Neurosurgical management for chronic and end‐of‐life pain in children: A systematic review
Sunny Abdelmageed, Nicole Villalba, Gloria Bae, James M. Mossner, Siegfried J. Adelhoefer, Kannan Aravagiri, Ravi D. Shah, Jeffrey S. Raskin

TL;DR
This review examines the use of neurosurgical treatments for managing chronic and end-of-life pain in children, highlighting their safety and potential efficacy.
Contribution
The paper provides updated recommendations for incorporating neurosurgical procedures into pediatric pain management guidelines.
Findings
Neurostimulation was effective for neuropathic pain in 58% of cases.
Ablative procedures showed better results for nociceptive pain.
Intrathecal pumps and chordotomy provided relief for mixed pain conditions.
Abstract
Chronic and end‐of‐life pain in children is underreported and undermanaged. Current guidelines for pediatric chronic pain include medical and interventional modalities; however, the inclusion of neurosurgical treatments is uncommon and inconsistent. This systematic review presents the literature, and we provide recommendations for the role of neurosurgical procedures in treating chronic and end‐of‐life pain in children. A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta‐analyses (PRISMA) guidelines using three databases: PubMed, Embase, and Scopus. We included 40 studies presenting neurosurgical procedures for the treatment of chronic and end‐of‐life pain in children. Thirty‐one (77.5%) manuscripts focused on the treatment of neuropathic pain, five (12.5%) focused on nociceptive pain, and four (10%) treated mixed pain…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
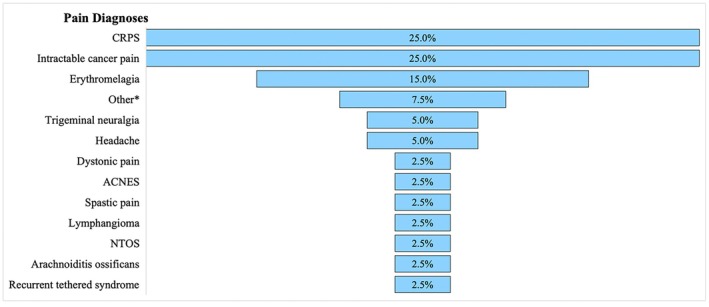 FIGURE 1
FIGURE 1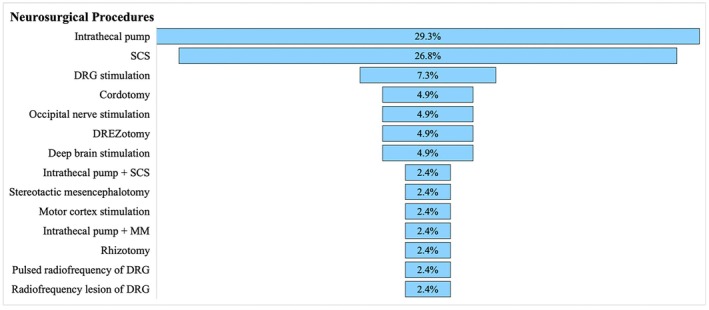 FIGURE 2
FIGURE 2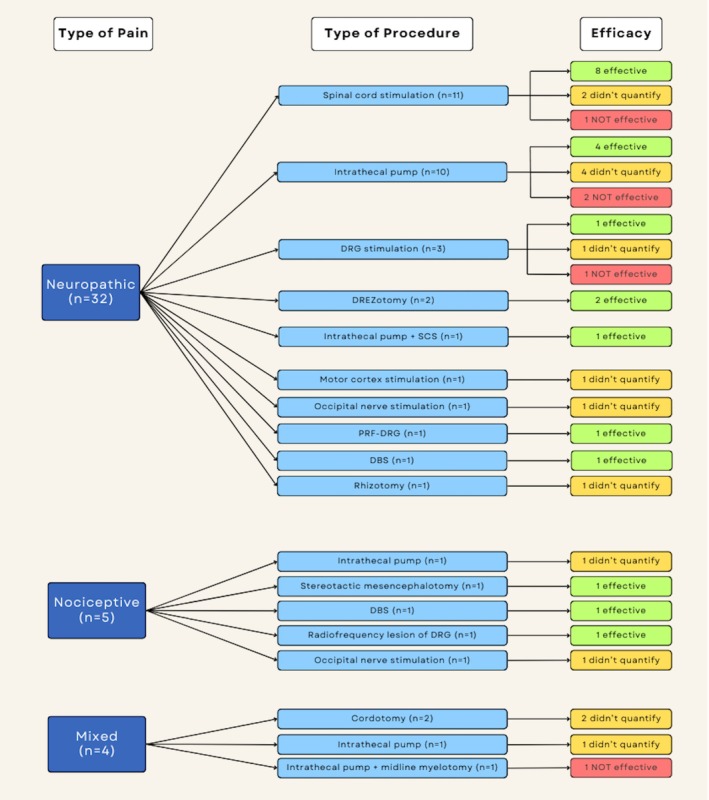 FIGURE 3
FIGURE 3| Study | Country | Study design ( | Follow‐up period | Pain diagnosis | Procedure | Pain outcomes | Complications | Time to surgery decision | Quality/risk of bias |
|---|---|---|---|---|---|---|---|---|---|
| Reddy et al | USA | Case report (1) | 10 days | Intractable cancer pain | Percutaneous cordotomy | Pain relief, functional status | None | Unspecified | E/Serious |
| Steel et al | UK | Case report (2) | 12 weeks, 36 months | Intractable cancer pain | Open thoracic anterolateral cordotomy | Pain relief, functional status, medication use | None | 2 months | E/Serious |
| Kanpolat et al | Turkey | Case report (1) | 60 months | CRPS‐I | DREZotomy | VAS score, functional status | Transient ipsilateral lower extremity ataxia (2 months) | 19 months | E/Serious |
| Iglesias et al., 2022 | Argentina | Case series (3) | Unspecified, 4 months, unspecified | Intractable cancer pain | Lumbosacral DREZotomy | VAS score, quality of life | None | Unspecified, 4 months, 19 months | E/Serious |
| D'Angelo et al | USA | Case report (1) | 1 year | Erythromelalgia | Intrathecal pump | Pain relief | None | 2 weeks | E/Serious |
| Collins et al | USA | Retrospective study (11) | Unspecified | Intractable cancer pain | Intrathecal pump | Pain relief | Catheter occlusion by tumor causing tachyphylaxis | 2 weeks‐6 months | B/Moderate |
| Galloway et al | USA | Case report (1) | 5 months | Intractable cancer pain | Intrathecal pump | VAS score, functional status, quality of life | None | Unspecified | E/Serious |
| Aram et al | USA | Retrospective study (25) | 4–240 days | Intractable cancer pain, abdominal surgery, trauma | Intrathecal pump | Pain relief, medication use | Cellulitis at catheter exit site, accidental dislodgement | Unspecified | B/Serious |
| Stanton‐Hicks & Kapural | USA | Case report (1) | 9 months | CRPS‐I | Intrathecal pump | VAS score, functional status | None | 2 months | E/Serious |
| Farid & Heiner | USA | Case report (1) | 2 months | CRPS | Intrathecal pump | Pain relief, functional status | None | 7 weeks | E/Serious |
| Kajiume et al | Japan | Case report (1) | 109 days | Intractable cancer pain | Intrathecal pump | Pain relief, quality of life | None | 57 days | E/Serious |
| Moens et al | Belgium | Case report (1) | 3 months | Pain due to arachnoiditis ossificans | Intrathecal pump | Pain relief | Transient loss of appetite, metallic taste | Unspecified | E/Serious |
| Bengali et al | USA | Case report (1) | 5 months | Intractable cancer Pain | Intrathecal pump | Pain relief, quality of life | None | Unspecified | E/Serious |
