Self-Reported Socio-Economic and Psychological Burdens for Caregivers of Patients Undergoing Dialysis: A Cross-Sectional Study
Mandreker Bahall, Anuka D Harry, Anjali Kisseur, Vidal Ramdass, Dominique Gransaul, Sydney Alexander, Sacha Nandlal, George Legall

TL;DR
This study shows that caregivers of dialysis patients face significant stress, financial strain, and mental health challenges due to the demands of caregiving.
Contribution
The study provides new empirical data on the socio-economic and psychological burdens of caregivers in Trinidad and Tobago.
Findings
Most caregivers experienced anxiety, depression, and burnout, with 6.7% reporting suicidal thoughts.
Over 60% of caregivers struggled with work-life balance and financial worries.
Nearly half of caregivers rated their quality of life as 'less than good.'
Abstract
Background Patients undergoing dialysis require intensive treatment and supportive care, which affects their caregivers physically, socially, economically, and psychologically. However, this topic has been largely underexplored. Objectives This study aimed to examine the socio-economic and psychological burdens experienced by primary caregivers of patients undergoing dialysis. Method This cross-sectional study was conducted over 12 weeks using purposive sampling of primary caregivers of patients undergoing dialysis at two public and two private dialysis centers in Trinidad and Tobago. The questionnaire collected data on socio-demographics, economics, and selected psychological issues. Selected global health status questions adapted from the World Health Organization Quality of Life Brief Version were included. Participants were assured of confidentiality and anonymity. Verbal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
