at the hospital ( | ||
| Yes | 84 | 75 |
| No, a cardiology technician manages it | 11 | 10 |
| No, a physician manages it | 15 | 13 |
| No, an external service provided by ICM manufacturer manages it | 2 | 2 |
| Possibility to withdraw remote monitoring in the patient informed consent form of the hospital ( | ||
| Yes | 44 | 39 |
| No | 68 | 61 |
| The nurse performs first review of remote data transmissions and notifies the physician about the relevant one, at the hospital ( | ||
| Yes | 82 | 73 |
| No, a cardiology technician manages it | 18 | 16 |
| No, a physician manages it | 12 | 11 |
| Availability of SOP of the hospital indicating which transmissions/events need to be notified to the physician ( | ||
| Yes | 19 | 17 |
| No, but nurse and physician agree on which transmissions/events need to be notified | 69 | 62 |
| No, a physician reviews ICM transmissions | 12 | 11 |
| Unknown | 12 | 11 |
| Type of transmissions to be notified to the physicians ( | ||
| All transmissions containing arrhythmic episodes | 15 | 13 |
| Transmissions containing new and dubious arrhythmic episodes | 41 | 37 |
| Transmissions containing new and non‐managed arrhythmic episodes | 24 | 21 |
| Unknown (interviewed nurse not involved in transmission review) | 32 | 29 |
| ICM patients with tool (activator/App) for recordings of symptoms ( | ||
| > 75% | 58 | 52 |
| 25%–75% | 25 | 22 |
| < 25% | 29 | 26 |
- —The authors received no specific funding for this work.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Cardiac Arrhythmias and Treatments · ECG Monitoring and Analysis
Introduction
1
Implantable loop recorders (ILRs) are recommended by international guidelines [1, 2] for diagnosing unexplained syncope or falls, palpitations, cryptogenic stroke and monitoring atrial fibrillation recurrence following AF ablation, as they offer a higher diagnostic yield than intermittent monitoring tools [3, 4]. The latest ILR generation has been miniaturized and redefined as insertable cardiac monitors (ICM), allowing a minimally invasive insertion under the skin using a dedicated tool [5, 6, 7, 8].
In recent years, nursing skills in cardiology have evolved beyond historical responsibilities, especially in telecardiology and interventional electrophysiology, with a special focus on cardiac pacing and related monitoring services. Reports have shown that trained arrhythmia nurses can safely implant ICMs autonomously [9, 10, 11, 12, 13, 14, 15, 16, 17]. Moreover, nurse‐led ICM implantations have been as safe and effective as EP‐led ones [8, 9, 10, 11, 12, 13, 17] while also improving hospital efficiency [9, 11, 12] and reducing costs, particularly when procedures move from the electrophysiology or catheterization laboratory (EP/Cath lab) to out‐patient settings [11, 12].
In response to the growing number of UK hospitals allowing non‐medical staff to perform ICM implantation, the British Heart Rhythm Society (BHRS) released evidence‐based guidance in 2018, updated in 2020 [18], providing minimum standards for safe ICM implantation and management by nurses or cardiac physiologists. Following this success, in Italy, ICM manufacturers conceived training centers in selected hospitals, for nurses to receive theoretical and practical training by electrophysiologists or expert nurses on ICM indication, implantation, and remote monitoring. However, no guidelines from the Italian Arrhythmology and Cardiac Pacing Association have been published, leading some hospitals to create internal standard operating procedures (SOP) to authorize trained nurses to implant ICMs and/or manage remote follow‐ups, while others allow this only under electrophysiologist responsibility.
Our project aimed to assess the rate of trained nurses currently performing ICM implantation and remote follow‐up in Italian hospitals, and to characterize hospital protocols and current practice. Additionally, we sought to investigate the nurse's perception and gather feedback on aspects of current practice, including the ease and safety of ICM implantation, confidence and satisfaction with their new responsibilities, implant tools, ICM programmer/remote monitoring systems, and training materials.
Methods
2
This project was based on a survey sent to nurses who have received a training course about ICM implantation and remote follow‐up in Italy.
The survey was fully anonymous, and no sensitive data were collected or managed. Participation of survey recipients was voluntary. The project was conducted in accordance with local laws and regulations.
