Fluoroscopic guidance for bulla identification during ventral bulla osteotomy in eight French bulldogs
Hui Yu Lu, Jeffery J. Biskup, Lea R. Mehrkens, Debbie Reynolds

TL;DR
This study shows how fluoroscopy can help identify the bulla during surgery in French bulldogs with middle ear infections.
Contribution
The novel use of fluoroscopic guidance for bulla identification in ventral bulla osteotomy in brachycephalic breeds is described.
Findings
Fluoroscopy successfully guided bulla identification in eight French bulldogs.
Six dogs retained a head tilt post-surgery, but most showed improvement over time.
One dog required additional surgery due to recurring otitis media.
Abstract
To describe the technique and outcome of fluoroscopy to guide bulla identification in French bulldogs during ventral bulla osteotomy. Medical records of eight French bulldogs with otitis media that underwent a fluoroscopic‐guided ventral bulla osteotomy between January 2020 and June 2023 were reviewed. Demographics, preoperative diagnostic findings, advanced imaging findings, surgical times, histopathology and culture results, as well as postoperative outcomes, were recorded. Following routine dissection of the bulla, fluoroscopic imaging was used to confirm the placement of a Steinmann pin before bulla penetration. The median surgical time was 152 minutes (range: 80–210 minutes). All dogs survived to discharge. Six out of eight dogs retained an ipsilateral head tilt postoperatively. Two dogs exhibited residual vestibular ataxia at 14 days postoperatively, which improved and resolved…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
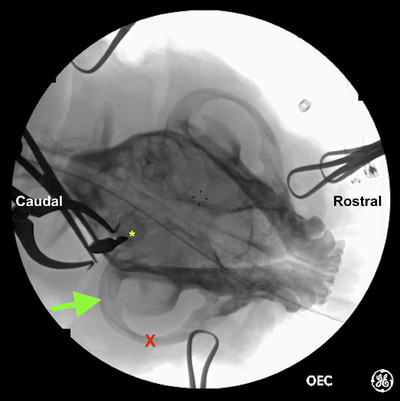 FIGURE 1
FIGURE 1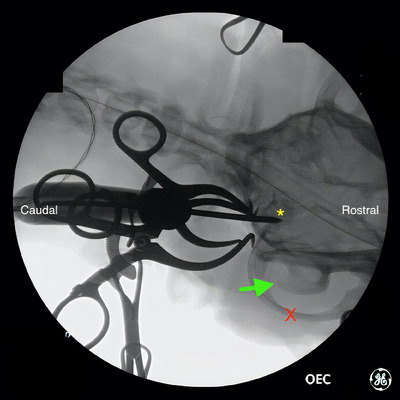 FIGURE 2
FIGURE 2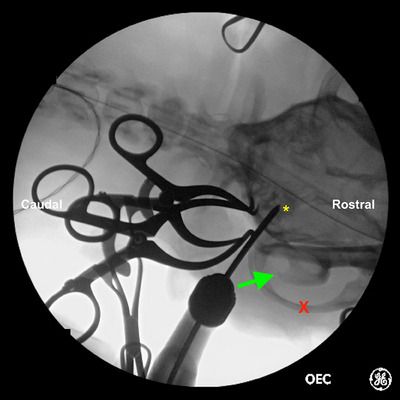 FIGURE 3
FIGURE 3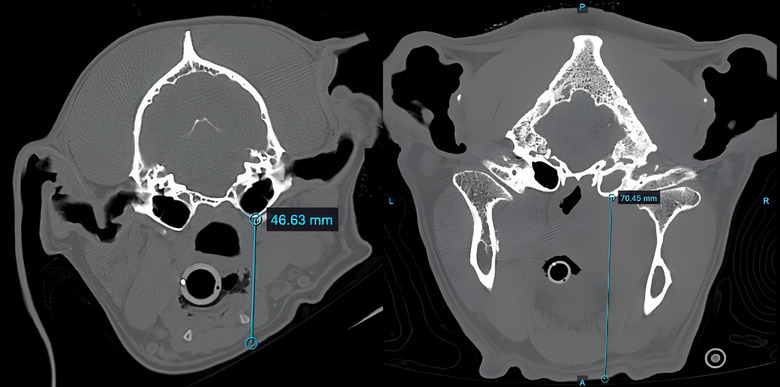 FIGURE 4
FIGURE 4| Dog | Sex | Age (years) | Weight (kg) | Clinically affected side | Duration of clinical signs (days) | Preoperative bloodwork abnormalities | Abnormal side(s) on preoperative MRI imaging | CNS extension | CSF findings | Duration of anaesthesia (min) | Duration of surgery (min) | Duration of hospitalisation (days) | Vertical distance from skin to ventral bulla (mm) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | FS | 3 | 11.8 | Left | 10 | NA | Bilateral | Yes |
Protein 162.7 mg/dL WBC 5304/µL | 165 | 90 | 4 | 56.9 |
| 2 | MN | 0.75 | 9.6 | Right | 35 | ALT 147 U/L | Bilateral | No | NA | 240 | 105 | 2 | NA |
| 3 | MN | 5 | 15.8 | Left | 60 | Neutrophilia 13 × 109/L | Left | No | NA | 240 | 195 | 1 | NA |
| 4 | MN | 3 | 14.4 | Right | 5 | Hyperbilirubinemia 17 µmol/L | Right | Yes |
Protein 647.2 mg/dL WBC 1664/µL | 195 | 180 | 2 | 56.8 |
| 5 | FS | 3 | 10.5 | Left | 5 | NA | Left | Yes |
Protein 200 mg/dL WBC 217.6/µL | 305 | 210 | 1 | 56.3 |
| 6 | ME | 2.5 | 15.6 | Left | 2 | Leukocytosis 18 × 109/L | Left | Yes |
Protein 23 mg/dL WBC 92.8 /µL | 180 | 135 | 2 | 41.3 |
| 7 | MN | 4 | 11 | Right | 4 | Neutrophilia 12.6 × 109/L, ALT 287 U/L | Bilateral | No | NA | 260 | 170 | 2 | 45.0 |
| 8 | MN | 11 | 15.4 | Right | 334 | Hyperglobulinemia 47 g/L | Right | Yes |
Protein 20 mg/dL WBC 0/µL | 170 | 80 | 2 | 70.4 |
| Postoperative complications | ||||||
|---|---|---|---|---|---|---|