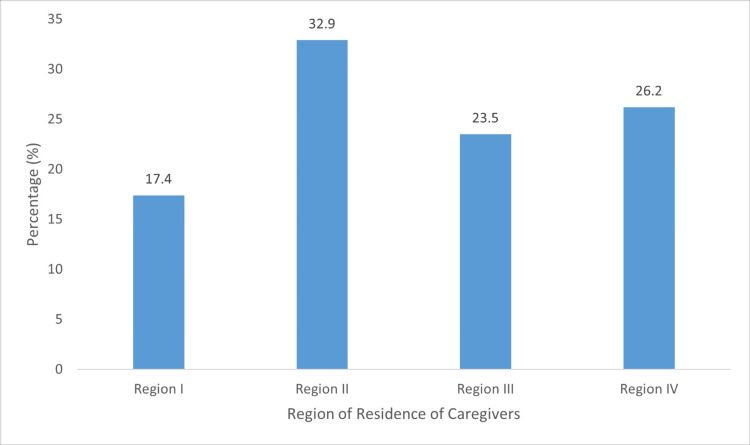 Figure 1
Figure 1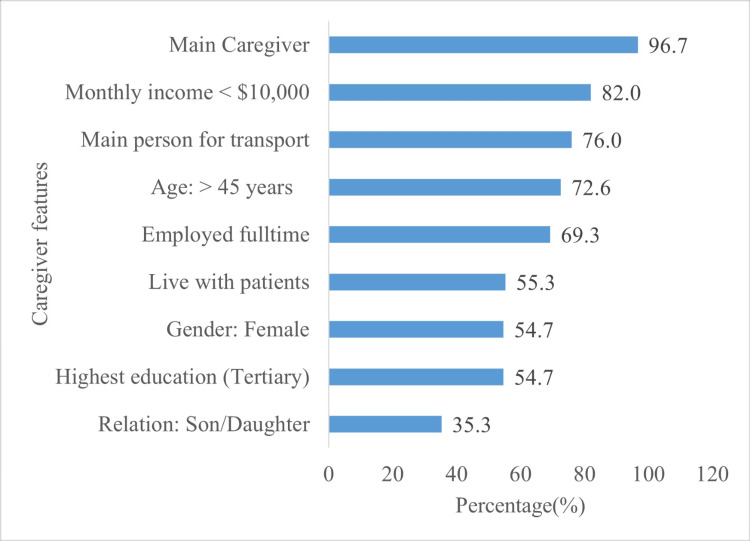 Figure 2
Figure 2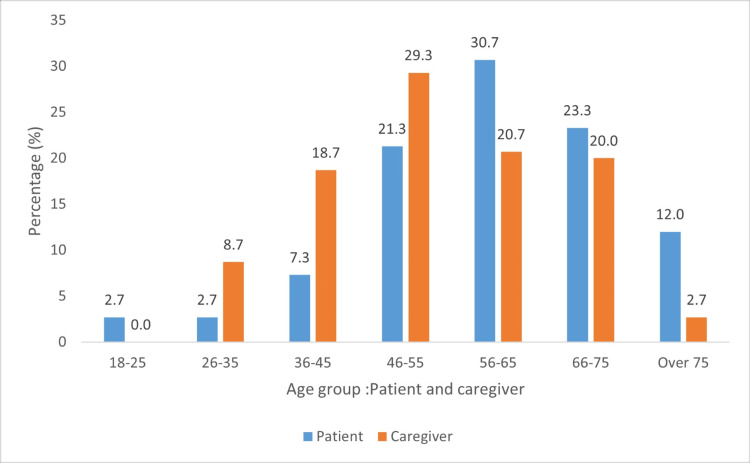 Figure 3
Figure 3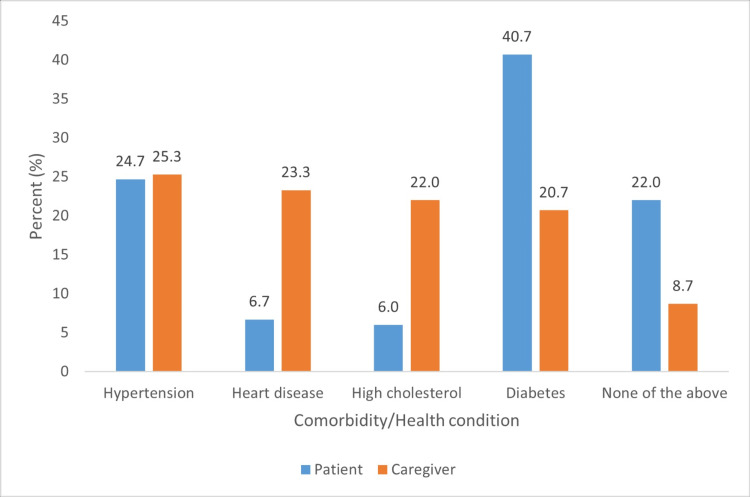 Figure 4
Figure 4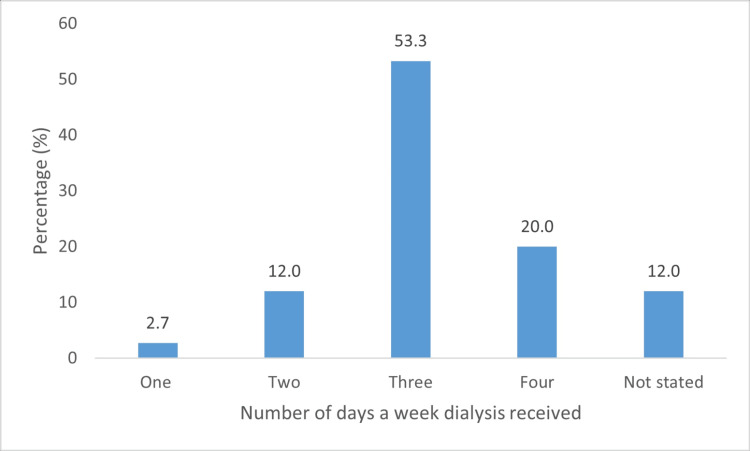 Figure 5
Figure 5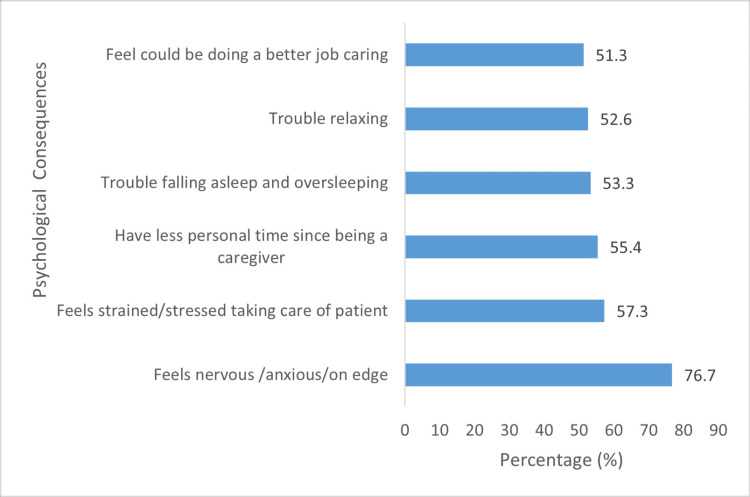 Figure 6
Figure 6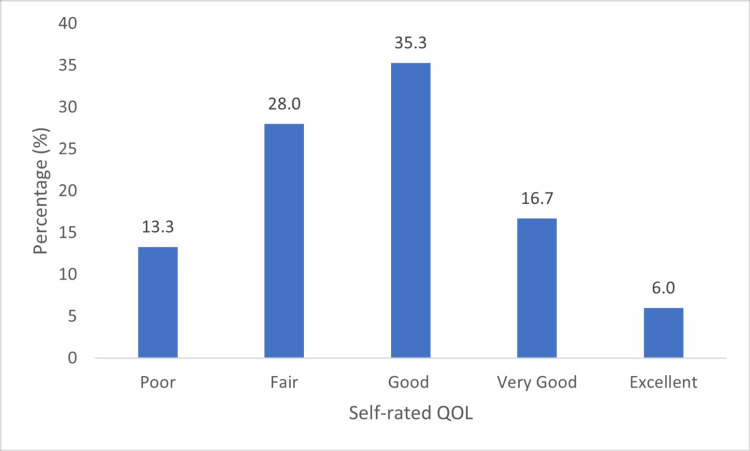 Figure 7
Figure 7| Variable | Rank | n | % |
| Hard to have a good work-life balance | 1 | 106 | 70.7 |
| Unable to attend many social events taking care of patient | 2 | 93 | 62.0 |
| Experienced judgment from others due to caregiver's role | 3 | 66 | 44.0 |
| Taking care of patients affected the closest relationships | 4 | 57 | 38.0 |
| I have good social support from family and/or friends | 5 | 54 | 36.0 |
| Spent less time on hobbies due to caregiving | 6 | 35 | 23.3 |
| I feel lonely as a result of taking care of the patient | 7 | 24 | 16.0 |
| QoL questions | Leading response | n | % |
| How would you rate your quality of life? | Less than good | 66 | 43.0 |
| Are you satisfied with your health? | No | 84 | 56.0 |
| How much do you enjoy life? | Rarely-Occasionally | 94 | 64.0 |
| To what extent do you feel your life to be meaningful? | Not at all-Rarely | 99 | 66.0 |
| Items | Type of scores | ||||
| Type of scores | Stress | Social | Financial | QoL | |
| Stress | 1 | 0.729** | -0.289** | -0.004 | |
| Social | 0.729** | 1 | -0.134 | -0.011 | |
| Financial | -0.289** | -0.011 | 1 | -0.137 | |