Project Phases
2.1
In October 2023, an Expert Nurse Focus Group (ENFG) of 15 expert nurses in cardiac pacing, each with over 2 years of experience in ICM implantation and/or remote monitoring, met to share best practices. Four electrophysiologists also attended to support the group. During the meeting, the ENFG designed a survey to gather current practice and feedback from nurses who had previously trained in ICM implantation and management.
The survey was designed to collect data on:
- −the percentage of trained nurses allowed to perform ICM implantation and/or remote follow‐ups at their hospital, barriers to implementation, existing hospital SOP, and current practices in Italian hospitals,
- −nurses' perceptions of the ease and safety of ICM implantation, satisfaction and confidence in this new role, and feedback on tools and trainings.
A draft of the questionnaire was created during the meeting and shared by email with all participants to refine and finalize all the questions. An electronic form was developed using Fillout.com service and invitations to participate were sent three times between November 2023 and March 2024 to the e‐mail addresses of all nurses who had previously attended an ICM training course. The service saves the survey responses only if all questions have been answered. Data collection closed in April 2024 and responses were processed.
Survey Structure
2.2
The survey included 65 multiple choice and ranking questions covering (see Appendix A): (1) Hospital information and available standard operating procedures (SOP) for nurse ICM implantation; (2) Nurse experience; (3) Nurse current practices about ICM implant procedure, settings, and materials; (4) Nurse feedback and satisfaction with ICM implantation; (5) ICM remote monitoring, available SOP and nurse involvement; and (6) Nurse feedback about patient enrollment in the remote monitoring system, training materials for nurses, and patients and ICM data transmission review.
Statistics
2.3
The results of the survey were presented with descriptive statistics. Categorical variables were expressed as counts and percentages. The chi‐square test for categorical variables was used to assess the significance of differences between groups. Statistical test deemed statistically significant if p < 0.05. All analyses were performed using SAS 9.4 version software (SAS Institute Inc., Cary, NC, USA).
Results
3
The survey was sent by e‐mail to 163 nurses (from 75 Italian hospitals) who completed training on ICM implantation and remote follow‐up. By the end of data collection, 112 nurses responded, representing a 69% response rate. Of these, 86 (77%) had over 3 years of experience in the cardiac pacing area, 17 (15%) between 1 and 3 years, and 9 (8%) less than 1 year.
ICM Implantation by Trained Nurses
3.1
Hospital Information and Available SOP on Nurse‐Led ICM Implantation
3.1.1
Table 1 reports characteristics of hospitals where survey respondents work and available SOP for nurse‐led ICM implantation. Over half of responding nurses (51%) are from southern Italy or the islands, 41% from the north, and 8% from the center. Public hospitals represented 89%, with 42% categorized as high‐volume and 49% as medium‐volume ICM implant centers. Seventy‐nine nurses (70%) have access to multiple ICM technologies.
Sixty‐seven nurses (60%) indicated that trained nurses currently implant ICMs at their hospital, while 34 (30%) also explant them. Figure 1 illustrates the proportion of ICM implants performed by trained nurses in the hospitals where nurses can implant ICMs (panel A) and barriers faced in hospitals where they are not allowed to implant. In hospitals where nurses implant ICMs, 29% require physician attendance.
Proportion of ICM implants performed by trained nurses in the hospitals where nurses implant ICMs (A) and barriers against ICM implantation by trained nurses in the hospitals where nurses are not allowed to implant ICMs (B).
Among hospitals where nurses implant ICMs, 22 (33%) survey respondents reported the availability of SOP for this purpose. Additionally, 36% (64% in sites with SOP and 22% in sites without SOP) reported a minimum number of supervised implants (by an electrophysiologist or highly experienced nurse in ICM implantation) required for autonomy, with 37% (77% in sites with SOP and 18% in sites without SOP) reporting the availability of written documentation of these procedures and date of achieved autonomy. The minimum number of required supervised implants ranges from 3 (8%) or 5 (34%) to ≥ 20 implants (50%). Fifteen nurses (22%) indicated that a periodic reassessment by a supervisor is necessary to continue implanting ICMs.
A tracking system of peri‐procedural complications, including those related to ICM implantation, is available in the hospital of 50% of the total survey respondents. Complication monitoring strategies include educating patients about possible complications and reporting by phone (56%), scheduling follow‐up visits (46%) for wound check from 7 (34, 30%) to > 15 days (4%) days after implantation and patient interview during in‐office or telephone follow‐ups (27%).