| Abolhasan Gharehdaghi et al | Iran | Randomized clinical trial (88) | 14 days | Intractable cancer pain | Intrathecal pump | VRS score, VAS score, DN4 score | Nausea, vomiting | Unspecified | A/Moderate |
| Tubic | USA | Case report (1) | 12 weeks | CRPS‐I | Intrathecal pump | NRS score, functional status | Transient itching on stomach, nausea, stomach irritation | 2 months | E/Serious |
| Bentley et al | USA | Case report (1) | 3 months | Intractable cancer pain | Intrathecal pump + midline myelotomy | VAS score | None | Unspecified | E/Serious |
| Rodriguez‐Lopez et al | Spain | Case series (6) | Unspecified | CRPS | Intrathecal pump + spinal cord stimulation | VAS score, functional status, medication use, pain relief | None | 5 weeks | E/Serious |
| Kim et al | USA | Case series (14) | 22 months +/− 18 months | Intractable pain | Intrathecal pump, spinal cord stimulation | VNS score, functional status, medication use | Seroma, post‐dural puncture headache, pump erosion through skin, vomiting | 6–58 months | E/Serious |
| Ivanishvili et al | UK | Case report (1) | 5 months | Intractable cancer pain | Stereotactic mesencephalotomy | VAS score, medication use | None | 6 months | E/Serious |
| Kato et al | Japan | Case report (1) | 3 months | Trigeminal neuralgia | Rhizotomy | Pain relief | Transient Mild sensory disturbance (tinnitus, hearing loss, left nystagmus) | 8 months | E/Serious |
| Perides et al | UK | Retrospective study (63) | 12.4 months +/1.2 months | Dystonic pain | Deep brain stimulation | NRS score, PPP, medication use | None | Unspecified | B/Serious |
| Mol & Roumen | Netherlands | Case report (1) | 12 months | Anterior cutaneous nerve entrapment syndrome | Dorsal root ganglion stimulation | NRS score | Severe pain at battery site improved with relocation | Unspecified | E/Serious |
| Pinckard‐Dover et al | USA | Case report (1) | 30 months | CRPS‐I | Dorsal root ganglion stimulation | Pain relief, functional status | None | 2 years | E/Serious |
| Graca et al | USA | Case series (5) | 3–48 months | CRPS‐I | Dorsal root ganglion stimulation | NRS score, functional status | None | 1–5 years | E/Serious |
| Vles et al | Netherlands | Prospective study (17) | 6–9 months | Spastic pain | Radiofrequency lesion of dorsal root ganglia | VAS score | Transient increase in pain | Unspecified | B/Moderate |
| Apiliogullari et al | Turkey | Case report (1) | 6 months | CRPS‐I | Pulsed radiofrequency to dorsal root ganglia | VAS score | None | 1 month | E/Serious |
| Delavallee et al | Belgium | Case report (1) | 15 months | Trigeminal neuralgia | Motor cortex stimulation | Pain relief, medication use | Superficial wound infection | Unspecified | E/Serious |
| Stubberud et al | Norway | Case report (1) | 3 years | Headache | Occipital nerve stimulation | Pain relief | None | 5 years | E/Serious |
| Borius & Valade | France | Case report (1) | 12 months | Headache | Occipital nerve stimulation | Pain relief, quality of life | None | 6 months | E/Serious |
| Olsson et al | Sweden | Retrospective case study (7) | 1–3 years | CRPS‐I | Spinal cord stimulation | Pain relief, functional status | Subcutaneous infection | Unspecified | B/Serious |
| Patel et al | USA | Case report (1) | 2 years | Erythromelalgia | Spinal cord stimulation | NRS score, functional status | None | Unspecified | E/Serious |
| Dones et al | Italy | Case report (1) | 1 year | Lymphangioma | Spinal cord stimulation | VAS score, functional status | None | 4 years | E/Serious |
| Tyagi et al | USA | Case report (1) | 10 months | Recurrent tethered cord syndrome | Spinal cord stimulation | VAS score, functional status | None | Unspecified | E/Serious |
| Fan et al | China | Case report (1) | 12 months | Erythromelalgia | Spinal cord stimulation | VAS score, medication use | None | Unspecified | E/Serious |
| Hale & Cheng | USA | Case report (1) | 3 years | Neurogenic thoracic outlet syndrome | Spinal cord stimulation | Pain relief, functional status, medication use | None | 1 year | E/Serious |
| Bakr et al | USA | Case series (12) | 12 months | CRPS, spinal cord injury, hyperpathia, lumbago, urogenic pain, neuralgia | Spinal cord stimulation | VAS score, medication use, functional status | Transient intraoperative CSF leak | 1–6 years | E/Serious |