| QOL | -0.004 | -0.137 | -0.137 | 1 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFamily Caregiving in Mental Illness · Dialysis and Renal Disease Management · Intergenerational Family Dynamics and Caregiving
Introduction
End-stage renal disease (ESRD) is a common condition, accounting for a global prevalence of 4.902-7.083 million [1]. In Trinidad and Tobago, the prevalence is 875 per million population [2], one of the highest globally, and is reported in the annual report from the United States Renal Data System [3]. Dialysis is the primary treatment for preventing or minimizing ESRD-related complications. Caregivers of patients undergoing dialysis reported experiencing poorer quality of life (QoL) [4], psychological consequences [5], anxiety (27.8%), and depression (11.4%) [6]. According to Sajadi et al. [5], caregivers experience psychological pressure, isolation, and neglect, which adversely affect their mental and physical health. Ibrahim et al. [7] identified common caregiving burdens, including physical, psychological, social, and financial challenges. Factors such as caregiver demographics, disease-related variables, interpersonal relationships, social support, and psychological factors (e.g., depression and anxiety) contribute to this burden [8].
No studies have examined the socio-economic and psychological impacts on caregivers of patients undergoing dialysis in the Caribbean. This study aims to explore the socio-economic and psychological impacts on caregivers of patients undergoing dialysis, identify associations, and determine predictors. Given the global increase in ESRD cases [9], initiatives that support caregivers are increasingly crucial for understanding and improving their well-being.