Information About ICM Implanter Nurses and Current Practices
3.1.2
Out of 112 surveyed nurses, 54 (50%) perform ICM implantation at their hospital. Of these, 33 (29%) also manage all other aspects of ICM patient care, including ICM programming, enrollment in remote monitoring, training, data review, and follow‐up. Details on ICM implanter nurses and their practices are reported in Table 2. Most implanter nurses work at high‐volume sites (48%) and are located both in the north (46%) and in the south or islands (41%) of Italy. Eighty‐five percent have over 3 years of cardiac pacing experience, with 57% having performed more than 20 ICM implants. For 28 (52%) implanter nurses, fewer than 5 supervised implants were needed to achieve autonomy, while 9 (16%) required ≥ 10 implants. Fifty‐one (94%) nurses reported that no patients have ever refused to be implanted by a nurse.
Regarding ICM implant location (Figure 2A), 29 (55%) nurses use settings outside of the EP/Cath lab for all or part of ICM implants and 17 (31%) use this as the primary location (> 80% of implants performed there). On the other hand, 57% still predominantly use the EP lab/Cath lab. Figure 2 also reports the equipment available in out of EP/Cath lab settings (Figure 2B): when not present in the implanting room, resuscitation equipment is always nearby. During nurse‐led ICM implantation, a physician is in the same room for only a quarter of cases (24%), while he is often in a nearby room (33%) or on the same floor (36%).
Implant settings where nurses perform ICM implantation (A) and available equipment in non‐standard setting (B).
During ICM implantation, it is nurse's common practice (73%) to monitor patient's electrocardiogram (EKG) with a multiparameter monitor and to establish venous access beforehand (69%). These practices are more frequent for nurses who only implant in the EP/Cath lab (100% vs. 53% for EKG monitoring; p < 0.01% and 88% vs. 53% for venous access; p < 0.01). For patients on anticoagulants, 57% of nurses do not stop the therapy, while others typically stop it 24 h (30%), 12 h (7%), or 48 h (6%) before the procedure. Fifty percent of implanter nurses do not administer peri‐procedural antibiotics for ICM implants, while 35% give them to all patients and 15% only to those at high infection risk. All nurses use the manufacturer's implantation kit, though four (8%) use an additional scalpel; most (87%) follow manufacturer guidelines for ICM position and orientation in the patient's chest, but for 33% of them, an exception should be considered for women with breast implants. Preferred wound closure methods are Steri‐Strips (56%), absorbable (46%), and nonabsorbable (33%) stitches, and the most common dressing is medicated transdermal patches (85%) (Table 2).
After implantation, nurses perform ICM programming, following physician's indications, in the hospitals of 76% of surveyed ones, while 10% have a cardiology technician doing it, and 14% have a physician handle it (Table 1).
Nurse Feedback and Satisfaction on ICM Implantation
3.1.3
Among 54 nurses who perform ICM implantations, 49 (91%) chose this role for professional growth, while 24 (44%) seek recognition for this activity, and 1 nurse (2%) had this decision imposed by the hospital (Table 2). For 30 (56%) nurses, professional growth was the sole reason for their choice. As shown in Figure 3, nurse feedback about ease and safety of ICM implantation procedure, confidence in performing it and in managing potential complications, and about the programmer tablet was positive for the majority. Most nurses consider ICM implantation a rewarding activity, although the increased workload and the lack of additional compensation are concerns for 31% and 59% of them, respectively.
Nurse feedback and satisfaction on ICM implantation.
ICM Remote Monitoring by Trained Nurses
3.2
Hospital Information and Available SOP on Nurse‐Led ICM Remote Monitoring
3.2.1
Table 3 displays hospital characteristics and available SOP for ICM remote monitoring by trained nurses. Over 70% of surveyed nurses reported that their hospital allows nurses to handle patient enrollment in the remote monitoring website (74%), provide them training on remote monitoring and recording activation during symptoms (75%) and/or conduct initial review of ICM data transmissions (73%). In contrast, these tasks are assigned to physicians in 14%, 13%, and 11% of cases, respectively. A cardiology technician manages remote monitoring in most other instances, while in only 2% of cases, patient training is handled by an external service provided by ICM manufacturer. In the hospital of 69 (62%) interviewed nurses, no SOP exists to indicate which ICM data transmissions should be notified to physicians after the first nurse review. However, it is the current practice of 41 (37%) nurses to notify all transmissions with new or questionable arrhythmic episodes, of 24 (21%) to notify arrhythmic episodes only when no clinical action has been taken yet (e.g., anticoagulant initiation), of 15 (13%) to notify all the transmission with episodes regardless of type or action. Additionally, 58 (52%) nurses provide the recording tool for symptoms to over 75% of ICM patients.