| Dog | Intraoperative complications | <14 days | >14‐day follow‐up duration (days) | Description | Histopathological diagnosis | Culture and sensitivity results |
| 1 | None | Static left head tilt and facial nerve paralysis | 120 | Static left head tilt and facial nerve paralysis, chronically on steroids due to recurring otitis media, total ear canal ablation surgery was recommended. | Lymphoplasmacytic and neutrophilic otitis media with fibroplasia | No growth |
| 2 | None | Static right head tilt | 440 | Static right head tilt | Granuloma tissue | No growth |
| 3 | None | Decreased left palpebral response | 726 | Static decreased left palpebral response | Chronic‐active otitis media with inflammatory polyp | No growth |
| 4 | None | Mild vestibular ataxia | 210 | Mild but improved vestibular ataxia | Tympanokeratoma/cholesteatoma | Methicillin‐resistant |
| 5 | None | Static left head tilt and mild positional nystagmus | 180 | Static left head tilt | Chronic suppurative lymphoplasmacytic otitis media with inflammatory polyp |
|
| 6 | None | Static left head tilt and mild vestibular ataxia | 730 | Static left head tilt, resolved vestibular ataxia | Suppurative haemorrhagic otitis media with granulation tissue |
|
| 7 | Mild drug‐associated dysphoria, self‐resolved | Static right head tilt | 1491 | Static right head tilt | Not applicable | Beta‐haemolytic |
| 8 | None | Static right head tilt | 208 | Static right head tilt | Suppurative lymphoplasmacytic otitis media | No growth |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEar Surgery and Otitis Media · Veterinary Oncology Research · Nasal Surgery and Airway Studies
INTRODUCTION
Brachycephalic dog breeds’ unique skull conformation predisposes to several disease processes, with several studies reporting associations between brachycephaly and middle ear disease because skull conformation obstructs the Eustachian tube.1, 2, 3, 4 In 55 brachycephalic dogs that had computed tomography (CT) for respiratory signs, middle ear effusion was discovered incidentally in 53% of French bulldogs.5 Similarly, in a study of routine skull CT imaging of 75 French bulldogs and pugs undergoing brachycephalic airway corrective surgery, 40% of dogs exhibited middle ear effusion and 82% had narrowed ear canals.6 It has been hypothesised that compromise to the patency of the Eustachian tubes results in a buildup of ceruminous debris and fluid in the middle ear, creating an ideal microenvironment for the proliferation of bacteria and subsequently leading to otitis media.7
In cases where medical management for otitis media does not improve clinical signs or there is a central extension of disease, ventral bulla osteotomy (VBO) is a viable surgical treatment option to remove debris and diseased tissue of the middle ear and to debride the bulla lining while leaving the external canal intact in patients that do not have a history of otitis externa.8, 9, 10 Ventral bulla osteotomy is an alternative treatment option to a total ear canal ablation and lateral bulla osteotomy (TECA‐LBO) as it has the potential to preserve any residual hearing ability.11 Identification of the bulla is challenging in brachycephalic dogs due to their unique skull conformation, small bulla size, and thick muscle overlying the bulla.12 Intraoperative image guidance has been reported to allow for better identification of the bulla in dogs receiving a VBO for cholesteatoma. This technique has only been reported in dolichocephalic dogs.8 Fluoroscopy is an intraoperative imaging modality typically available in referral veterinary hospitals due to its frequent use in fracture repairs.13 To the best of the authors' knowledge, there are no studies describing the use of intraoperative fluoroscopy to identify the bulla.