Materials and methods
This cross-sectional study was conducted over 12 weeks (January to March 2024), due to time constraints and limited resources, and utilized purposive sampling to recruit the primary caregivers of patients undergoing dialysis. Trinidad and Tobago, a small resource-limited country, with 1.5 million people [10], has 14 dialysis centers, across its four health authorities. However, data were collected from two public and two private dialysis centers. The study sample was calculated as 150 participants using the formula below:
Sample Size = (Z value)^2^ *((p (1-p)) / (Margin of Error)^2^)
Purposive sampling was employed to ensure diverse caregiving experiences and viewpoints. Inclusion criteria involved caregivers aged 18 years or older and those serving as the primary caregivers for more than 50% of the time. Family members or individuals not directly involved in the patient's care were excluded. In healthcare, a primary caregiver is defined as any individual responsible for identifying, preventing, or treating an illness or disability [11]. Potential participants were assured of the anonymity and confidentiality of all information, briefed on the aim and nature of the study, and informed of their right to withdraw at any time. Participants who provided written consent were eligible to participate after fulfilling the inclusion and exclusion criteria. A self-made questionnaire was used to collect data on socio-demographics (27), economic status (six), social status (seven), and selected psychological issues (15). Questionnaires were distributed to caregivers present at the dialysis centers and entrusted to patients to be forwarded to their primary caregivers, or through an online platform.
Completed questionnaires (see Appendix) were stored in secure lockers, whereas digital data collected via Google Docs were accessible only through password-protected devices. Only the study group members and supervisor had access to view, edit, or comment.
The questionnaire included patient socio-demographics, dialysis treatment and duration, and caregiver characteristics, including age, sex, employment status, ethnicity, education level, and health conditions. These factors were examined in relation to economic, social, and psychological consequences. Descriptive statistics included frequency and percentage distribution tables, means, and standard deviations. Inferential analysis was conducted using 95% confidence intervals and hypothesis testing (chi-square tests of association and analysis of variance). All hypotheses were tested at a 5% level of significance.
Global health status scores were identified using four selected questions: “How would you rate your quality of life?”, “Are you satisfied with your health?”, “How much do you enjoy life?”, and “To what extent do you feel your life is meaningful?” Information is presented in tables and bar graphs, and percentages are categorically determined based on the social, economic, and psychological impacts on caregivers.
Ethical approval was obtained from the Ethics Committee of the University of the West Indies, Trinidad and Tobago, on December 13, 2023 (Ref: CREC-SA.2416/11/2023), and the Eastern Regional Health Authority and North Central Health Authority of Trinidad and Tobago on February 15, 2024, and March 15, 2024, respectively. All the participants voluntarily provided written informed consent to participate in this study. Participants were notified of the confidentiality of the data and their right to withdraw from the study.
Results
Socio-demographics
Data were collected from 150 caregivers from two public and two private dialysis centers, in four health regions. Figure 1 presents the respective percentage distributions.
Health region of residences of caregivers
Patient and caregiver characteristics
The majority of patients were men (n = 82, 54.7%) and belonged to the 46-75 age group (n = 113, 75.3%). Most caregivers were either the sole or primary caregivers. Other caregiver characteristics included being female, over 45 years of age, employed full time, and having at least a tertiary-level education. Moreover, more than half of the caregivers lived with the patient (Figure 2). Caregiver-patient relationships were children of the patients (n = 53, 35.3%), spouses (n = 39, 26.0%), and siblings (n = 20, 13.3%; Figure 2).
Primary caregiver characteristics
Age comparisons between patients and caregivers
Age differences were mainly identified in the 26-35 and 56-65 age groups. The majority of caregivers were in the productive age range of 26-65 years (Figure 3).
Age groupings of patients and caregivers
Health conditions of caregivers and patients
Eighty (52.7%) caregivers reported having at least one health condition, and six (7.5%) reported having four (Figure 4).
Selected health conditions (caregivers) and comorbidities (patients undergoing dialysis)
Patients were taken to receive dialysis between one (n = 4, 2.7%) and four (n = 30, 20.0%) times weekly (Figure 5).
Days to dialysis centers weekly
Dialysis sessions, travel time, and time with patient/exhaustion and sickness
Reported travel times from patients’ homes to dialysis centers ranged from as little as 45 minutes (n = 30, 20.0%) to three hours (n = 3, 2.0%). Some caregivers answered that they "drop the patients off and leave" (n = 58, 38.9%), others remain "sometimes" (n = 55, 36.7%), and about one-fifth of caregivers remain with the patient "always" (n = 29, 19.5%).