| Schatmeyer et al | USA | Case report (1) | 6 months | CRPS | Spinal cord stimulation | Pain relief, quality of life | None | Unspecified | E/Serious |
| Toriya et al | Russia | Case report (1) | 6 months | Erythromelalgia | Spinal cord stimulation | VAS score, functional status | None | Unspecified | E/Serious |
| Zuo et al | China | Case report (1) | 2 months | Erythromelalgia | Spinal cord stimulation | VAS score, functional status, medication use | None | 1 year | E/Serious |
| Delye et al | Belgium | Case report (1) | 7 weeks | Erythromelalgia | Deep brain stimulation | Pain relief, medication use | None | Unspecified | E/Serious |
| Neuropathic pain ( | Nociceptive pain ( | Mixed pain ( |
|---|---|---|
| CRPS ( | Arachnoiditis ossificans ( | Intractable cancer pain ( |
| Intractable cancer pain ( | Intractable cancer pain ( | Other |
| Erythromelalgia ( | Dystonic pain ( | |
| Trigeminal neuralgia ( | Spastic pain ( | |
| Other | Headache ( | |
| Anterior cutaneous nerve entrapment syndrome ( | ||
| Headache ( | ||
| Lymphangioma ( | ||
| Neurogenic thoracic outlet syndrome ( | ||
| Recurrent tethered cord syndrome ( |
| Pain outcome |
|
|---|---|
| Visual Analogue Scale (VAS) | 16 (40.0%) |
| Numeric Rating Scale (NRS) | 5 (12.5%) |
| Verbal Rating Scale (VRS) | 1 (2.5%) |
| Verbal Numeric Scale (VNS) | 1 (2.5%) |
| Douleur Neuropathique 4 (DN4) | 1 (2.5%) |
| Karnofsky Performance Scale | 2 (5.0%) |
| Pain relief | 19 (47.5%) |
| Functional status (mobility, activity, strength) | 19 (47.5%) |
| Quality of life | 6 (15.0%) |
| Pain medication use | 12 (30.0%) |
| Mood (depression, anxiety) | 4 (10.0%) |
| Intrathecal pump | |||||
|---|---|---|---|---|---|
| Neuropathic pain | |||||
| Study | Procedure | Assessment | Preoperative Pain Score | Postoperative Pain Score | Effective? |
| Galloway et al | Intrathecal pump | VAS | 8 | 0–3 | Yes |
| Stanton‐Hicks & Kapural | Intrathecal pump | VAS | 5 | 4 | No |
| Farid & Heiner | Intrathecal pump | NRS | 10 | 0–2 | Yes |
| Abolhasan Gharehdaghi et al | Intrathecal pump | VAS | 7 +/−0.25 | 1 +/−0.12 | Yes |
| Kim et al | Intrathecal pump | VNS | 7.9 | 5.9 | No |
| Tubic | Intrathecal pump | NRS | 8 | 0 | Yes |
| Ablative techniques | |||||
| Neuropathic pain | |||||
| Kanpolat et al | DREZotomy | VAS | 9 | 0 | Yes |
| Iglesias et al., 2022 | Lumbosacral DREZotomy | VAS | 10 | 0.67 | Yes |
| Apiliogullari et al | Pulsed radiofrequency to dorsal root ganglion | VAS | 100 | 0 | Yes |
| Nociceptive pain | |||||
| Vles et al | Radiofrequency lesion of dorsal root ganglion | VAS | 8.39 | 4.17 | Yes |
| Ivanishvili et al | Stereotactic mesencephalotomy | VAS | 10 | 0 | Yes |
| Neuromodulation | |||||
| Neuropathic pain | |||||
| Patel et al | Spinal cord stimulation | NRS | 10 | 0 | Yes |
| Dones et al | Spinal cord stimulation | VAS | 9 | 1 | Yes |
| Tyagi et al | Spinal cord stimulation | VAS | 8 | 1 | Yes |
| Kim et al | Spinal cord stimulation | VNS | 7.5 | 3.8 | No |
| Fan et al | Spinal cord stimulation | VAS | 8 | 0 | Yes |
| Hale & Cheng | Spinal cord stimulation | NRS | 6 | 0–2 | Yes |
| Bakr et al | Spinal cord stimulation | VAS | 9.2 | 2.9 | Yes |
| Toriya et al | Spinal cord stimulation | VAS | 8 | 2–4 | Yes |
| Zuo et al | Spinal cord stimulation | VAS | 6 | 2–3 | Yes |
| Mol & Roumen | Dorsal root ganglion stimulation | NRS | 8 | 3 | Yes |
| Graca et al | Dorsal root ganglion stimulation | NRS | 9.4 | 5.2 | No |
| Nociceptive pain | |||||
| Perides et al | Deep brain stimulation | NRS | 7.3 | 2.3 | Yes, |
| Mixed procedures | |||||
| Neuropathic pain | |||||
| Rodriguez‐Lopez et al | Intrathecal pump + spinal cord stimulation | VAS | 7.7 | 0.3 | Yes |
| Mixed pain | |||||
| Bentley et al | Intrathecal pump + midline myelotomy | VAS | 9 | 7 | No |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Pain Management Techniques · Anesthesia and Pain Management · Pain Mechanisms and Treatments
INTRODUCTION
Chronic pain, defined as persistent or recurring pain lasting longer than 3 months, has high morbidity and long‐lasting quality of life impact.1 In pediatric populations, chronic pain of any type is estimated to impact between 11% and 38% of individuals, with approximately 5% of those with chronic pain experiencing significant impacts in daily functioning.2 Chronic pain has noticeable impacts on a child's future development and can lead to education delays or long‐lasting psychological harm.2, 3