Nurse Feedback and Satisfaction on Training Materials and Remote Monitoring
3.2.2
Among the 112 interviewed nurses, 72 (64%) personally manage patient enrollment in the remote monitoring system, 73 (65%) provide patient training on ICM functioning, remote monitoring, and activation recording, and 60 (54%) review ICM data from the remote monitoring system. Figure 4 shows their feedback and satisfaction with remote monitoring tools and training materials. Eighty‐four percent find the tablet a more efficient tool for patient enrollment compared to manual method. Almost all nurses involved in remote data review feel confident in notifying physicians of relevant transmissions after adequate training and find the support from a dedicated service provided by the ICM manufacturer helpful. Two‐thirds believe that AI can reduce transmission review time, and 55% already trust AI algorithms. The use of an external service (to the hospital and to the ICM manufacturer) to screen ICM transmissions and to notify the hospital only the actionable ones is considered acceptable by 43%.
Nurse feedback and satisfaction on training materials and remote monitoring.
Discussion
4
In recent years, about 160 experienced nurses from over 75 sites in Italy have been authorized to attend training courses for ICM implantation and remote follow‐up management. Our survey of these trained nurses shows that nurse‐led ICM implantation and remote follow‐up are currently established practices in Italy, with all interviewed nurses managing at least one task related to this process. Approximately 30% of them are accountable for the complete management of patients with ICM, involving implantation, programming, enrollment in remote monitoring systems, patient training, and data transmission review. However, many hospitals lack SOP, leaving final responsibility and level of nurse involvement in ICM implantations and remote data review at the discretion of physicians.
ICM Implantation by Trained Nurse
4.1
Ease and Safety of the Procedure and Nurse Empowerment
4.1.1
The miniaturization of devices and the use of the dedicated implantation tool have made ICM implantation safely feasible by trained allied professionals [9, 10, 11, 12, 13, 14, 15, 16, 17]. Nurse‐led ICM implantation has been shown to improve hospital efficiency [9, 12, 13] and reduce costs, particularly in outpatient settings [12, 13]. Key findings from our survey indicate that 60% of Italian nurses trained in ICM implantation are allowed to perform the procedure at their hospital, with many performing over 90% of these procedures. Nurse implanters are well distributed across Italy. However, the lower proportion of survey respondents (8%) and implanter nurses (13%) from the center of Italy may reflect the lack of a training center in that area.
After the initial training, only 29% of nurses involve a physician during the procedure. In fact, a significant majority find the procedure easy, fast, and safe with the provided implantation kit. After adequate training, they feel prepared to safely carry out the procedure and manage potential rare complications (87% of nurses report rare occurrences) with prompt physician support, if necessary.
Nurse‐led ICM implantation results in nurse empowerment. More than 90% of implanter nurses consider ICM implantation rewarding and a form of professional growth, although the increased workload and the lack of additional compensation are concerns for some.
Lack of SOP
4.1.2
Nurse unwillingness to take on ICM implant responsibility was considered a barrier hindering this program only for a low percentage of respondents. The results of our survey show that the main obstacle is the lack of SOP in hospitals. Consequently, some physicians or nurse coordinators are afraid to take on the responsibility of authorizing nurse‐led implantation, which was reported as the second most important barrier in our survey. In the UK, as more centers allowed nurses or cardiac physiologists to perform ICM implants, BHRS issued evidence‐based guidance [18] to set minimum standards for their safe ICM implantation and management. On the contrary, in Italy and the rest of Europe, despite more centers adopting this strategy recently, scientific societies have not yet released guidelines, and hospital SOP remain non‐standardized, loosely based on BHRS standards [18]. Our survey shows that, regardless of available hospital SOP, most Italian hospitals/nurses are adhering to room, equipment, staffing, implantation tools and most of the procedure requirements of BHRS standards [18]. However, they often deviate from these standards, regarding the following aspects, that should be urgently addressed by national guidelines/standards to increase the adoption of this safe and cost‐saving strategy in Italy: the minimum number of 20 implants for assessing nurse competency, nurse competency reassessment if 20 procedures/year are not performed, the need of a hospital‐certified for infection‐control implantation room, uninterrupted oral anticoagulant therapy strategy during the procedure, the use of peri‐procedural antibiotics and the possibility of ICM explant procedure by nurses.