Caregivers reported "getting sick easily" (n = 61, 40.6%) after they became a caregiver and experiencing burnout or exhaustion from stress (n = 101, 67.3%). Some claimed to have had cause to visit a doctor for a health check since being caregivers (n = 32, 21.3%), whereas others reported an increase in alcohol consumption (n = 36, 24.0%).
Social consequences of caregivers
Table 1 presents the seven items used to measure self-reported consequences with the percentage of caregivers who answered "Yes" to each item.
Lower scores indicate less adverse social consequences.
Cronbach alpha = 0.664: Interpretation: Questionable reliability
The most-reported social consequence of caregiving was "Finding it difficult to maintain a good work-life balance" (n = 106, 70.7%), which was significantly associated with the caregiver’s relationship to the patient (chi-square = 11.336; df = 6; p = 0.045). The second most common consequence was "Unable to attend many social events while taking care of patients" (n = 93, 62.0%), which was significantly associated with the caregiver's age group (chi-square = 8.333; df = 3; p = 0.039).
Economic consequences of caregivers
The most reported economic consequence of caregiving was "I wish other members of the family would help contribute financially to taking care of the patient" (n = 107, 71.3%). The least reported was "I feel that I cannot sufficiently afford to pay for food, clothes, or vacations for myself or my family, owing to caregiving for the patient" (n = 83, 55.3%). Others included "wishing other family members would contribute financially"(n = 107, 71.3%), "having to worry about finances"(n = 102, 68.0%), and* *"having had to change job or work hours" (n = 99, 66.0%).
Psychological consequences for caregivers
The possible scores for the psychological consequences of providing care ranged from zero to four. Total scores (for all 15 items) ranged from 0 (n = 7, 4.7%) to 60 (n = 3, 2.0%). The mean was 32.8 (SD = 14.36), mode 38 (n = 9), and median 36. The majority experienced "feeling nervous, anxious or on edge" (n = 115, 76.7%). Figure 6 details the six items (out of 15) with the highest percentages of caregivers answering "Often" or "Everyday." Some caregivers reported feeling "down, depressed or hopeless" (n = 49, 32.7%), while others reported having "self-harm or suicidal thoughts" (n = 10, 6.7%).
Prevalence of psychological consequences of caregiving
Caregiver's age (p = 0.006) and monthly income (p = 0.028) were the only variables significantly associated with mean stress scores (Figure 6).
Health status indicators
Almost half of caregivers (n = 66, 44.0%) rated their quality of life to be "less than good." Some caregivers responded either "Rarely" or "Not at all" when asked, "To what extent do you feel life is meaningful"(n = 99, 66%; Table 2).
The leading response to each of the four items that were meant to assess caregiver QoL is presented in Figure 7.
Self-rated QoLQoL: Quality of life
Caregivers who lived with the patient had significantly higher mean QoL scores than those who did not (p = 0.040), as defined by the components used to measure it (Figure 7).
Correlations among stress, social well-being, economic well-being, and health status indicators
All bivariate correlations among stress, social well-being, economic well-being, and health status indicators were significant (Table 3). Specifically, QoL was negatively correlated with psychological, social, and economic factors.
Table 3: Correlations among stress, social well-being, economic well-being, and health status indicatorsStatistically significant at the 5% level (p < 0.05)QoL: Quality of life**
The data also showed that stress decreased with improved financial well-being.
Discussion
The majority of caregivers were women (n = 82, 54.7%), aged between 36 and 75, with the highest representation in the 36-45 (n = 28, 18.7%), 46-55 (n = 44, 29.3%), and 56-65 (n = 31, 20.7%) age groups. Most caregivers had a tertiary-level education (n = 82, 54.7%) and were employed fulltime (n = 104, 69.3%). A similar demographic profile was observed in a study conducted by Edwards et al. [12], which discovered that most caregivers were women under 45 years old, employed, and possessed a college degree.
Regarding the relationship to the patient, 35.3% (n = 53) of caregivers were elderly children, 26.0% (n = 39) were spouses, and 13.3% (n = 20) were siblings. More than half (n = 83, 55.3%) of the caregivers lived with their patients, and 69.3% (n = 104) provided full-time care. Similarly, Kari et al. [13] discovered that 58% of caregivers were fathers, 25% were mothers, and 17% were other caregivers.