Pediatric chronic pain requires interdisciplinary pain management by a team of healthcare professionals from various disciplines. Treatment approaches include physical therapy, occupational therapy, psychological support, and medication.4 Initially, conservative medical management focuses on nonopioid medications, often evolving to opioid therapies of increasing strength. When these conservative measures fail, interventional procedures are often introduced. Common regional and neuraxial injections are considerably less invasive than neurosurgical procedures.5, 6 These techniques demonstrate a safety and efficacy profile for pediatric chronic pain similar to those in adults.7 However, neurosurgical interventions in the pediatric population are less well studied and are not currently included in chronic or end‐of‐life pain management guidelines.8
The neurosurgical treatment of pain can be categorized into three groups: neurostimulation, ablative techniques, and targeted drug delivery through intrathecal pumps.5 These neurosurgical modalities have been shown to vary in efficacy for different types of pain. Understanding the fundamental primary pain generators for chronic and end‐of‐life pain is essential to optimize neurosurgical therapy. Pain is often defined by its pathophysiology, and common types include nociceptive (ie, originating from nociceptors in the musculoskeletal system), neuropathic (ie, originating from the central nervous system), and mixed. Nociplastic pain is an alteration of perception pain syndrome (eg, fibromyalgia) and is not covered in this review.9
Comprehensive reviews of the neurosurgical treatment of pain in adults stipulate indications and outcomes across procedures and pain syndromes; however, this is entirely lacking for children.5 We systematically review the existing literature regarding the neurosurgical treatment of chronic and end‐of‐life pain in pediatric populations and provide recommendations for neurosurgical procedures in practice.
METHODS
Study selection
A systematic review was conducted in accordance with the Preferred Reviews and Meta‐analyses (PRISMA) 2020 guidelines to determine the role of neurosurgical procedures in the treatment of chronic pain in pediatric patients.10 Keywords associated with chronic pain, pediatric patients, and neurosurgical procedures were searched on November 27, 2023, through PubMed MEDLINE (National Library of Medicine), Embase (Elsevier), and Scopus (Elsevier). A full list of search terms is listed in Table S1. No date, language, or article type restrictions were applied. This protocol was prospectively registered on PROSPERO.11
All publications from the initial search were imported into EndNote (Clarivate Analytics, Philadelphia, PA), and duplicates were excluded. The deduplicated articles were screened for relevance by title and abstract by two authors (SA and GB). Articles progressing to full‐text review were screened for final inclusion according to the following predetermined inclusion criteria: (1) published in or translated into the English language, (2) available full text, (3) pediatric population (<25 years of age) with chronic pain, (4) neurosurgical therapy for the primary purpose of pain control, and (5) provided outcomes of neurosurgical procedures. The outcomes of treatment included complication rates and efficacy determined by improvement in pain scales. Articles were screened independently by two reviewers (SA and GB) through Rayyan (https://rayyan.qcri.org/). All disagreements were discussed and resolved by the reviewers.
Data extraction
Data from included studies were extracted independently and cross‐checked for accuracy by authors (SA and GB). Article information including bibliographic data, study design, number of patients, condition, type of pain, procedure, and outcomes—efficacy and complications—were reviewed.
Type of pain
Studies were grouped into three categories based on the type of pain (neuropathic, nociceptive, or mixed). The type of pain was determined in the following tiered system: (1) reported within the study manuscript, (2) pain condition with known etiology, and (3) classified by authors through standard definitions of pain types. Any manuscript needing to be classified by authors was reviewed by a senior author (JSR) for accuracy.