Number of Supervised Implants for Competency
4.1.3
We found that, in the practice of Italian sites, many nurses achieved autonomy after less than 10 supervised implants (52% after less than 5) and no reassessment is requested for about 80% of trained nurses, regardless of the amount of procedures/year. These results suggest, along with the infrequent occurrence of complications [9, 10, 11, 12, 13, 14, 15, 16, 17], even with only three to five supervised nurse procedures to assess competency [11, 12, 16], that shortening the practical training phase and avoiding yearly nurse reassessment could be considered by national guidelines to enable also low volume sites to implement nurse‐led implantation program and have autonomous implanter nurses more quickly.
ICM Implant Location
4.1.4
Another important finding of our survey is that 55% of nurses perform ICM implants also outside the EP/Cath lab, in a location typically equipped as indicated by BHRS standards [17], and for 31% of them, this setting is the primary choice. However, a dedicated outpatient clinic with hospital certification for infection control is not always available at the hospital and even the recovery room adjacent to the EP lab, a non‐dedicated out‐patient clinic and patient's bed in the ward are also used for ICM implantation by 15%, 22%, and 28% of nurses, respectively. Future national and international guidelines should consider that multiple published experiences of ICM implantation by nurses, performed in rooms non‐certified for infection control, have reported a low complication rate (≤ 2%) [10, 11, 13, 14, 17]. Therefore, ICM implantation in non‐certified infection control rooms should be allowed, provided that all necessary equipment are available and adequate infection control strategies are applied [17]. This could reduce the percentage of procedures performed in the EP/Cath lab, which currently serves as the primary procedure location for 57% of nurses, despite its lower efficiency and higher costs [9, 12, 13, 19].
Anticoagulation
4.1.5
Although BHRS guidelines [18] suggest that interrupting direct anticoagulants (DOACs) or vitamin K antagonists (VKA) before ICM implantation is generally unnecessary, 57% of Italian implanter nurses continue this practice. The primary risk for patients undergoing anticoagulation therapy during device implantation procedures is the development of a pocket hematoma, which can lead to serious consequences. This may require extended discontinuation of anticoagulation [20, 21], thereby heightening the risk of thromboembolism and infection [22, 23]. In patients on VKA anticoagulation undergoing pacemaker or defibrillator implantation, continuing VKA therapy without interruption significantly reduces pocket hematoma compared to interruption with heparin bridging, without increasing surgical or thromboembolic risks [20]. Additionally, pre‐procedural INR ≤ 2.5 in lower‐risk patients (CHA₂DS₂‐VASc ≤ 5, no mechanical heart valves, or severe mitral stenosis) and INR > 2 in higher‐risk patients significantly lowers hematoma and infection rates [24]. For patients on DOAC therapy, brief interruptions for procedures or surgery increased the risk of stroke/systemic embolism about threefold in trials comparing DOACs to VKAs [25, 26]. The BRUISE CONTROL‐2 trial showed that an uninterrupted DOAC strategy during pacemaker/defibrillator implantation is not inferior to interrupted DOACs regarding pocket hematoma and stroke incidence [27]. However, more recently, a minimal peri‐procedural DOAC interruption (no more than 24 h before and 12–24 h after the procedure) was found to be as safe as uninterrupted VKA therapy [28, 29]. During ICM implantation, the procedure is very brief [11, 12, 15] and far less traumatic than pacemaker or defibrillator implantation due to the smaller device size and simpler technique. Consequently, the risk of peri‐procedural bleeding or hematoma is very low [9, 12, 13, 15, 16, 17, 30]. Conversely, patients receiving an ICM for atrial fibrillation management or previous cryptogenic stroke often have a high thromboembolic risk. Reports of ICM implantation without anticoagulant interruption show very low rates of bleeding or hematoma [9, 16, 17, 19, 30]. Thus, it appears reasonable not to interrupt VKA (with INR on the day of surgery below the upper therapeutic range) or DOACs before ICM implantation, especially in high‐risk patients, as already currently recommended for pacemaker or defibrillator procedures [31, 32]. For low‐risk patients, minimally interrupted DOACs or VKA without heparin bridging (last dose the morning before the procedure, resumed 12–24 h later) is a safe alternative [32].