Most caregivers (n = 79, 52.7%) reported having at least one health condition. Additionally, 32 (21.5%) required medical checkups, and 36 (24.2%) reported increased alcohol consumption since becoming caregivers. These findings align with those of Ebadi et al. [5] and Llamas-Ramos et al. [14], who reported that caregiving affects physical health by impairing the quantity and quality of sleep, causing fatigue, increasing musculoskeletal disorders, and causing high levels of pain. Other studies have highlighted that female caregivers, in particular, report adverse physical and psychological health profiles, with a poorer QoL [15].
Additionally, more than 50% of the caregivers (n = 80, 53.3%) took the patient for dialysis three times per week, whereas 30 (20%) did so four times weekly. This responsibility can be demanding because travel time ranges from 45 minutes to three hours. In addition, regardless of their physical presence at the dialysis center, their caregiving responsibilities extend beyond the facility. Consequently, caregivers have reported additional problems, such as getting sick easily (n = 61, 40.6%) and burnout/exhaustion from stress (n = 101, 67.3%). Similarly, Schulz et al. [8] reported that caregivers admitted to missing personal medical appointments and developing unhealthy eating habits, particularly those from lower socio-economic backgrounds. Farzi et al. [16] also revealed that reducing the commuting rate lowered the number of caregiving hours and eased the caregiver burden.
Our study revealed major challenges to the caregivers’ social lives, with the most commonly reported being “hard to have a good work-life balance” (n = 106, 70.7%), followed by “unable to attend many social events taking care of the patient” (n = 93, 62.0%). Nkuranyabahizi et al. [17] reported similar findings, with most caregivers unable to balance their duties and activities of daily living, particularly those caring for patients with ESRD. Health Experiences Research Canada [18] also reported that caregivers felt exhausted or busy to be socially active, leading to a reduction in their friends and ultimately isolation. Other studies have reported that caregivers can be overwhelmed owing to caregiving demands (e.g., end-of-life care in ESRD) or a lack of resources [19]. Statistical analysis revealed significant pairwise differences in mean scores for four demographic variables: relationship to the patient (p = 0.005), caregiver age group (p = 0.025), main responsibility for taking patients to dialysis (p = 0.037), and caregiver’s highest level of education (p = 0.005).
The economic impact was also significant. Caregivers worry about financing (n = 102, 68.0%), cannot afford personal items (n = 83, 55.3%), and 66% (n = 99) cannot afford to send patients undergoing dialysis to a nursing home. Ninety-nine (66.0%) reported having to make changes to work hours and wished other family members would contribute financially (n = 107, 71.3%). These findings are consistent with that of the study by Abebe et al. [20], in which respondents identified the loss of financial capability and other assets, such as loss of job owing to absenteeism and incapacity to purchase essential household consumables, as economic burdens. Additionally, Ma et al. [21] attributed significant expenses primarily related to dialysis, laboratory tests, and hospitalization expenses, with drug costs accounting for 50% of the economic burden faced by patients undergoing dialysis and their families.
Burnout was prevalent (n = 101, 67.8%) and could be associated with exhaustion from the stress of having to take patients to dialysis sessions, with the majority being three times weekly (n = 83, 53.3%), as well as having full-time jobs (n = 103, 69.3%). Among psychological symptoms, feeling nervous, anxious, or on edge was most common (n = 115, 76.7%), followed by loss of personal time (n = 86, 57.3%). A significant proportion of respondents also reported feeling depressed (n = 49, 32.7%). Adejumo et al. [22] highlighted elevated anxiety (31.6% vs. 5.3%) and depression (31.6% vs. 3.5%) among caregivers compared with their counterparts. Caregivers also reported “I feel lonely as a result of taking care of the patient” (n = 24, 16.0%). Ekwall et al. [23] reported similar feelings of loneliness and social life. Our study revealed suicidal tendencies among 6.7% of caregivers. This value is within the broad range (2.7%-71%) reported by O’Dwyer et al. [24] who discovered that a significant proportion of caregivers experienced suicidal ideation. Self-reported suicidal ideation [25], which can be understated, reflects the trauma that caregivers undergo.
Global self-reported health status scores revealed that the majority of caregivers rated their QoL as “less than good” (n = 62, 41.3%). Moreover, when asked “To what extent do you feel life to be meaningful,” most responded either “Rarely” or “Not at all” (n = 99, 66.0%). This finding supports that of Sajadi et al. [4], who reported a poorer QoL among caregivers than in the general population.