Pain outcomes
The primary outcome was efficacy of the neurosurgical procedure to treat pain. Efficacy was determined for studies that reported numerical pain scores pre‐ and postoperatively. Treatment was determined effective if there was a ≥50% reduction in the numeric pain score and ineffective if there was a <50% reduction. Studies that did not report a numeric pain score or had missing data were classified as “not quantified.” Subjective data on the effect on pain control were collected, but these data were not used to determine efficacy. Secondary outcomes included both intraoperative and postoperative complications. Descriptive analysis was performed in Excel.
Risk of bias and quality evaluation
Critical appraisal of all included studies was conducted by assessing the risk of bias using the Risk Of Bias In Non‐Randomized Studies—of Interventions (ROBINS‐I) tool and quality using the Grading of Study Design Quality framework as described in another study.12, 13 Two reviewers (SA, GB) assessed the risk of bias and quality of each study independently, and disagreements were resolved by a third reviewer (NV).
RESULTS
A total of 3492 articles were identified: 990 from PubMed, 915 from Scopus, and 1587 from Embase. 858 duplicate articles were removed, and 2634 articles were screened by title and abstract. After initial title and abstract screening, 139 full‐text articles were assessed for eligibility and 40 articles were found to be eligible (Figure S1).14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53 Study characteristics are reported in Table 1. The study periods ranged from 1992 to 2023. The majority of studies were case reports (72.5%) followed by case series (12.5%), retrospective cohorts (10%), prospective cohorts (2.5%), and randomized clinical trials (2.5%). The number of patients in each study ranged from 1 to 88. In total, there were 281 pediatric participants with chronic pain who received neurosurgical treatment. The overall risk of bias in this study was serious, and the overall quality of evidence was low due to the prevalence of case reports and lack of randomized control trials included.
Pain diagnoses and neurosurgical procedures
Of the 40 studies, 31 (77.5%) reported a neuropathic type of pain,16, 17, 18, 19, 20, 22, 23, 24, 26, 27, 28, 30, 31, 33, 35, 36, 37, 39, 40, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53 5 (12.5%) reported a nociceptive pain,25, 32, 34, 38, 41 and 4 (10%) reported a mixed pain (Table 2).14, 15, 21, 29 The most common diagnoses were intractable cancer pain and complex regional pain syndrome (CRPS). Both diagnoses were found in 10 (25%) articles each (Figure 1).14, 15, 16, 17, 19, 20, 22, 23, 24, 26, 27, 28, 29, 30, 32, 36, 37, 39, 43, 50 Of the 41 neurosurgical procedures for pain reported in all studies, the intrathecal pump was the most commonly used (29.3%),18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 31 followed by spinal cord stimulation (SCS) (26.8%),31, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52 dorsal root ganglion (DRG) stimulation (7.3%),35, 36, 37 cite cordotomy (4.9%),14, 15 occipital nerve stimulation (ONS) (4.9%),41, 42 lesioning of the dorsal root entry zone (DREZotomy) (4.9%),16, 17 deep brain stimulation (DBS) (4.9%),34, 53 and other procedures (intrathecal pump + SCS, mesencephalotomy, motor cortex stimulation (MCS), intrathecal pump + midline myelotomy, rhizotomy, pulsed radiofrequency of DRG, and radiofrequency lesion of DRG) each at 2.4% (Figure 2).29, 30, 32, 33, 38, 39, 40
*Funnel plot of pain diagnoses reported in the included studies, from most commonly (top) to least commonly (bottom) reported. ACNES, anterior cutaneous nerve entrapment syndrome; CRPS, chronic regional pain syndrome; NTOS, neurogenic thoracic outlet syndrome. other includes studies (Aram 2001, Bakr 2022, and Kim 2018) including patients with multiple etiologies of chronic pain these include cancer/metastatic disease, hematologic conditions, severe trauma causing lasting injury, chronic low back pain, spinal cord injury, musculoskeletal conditions, cerebral palsy.
Funnel plot of neurosurgical procedures for pain reported in the included studies, from most commonly (top) to least commonly (bottom) reported. DREZ, dorsal root entry zone; DRG, dorsal root ganglion; MM, midline myelotomy.
Pain outcomes
Reported pain outcomes across studies were heterogeneous, with both qualitative and quantitative measures used (Table 3). The most common methods for reporting pain outcomes were qualitative measures, including pain relief (47.5%) and functional status (47.5%). Six quantitative assessments were used, with the Visual Analogue Scale (VAS) being the most frequent (40.0%), followed by the Numeric Rating Scale (NRS) (12.5%), the Karnofsky Performance Scale (5.0%), the Verbal Rating Scale (VRS) (2.5%), the Verbal Numeric Scale (VNS) (2.5%), and Douleur Neuropathique (DN4) (2.5%).