Use of Prophylactic Antibiotics
4.1.6
While BHRS considers the use of prophylactic antibiotics in high‐risk infection patients [18], current practices in Italy vary, with 15% administering them in high‐risk cases and 35% doing so in general. Several studies, with the use of prophylactic antibiotics in 28%–100% of cases, have reported a very low infection risk (≤ 1.1%) [9, 11, 12, 14, 16, 19, 30]. Additionally, a non‐randomized comparison of infection rates in ICM implantation procedures, with or without peri‐procedural antibiotic administration, confirmed that most procedures are performed without antibiotics in real‐world settings, with a similarly low infection risk (< 1%) [33]. Considering the potential for reduced global antibiotic efficacy, allergic reactions, and gastrointestinal complications from unnecessary use, it is reasonable to limit antibiotics to patients at high risk of infection.
ICM Explant Procedure by Trained Nurses
4.1.7
The BHRS recommends that ICMs be removed by a qualified practitioner, whether physicians, nurses, or physiologists, upon battery depletion [18]. However, only 30% of respondents to our survey reported that nurses are also authorized to perform ICM explantations at their hospitals. This may be due to limited evidence regarding the safety of ICM explant procedures performed by nurses. A retrospective single‐site study in Italy reported a 100% success rate for nurse‐led ICM explants, with no serious complications in 114 procedures performed by nurses in the EP lab with prophylactic antibiotics, compared to 88 procedures performed by electrophysiologists [34]. Two single‐site observational studies demonstrated that ICM explants or replacements can be safely performed outside of EP/Cath labs with short procedure times and no need for antibiotics, in 51 and 119 procedures, respectively, without infections or other complications [35, 36]. These findings suggest that such procedures could also be safely carried out by trained nurses. However, future multicenter comparative studies on the safety and cost‐effectiveness of nurse‐led vs. physician‐led ICM management should also include ICM explant procedures to confirm how nurses can safely manage the full ICM lifecycle.
ICM Remote Monitoring by Trained Nurse
4.2
For an optimal ICM diagnostic yield [37], patients should be enrolled in remote monitoring programs before discharge [38] (Class I, Level C recommendation), even if this can increase hospital workload for data review [39, 40] and require additional staff.
Our survey indicates that 72% of trained nurses work in hospitals with a significant number of remote‐monitored ICM patients, confirming the high workload that necessitates nurse involvement. Most likely for the same reason, nurses manage all phases of remote monitoring in over 70% of cases, even if SOP regarding roles and responsibilities are only present in 17%.
Italian current practice is to notify the physician with new arrhythmic episodes and questionable episodes (37%) or those not yet actioned (21%), while in a minority of cases all transmissions with episodes are notified (13%).
Our survey also shows high nurse confidence in reviewing remote data and notifying relevant information to the physician (97%) and high satisfaction (72%) about training materials on remote monitoring. Advancement in technology can facilitate nurse work, as demonstrated by 84% of surveyed nurses who overwhelmingly believe that tablet programmers make programming easier and faster and patient enrollment in the remote monitoring system more efficient compared to manual procedures. Nurses appreciate the dedicated technical support from manufacturers during remote patient management, while transmission screening by an external service [41] to the hospital and to the ICM manufacturer would be accepted only by 43% of nurses managing remote data review. AI holds promise for easing nurse workload because it reduces the number of transmitted false alerts that should be reviewed [42, 43, 44]. Though a significant portion (30%) had no opinion on AI effectiveness due to limited experience, 66% of nurses believe AI could reduce review times and 55% already trust the results of AI algorithms.