Recommendations
Targeted interventions are needed to address caregiver issues in multiple domains without significantly affecting QoL. We recommend expanding supportive services for primary caregivers in public and private healthcare facilities. These programs should be tailored to address the psychosocial and economic burdens of caregivers and patients undergoing dialysis. These initiatives include implementing counseling services, support groups, and improved access to psychiatric care, alongside financial assistance such as subsidies for medical expenses, transportation support, and caregiver allowances. Furthermore, workplace policies should be adapted to provide greater flexibility. Accommodations such as adjustable schedules, telecommuting options, and unpaid leave should be encouraged to enable caregivers to effectively balance their caregiving responsibilities with their employment commitments. These measures are essential for supporting caregivers and enhancing their ability to provide quality care while maintaining their well-being.
Limitations
The sample size was relatively small, especially for subgroup analyses. The participants relied on memory, which is subjective and inaccurate. In addition, inaccuracy may have resulted from a non-caregiver completing the questionnaire on behalf of the primary caregivers. As the study utilized an online platform, participants were limited to computer-literate caregivers.
Conclusions
The results of this study showed significant socio-economic and psychological burdens faced by caregivers of patients on dialysis. More than half of caregivers (n = 80, 53.3%) took the patient for dialysis three times per week, which has led to more than 50% of caregivers having difficulty maintaining a work-life balance and attending social engagements. The majority also experienced economic hardships, worrying about finances (n = 102, 68.0%) and adjusting their work hours (n = 99, 66.0%). Depressive symptoms remained high (n = 49, 32.7%) but were significantly surpassed by feelings of anxiety (n = 115, 76.7%) and burnout (n = 102, 68.0%). More than half of the respondents reported no comorbidities; however, the majority claimed that they had been "getting sick easily" since becoming caregivers. These factors all impact the QoL. These findings underscore the need for targeted interventions to support caregivers and improve their overall QoL.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prevalence and disease burden of chronic kidney disease Renal Fibrosis: Mechanisms and Therapies Lv JC Zhang LX 315Gateway East, Singapore Springer 116510.1007/978-981-13-8871-2_131399958 · doi ↗ · pubmed ↗
- 2Understanding the burden of kidney failure in Trinidad and Tobago: a review of the epidemiological data from a regional center Cureus Ramrattan A Mohammed EP Bodkin D 015202310.7759/cureus.40663 PMC 1028174037347076 · doi ↗ · pubmed ↗
- 3US Renal Data System 2020 annual data report: epidemiology of kidney disease in the United States Am J Kidney Dis Johansen KL Chertow GM Foley RN 0877202110.1053/j.ajkd.2021.01.002PMC 814898833752804 · doi ↗ · pubmed ↗
- 4Quality of life among family caregivers of patients on hemodialysis and its relevant factors: a systematic review Int J Community Based Nurs Midwifery Sajadi SA Ebadi A Moradian ST 20621852017 https://pmc.ncbi.nlm.nih.gov/articles/PMC 5478741/28670583 PMC 5478741 · pubmed ↗
- 5Psychological consequences for family caregivers of patients receiving hemodialysis: threat or opportunity?BMC Psychol Ebadi A Sajadi SA Moradian ST Akbari R 154920213462024110.1186/s 40359-021-00667-7PMC 8496675 · doi ↗ · pubmed ↗
- 6Anxiety-depression of dialysis patients and their caregivers Medicina (Kaunas) Gerogianni G Polikandrioti M Babatsikou F 1685520193113756310.3390/medicina 55050168 PMC 6572629 · doi ↗ · pubmed ↗
- 7The effects of psychosocial and economic factors on the quality of life of patients with end-stage renal disease and their caregivers in Klang Valley, Malaysia: protocol for a mixed-methods study BMJ Open Ibrahim N Chu SY Siau CS Amit N Ismail R Abdul Gafor AH 012202210.1136/bmjopen-2021-059305 PMC 917125736691236 · doi ↗ · pubmed ↗
- 8Physical and mental health effects of family caregiving Am J Nurs Schulz R Sherwood PR 2327108200810.1097/01.NAJ.0000336406.45248.4c PMC 279152318797217 · doi ↗ · pubmed ↗