The efficacy of neurosurgical pain treatments is reported in Figure 3. Neuropathic pain was treated with 32 procedures across 31 studies. SCS was the most common neurosurgical procedure reported in 35.5% (11/31) of studies.31, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52 Of these studies, 8 reported effective treatment while 1 did not report improved results (Table 4).31, 44, 45, 46, 47, 48, 49, 51, 52 The remaining 2 studies reported significant improvement in pain relief and quality of life but did not provide numeric scores for a measurable outcome.43, 50 Other forms of treatment for neuropathic pain that were determined to be effective included intrathecal pump (n = 4),20, 23, 27, 28 DREZotomy (n = 2),16, 17 DRG stimulation (n = 1),35 intrathecal pump + SCS (n = 1),30 DBS (n = 1),53 and pulsed radiofrequency of DRG (n = 1) (Table 4).39 There were 10 studies that did not provide numeric pain scores but reported overall improvement in quality of life and pain relief after treatment of neuropathic pain, including intrathecal pump (n = 4),18, 19, 24, 26 SCS (n = 2),43, 50 DRG stimulation (n = 1),36 MCS (n = 1),40 ONS (n = 1),42 and rhizotomy (n = 1).33 There were 4 studies that reported ineffective treatment of chronic neuropathic pain, including intrathecal pump (n = 2),22, 31 SCS (n = 1),31 and DRG stimulation (n = 1) (Table 4).37
Efficacy of neurosurgical procedures reported in the included studies. The first column (dark blue, left) indicates the type of pain (neuropathic, nociceptive, or mixed) and the number of neurosurgical procedures by study employed. The middle column (light blue, middle) reports the type of procedure. The last column (right) reports the efficacy, with effective indicated in green, not quantified in yellow, and not effective in red. Efficacy was determined using only quantitative measures of pain control, defining effectiveness as a ≥50% reduction in the numeric pain score. DBS = deep brain stimulation; DREZ, dorsal root entry zone; PRF, pulsed radiofrequency; SCS, spinal cord stimulation.
Nociceptive pain was treated with 5 different neurosurgical procedures across 5 studies.25, 32, 34, 38, 41 Two studies, one using an intrathecal opioid pump and the other using ONS, reported subjective pain relief but did not provide numeric pain scores.25, 41 The remaining 3 studies provided pain scores and were determined to be effective in their treatment of chronic pain with stereotactic mesencephalotomy, DBS, and radiofrequency lesion of the DRG (Table 4).32, 34, 38
Lastly, in the treatment of mixed pain, 2 studies reporting on cordotomy and 1 study using an intrathecal opioid pump reported subjective pain relief but did not quantify pain using a numeric score.14, 15, 21 In one study, combination therapy with an intrathecal opioid pump and midline myelotomy was determined to be not effective in the treatment of chronic pain (Table 4).29
Complications
Overall, complications were minimal; see Table 1. The most common complication of ablative techniques was sensory complications. Difficulty with the pump or catheter system or medication side effects was the most common complication of intrathecal pumps. Infection was the most common complication of neurostimulation.
DISCUSSION
Chronic pain is undertreated and underreported in pediatric populations.3 Chronic pain reduces quality of life and can affect the developmental trajectory in children.2, 3 Treatment protocols for chronic pain typically evolve from non‐interventional medication regimens and physical therapy to regional and neuraxial injections and finally to neurosurgical procedures. Studying pain sensation in children can differ from that in adults, and this suggests that chronic pain in children should be addressed with even more vigor.54 Neurosurgical pain procedures in children are less widely applied with limited literature and absent guidelines. Contributors to a lack of evidence and application of neurosurgical pain procedures in children include ethical considerations, a lack of FDA‐approved indications, adult hardware, and limited infrastructure in institutions dedicated to treating children. There is also a lack of reliable, standardized assessments of pre‐ and postoperative pain in children. A recent review discussing interventional procedures for chronic pain in children provides a comprehensive overview of regional, and neuraxial techniques yet exclude neurosurgical therapies apart from one case report of SCS.7 To our knowledge, this is the first comprehensive review of neurosurgical treatments for chronic pain in children.
Pain can be classified into three main categories: neuropathic, nociceptive, and mixed.55 The quality and the region of the pain syndrome define the treatment. CRPS, intractable cancer pain, erythromelalgia, and trigeminal neuralgia predominantly exhibit neuropathic characteristics.56 Nociceptive pain is more commonly associated with conditions like dystonic pain and spastic pain.5 This differentiation aids in tailoring interventions to the specific pain mechanisms underlying each condition, improving treatment outcomes.
Neurostimulation reduces pain by interfering with the transmission of pain through tactile or electrical stimulation.5 Examples of neurostimulators include SCS, peripheral nerve stimulation (PNS), MCS, DBS, and ONS. In adults, SCS and PNS are recognized as effective management options for chronic pain.57 Intracranial stimulation, such as MCS, DBS, or ONS, may be pursued when less invasive methods have proven ineffective. MCS holds promise in treating central pain syndromes such as thalamic pain syndrome, while DBS may be employed for various nociceptive and neuropathic pain states.58
Originally, we intended to explore the use of neurosurgical procedures for chronic and end‐of‐life pain in children and create standardized treatment guidelines, similar to those developed in adults. However, the use of heterogeneous non‐standardized pain measures made it difficult to compare the efficacy of neurosurgical procedures across studies. Therefore, we determined efficacy using only quantitative measures of pain control, defining effectiveness as a ≥50% reduction in the numeric pain score. Here, we present a focused review describing the available evidence of the neurosurgical treatment of chronic pain for children, as a first step towards standardized pain guidelines.