Limitations
4.3
The main limitations of our project stem from the voluntary nature of the survey. First, despite sending invitations to participate three times, we did not achieve a 100% response rate. Second, our sample may be subject to selection bias due to the predominance of public hospitals and limited representation from central Italy. However, our primary aim was to assess the rate of nurses currently performing ICM implantation and remote follow‐up among those trained, which our sample reflects. In addition, with nearly 70% participation, our results are representative of current practices among trained nurses in Italy. Third, although we could not verify survey responses in the clinical setting, the anonymity and voluntary nature of participation should have encouraged honest responses. Further studies comparing characteristics, organizational models, applied standard protocols, complication rates, and patient satisfaction at sites with and without nurse‐led implantation are needed to validate SOP for nurse‐led ICM implantation programs in both national and international multicenter settings.
Conclusions
5
While many Italian hospitals are motivated to train nurses in ICM implantation and remote management, only 60% allow trained nurses to perform implantations, and 71% can do so independently, without physician support. Over 70% of nurses are involved in remote patient management. The lack of regulations and SOP poses significant barriers to broader delegation of these responsibilities to nurses. Establishing clear guidelines at both national and international levels could standardize training and enhance awareness of effective practices, ultimately improving patient care in ICM management.
Ethics Statement
The survey was fully anonymous, and no sensitive data were collected or managed. Participation of survey recipients was voluntary. The project was conducted in accordance with local laws and regulations.
Consent
The authors have nothing to report.
Conflicts of Interest
Rosario Cervellione is a proctor for Medtronic, and Massimiliano Maines is a consultant and proctor for Medtronic, Boston Scientific, and Abbott. The other authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. Brignole , A. Moya , F. J. de Lange , et al., “Practical Instructions for the 2018 ESC Guidelines for the Diagnosis and Management of Syncope,” European Heart Journal 39 (2018): e 43–e 80.29562291 10.1093/eurheartj/ehy 071 · doi ↗ · pubmed ↗
- 2G. Hindricks , T. Potpara , N. Dagres , et al., “2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration With the European Association for Cardio‐Thoracic Surgery (EACTS): The Task Force for the Diagnosis and Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Developed With the Special Contribution of the European Heart Rhythm Association (EHRA) of the ESC,” European Heart Journal 42 (2021): 373–498.32860505 10.1093/eurh · doi ↗ · pubmed ↗
- 3G. Tsivgoulis , A. H. Katsanos , B. M. Grory , et al., “Prolonged Cardiac Rhythm Monitoring and Secondary Stroke Prevention in Patients With Cryptogenic Cerebral Ischemia,” Stroke 50, no. 8 (August 2019): 2175–2180, 10.1161/STROKEAHA.119.025169.31216964 · doi ↗ · pubmed ↗
- 4B. H. Buck , M. D. Hill , F. R. Quinn , et al., “Effect of Implantable vs Prolonged External Electrocardiographic Monitoring on Atrial Fibrillation Detection in Patients With Ischemic Stroke: The PER DIEM Randomized Clinical Trial,” Journal of the American Medical Association 325, no. 21 (June 2021): 2160–2168, 10.1001/jama.2021.6128.34061146 PMC 8170545 · doi ↗ · pubmed ↗
- 5T. T. Tomson and R. Passman , “The Reveal LINQ Insertable Cardiac Monitor,” Expert Review of Medical Devices 12, no. 1 (January 2015): 7–18, 10.1586/17434440.2014.953059.25154970 · doi ↗ · pubmed ↗
- 6N. Reinsch , A. Füting , D. Höwel , and K. Neven , “The BIOMONITOR III Injectable Cardiac Monitor: Clinical Experience With a Novel Injectable Cardiac Monitor,” Journal of Clinical Medicine 11, no. 6 (March 2022): 1634.35329960 10.3390/jcm 11061634 PMC 8954265 · doi ↗ · pubmed ↗
- 7N. S. Srivastava , J. Arruda , C. A. Haddadin , J. Ries , and C. Snyder , “Successful Modified Implantation of Insertable Cardiac Monitor in a Very Young Paediatric Patient,” Cardiology in the Young 33, no. 12 (December 2023): 2518–2520.36970856 10.1017/S 1047951123000434 · doi ↗ · pubmed ↗
- 8S. Fareh , S. Nardi , L. Argenziano , et al., “Implantation of a Novel Insertable Cardiac Monitor: Preliminary Multicenter Experience in Europe,” Journal of Interventional Cardiac Electrophysiology 67 (May 2024): 2117–2125.38755520 10.1007/s 10840-024-01821-y PMC 11711855 · doi ↗ · pubmed ↗