Neuropathic pain
Neuropathic pain, characterized by hyperalgesia, allodynia, and paresthesia, originates as a result of damage or dysfunction of the central or peripheral nervous system.56 Neuropathic pain typically responds well to neurostimulation.56 Overall, 58% of the papers treating neuropathic pain utilized neurostimulation, with the majority reporting good efficacy.30, 31, 35, 36, 37, 40, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53 Only one study reported non‐efficacy utilizing neurostimulation.37 Graca and colleagues utilized DRG stimulation for CRPS‐I, reporting efficacy in 60% of patients (3/5) with a reduction in NRS score ranging from 50% to 100%, while the other two patients had no response at all.37 One additional case report utilized DRG stimulation for CRPS‐I and reported a 100% reduction in pain.36 SCS was most commonly employed (35.5%) with all but 1 manuscript reporting efficacy.31, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52 DRG stimulation was rarer (9.7%) and may require further research to determine optimal patient selection.35, 36, 37 ONS and MCS were each used in only one case report, which reported subjective improvement in pain but did not quantify the effect.40, 42
Neurostimulation should be considered for the treatment of chronic pediatric pain of neuropathic origin. This treatment option is particularly appealing in these patients due to its reversibility and absence of permanent damage. Ablative techniques may precipitate neuropathic pain and therefore may not represent an optimal treatment.5 However, our study found that 12.9% of manuscripts treating neuropathic pain utilized ablative techniques and noted objective or subjective improvement.16, 17, 33, 39 Sensory complications were noted following these procedures in 40% of patients with resolution over 3 months. Appropriate ablative techniques can be considered for neuropathic pediatric pain, although the higher risk of neuropathic pain or lack of efficacy should be considered and may not be suitable for candidates with a long‐life expectancy.59
Intrathecal pumps were used in 32.3% of papers for neuropathic pain, with variable efficacy.18, 19, 20, 22, 23, 24, 26, 27, 28, 31 Two papers reported non‐efficacy.22, 31 Complications such as device difficulties (eg, pump size, catheter blocking, catheter dislodgement), medication effects (eg, nausea, vomiting, sedation, respiratory depression, gastrointestinal issues), and surgical complications (eg, wound healing, post‐dural puncture headache) were reported.22, 31 Intrathecal pumps can be used to improve drug delivery and were most utilized for cancer pain.
Nociceptive pain
Nociceptive pain occurs in response to transduction by activated nociceptors and continues via transmission along pain tracts, modulation within the CNS, and is ultimately perceived. Nociceptors, classified by their response profiles, can be activated by mechanical, thermal, and chemical stimuli.
Neurostimulation was used in 40% of manuscripts (2/5) to treat nociceptive pain, one using DBS demonstrated efficacy, while the other using ONS worsened the pain until the device was explanted.34, 41 More research is needed to determine if neurostimulation is an effective treatment for nociceptive pediatric pain.
Ablative therapy was used in 40% of papers (2/5) to treat nociceptive pain; both demonstrated efficacy.32, 38 Stereotactic mesencephalotomy was used for refractory head and neck pain secondary to a cervical cord glioblastoma and demonstrated a reduction in VAS score from 10 to 0.32 In adults, intractable cancer pain of the head and neck is a primary indication for stereotactic mesencephalotomy; application in children is extremely uncommon. In this case, the patient was able to remain pain‐free and leave the hospital for 5 months following this procedure.32 DRG radiofrequency ablation was used for the treatment of spastic pain in 17 children with cerebral palsy with a reduction in average VAS score from 8.39 to 4.17.38 Although many papers using rhizotomy were identified for the treatment of hypertonia, demonstrating a significant reduction in nociceptive pain, they were not included in this study because their primary purpose was for muscle tone control.60, 61, 62 Ablative procedures are effective for nociceptive pain control in pediatric patients and should be considered for medically refractory cases.
An intrathecal bupivacaine pump was used in one case series for the treatment of rapidly progressive pain due to arachnoiditis ossificans secondary to chemotherapy.25 The patient experienced a metallic taste and loss of appetite, which resolved over time. Intrathecal pumps can be used in nociceptive pain, though side effects may occur.
Mixed pain
Mixed pain is the result of overlapping primary pain generators and includes nociceptive and neuropathic characteristics. This chronic pain was the least commonly reported (10% of manuscripts).14, 15, 21, 29 Neurostimulation was not reported for the treatment of mixed pain. Two papers reported the use of cordotomy both for intractable cancer pain and reported immediate and significant improvement in their pain.14, 15 Malignant pain with a life expectancy of <2 years is the primary indication for cordotomy in adults.5 One paper used intrathecal pumps in 25 children for various indications including end‐stage malignancy, extensive abdominal surgery, and trauma, noting a substantial reduction in pain and elimination or reduction of the need for supplemental opioids.21 Finally, one paper reported the use of midline myelotomy and an intrathecal pump for the treatment of intractable cancer pain.29 They reported pain relief from the midline myelotomy for 2 months and then, unfortunately, a complete return of their pain and only a moderate reduction in pain following intrathecal pump insertion (VAS score 9–7).
Mixed pain is complex, and reports of treatment in pediatric patients are extremely rare. Both intrathecal pumps and ablative techniques demonstrate subjective efficacy; however, combining therapeutic modalities did not appear to increase efficacy. A combination of neurostimulation with ablative or intrathecal pumps may provide relief in refractory patients. More research is required to discern optimal treatment strategies.
Considerations
It is important to acknowledge differing viewpoints within the pediatric chronic pain community regarding the use of interventional procedures. Some experts argue that these should be a last resort after all other conservative measures have been exhausted due to concerns about the potential risks and long‐term impacts on a child. Our findings suggest that neurosurgical interventions may offer significant relief in cases where chronic pain severely impacts the child's quality of life. The decision to proceed with any neurosurgical intervention should take into account the individual needs of the patient and involve interdisciplinary discussions with both the patient and their family. The timing to proceed with neurosurgical intervention varied significantly, ranging from 2 weeks to 5 years (see Table 1). Intrathecal pain pumps were typically the quickest intervention, with time to decision in as little as 2 weeks following presentation. By contrast, ablative and neuromodulatory techniques took longer (4 months‐5 years), perhaps due to the perceived invasiveness of these techniques. Several factors contributed to these delays, most notably the desire to exhaust all non‐interventional pain management strategies due to safety concerns and the desire to avoid procedural intervention. Additional delays were caused by patient‐specific factors, such as neutropenia or thrombocytopenia, which required medical stabilization before neurosurgical intervention could proceed. In some cases, lengthy delays were due to limited access to interventional specialists and extended referral times. Neurosurgical intervention should be integrated in discussions of pain management early in the treatment process. Many patients experienced significant pain resolution shortly after intervention, suggesting that earlier and improved access to neurosurgical procedures could lead to faster pain control, improved outcomes, and reduced psychiatric complications associated with prolonged pain.
Limitations
There are several limitations to this study. Most of the manuscripts identified were case reports, which limits generalizability. The considerable heterogeneity among included studies in terms of design, patient demographics, and outcome measures limited the ability to perform meta‐analyses and necessitated a narrative synthesis. Quality assessment revealed variability in study quality, predominantly case reports, with a lack of high‐quality randomized controlled trials. Short follow‐up periods in many studies may underestimate long‐term treatment effects. Despite efforts to minimize bias, inherent biases may exist in the included studies, potentially influencing findings. Non‐standardized measures or no numerical measures of pain control limit the ability to compare efficacy across studies. While providing valuable insights, future research should address these limitations to better inform clinical practice regarding neurosurgical interventions for pediatric chronic pain management.
CONCLUSIONS
Neurosurgical treatments are safe for chronic and end‐of‐life pain syndromes in children. Broad efficacy cannot be determined due to sparse literature and inadequately quantified pain responses. Neuropathic pain appears to be best treated with neurostimulation, nociceptive pain with ablative techniques and possibly neurostimulation techniques, and mixed pain with intrathecal pumps and/or ablative techniques. Guidelines for escalating chronic and end‐of‐life pain management in pediatric patients should be updated to include neurosurgical treatments and appropriate outcome scales. Focused research on appropriate patients, available neurosurgical therapies, and pediatric outcomes is warranted.
AUTHOR CONTRIBUTIONS
SA contributed to study conception, completed data acquisition, analysis, and interpretation, and drafted the manuscript. NV completed data visualization and drafted the manuscript. GB completed data acquisition, analysis, and interpretation, and drafted the manuscript. JMM completed data analysis and revised the manuscript. SJA drafted the manuscript. KA and RDS critically revised the manuscript. JSR contributed to study conception, supervised the study, and revised the manuscript. All authors reviewed and approved the submitted manuscript.
FUNDING INFORMATION
There was no specific funding received for the completion of this manuscript.
CONFLICT OF INTEREST STATEMENT
Jeffrey S. Raskin is a paid consultant to Iota, Synergia, BlackRock Neurotech, and Medtronic. The other authors have no potential conflicts of interest to disclose.
PATIENT CONSENT STATEMENT
Not applicable.
PERMISSION TO REPRODUCE MATERIAL FROM OTHER SOURCES
Not applicable.
CLINICAL TRIAL REGISTRATION
Not applicable.
Supporting information
Data S1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smith TJ , Hillner BE . The cost of pain. JAMA Netw Open. 2019;2(4):e 191532. 10.1001/jamanetworkopen.2019.1532 30951152 · doi ↗ · pubmed ↗
- 2Tutelman PR , Langley CL , Chambers CT , Parker JA , Finley GA , Chapman D , et al. Epidemiology of chronic pain in children and adolescents: a protocol for a systematic review update. BMJ Open. 2021;11(2):e 043675. 10.1136/bmjopen-2020-043675 PMC 788831133593785 · doi ↗ · pubmed ↗
- 3Mathews L . Pain in children: neglected, unaddressed and mismanaged. Indian J Palliat Care. 2011;17(Suppl):S 70–S 73. 10.4103/0973-1075.76247 21811376 PMC 3140088 · doi ↗ · pubmed ↗
- 4Odell S , Logan DE . Pediatric pain management: the multidisciplinary approach. J Pain Res. 2013;6:785–790. 10.2147/jpr.S 37434 24250232 PMC 3829620 · doi ↗ · pubmed ↗
- 5Sola RG , Pulido P . Neurosurgical treatment of pain. Brain Sci. 2022;12(11):1584. 10.3390/brainsci 12111584 36421909 PMC 9688870 · doi ↗ · pubmed ↗
- 6Anekar A , Hendrix J , Cascella M . WHO Analgesic Ladder. Tampa/St. Petersburg, FL: Stat Pearls Publishing; 2024. https://www.ncbi.nlm.nih.gov/books/NBK 554435/
- 7Shah RD , Cappiello D , Suresh S . Interventional procedures for chronic pain in children and adolescents: a review of the current evidence. Pain Pract. 2016;16(3):359–369. 10.1111/papr.12285 25753547 · doi ↗ · pubmed ↗
- 8Walker SM . Pain in children: recent advances and ongoing challenges. Br J Anaesth. 2008;101(1):101–110. 10.1093/bja/aen 097 18430745 · doi ↗ · pubmed ↗