The objective of this study was to describe the technique and outcomes of intraoperative fluoroscopy in bulla identification for VBOs in French bulldogs with otitis media.
MATERIALS AND METHODS
Medical records for French bulldogs that underwent a fluoroscopic guided VBO at Toronto Animal Health Partners Emergency and Specialty Hospital between 1 January 2020 and 1 June 2023 were reviewed and enrolled. Data collected included signalment, weight, laterality (left, right or bilateral), surgical indication (primary otitis media or secondary otitis media due to cholesteatoma or other tumours), physical examination findings, preoperative bloodwork, preoperative imaging (magnetic resonance imaging [MRI] and/or CT) findings, cerebrospinal fluid (CSF) findings, duration of surgery, postoperative CT findings, intra‐ and postoperative complications and histopathology results. The vertical distance from the ventral bulla to the skin was measured in the preoperative CT images using the Keystone Omni software (Asteris).
All dogs received a 14‐day postoperative recheck involving history collection and a physical examination. Subsequent follow‐up, more than 14 days postoperatively, was performed either by a telephone call or an in‐person recheck comprising history collection and a physical examination.
Surgical technique—Fluoroscopic guided VBO
The dogs were placed under general anaesthesia and were positioned in ventral recumbency for CT and MRI scans. All dogs were positioned in dorsal recumbency for surgery, with the ventral neck clipped and aseptically prepared. A rolled towel was placed under the dorsal cervical region to elevate the caudal skull.
Fluoroscopic imaging was performed to allow identification of the bulla before skin incision. On the ventrodorsal view of the skull, the ventral bulla was identified as a circular radio‐opaque structure caudomedial to the zygomatic arch and vertical ramus of the mandible, as labelled in Figures 1, 2, 3.
Ventrodorsal fluoroscopic image of French bulldog #8 undergoing fluoroscopic guided ventral bulla osteotomy. Following soft tissue dissection and using fluoroscopic guidance, a Freer periosteal elevator was positioned over the ventral bulla (yellow asterisk) once identified. The zygomatic arch (red X) and vertical ramus of the mandible (green arrow) are as labelled.
Ventrodorsal fluoroscopic image of French bulldog #8 undergoing fluoroscopic guided ventral bulla osteotomy. Following soft tissue dissection and using fluoroscopic guidance, a 3/32” Steinmann pin was advanced in the ventral bulla (yellow asterisk). The zygomatic arch (red X) and vertical ramus of the mandible (green arrow) are as labelled.
A second intraoperative ventrodorsal fluoroscopic image of French bulldog #8 undergoing fluoroscopic guided ventral bulla osteotomy. The ventral bulla (yellow asterisk), zygomatic arch (red X) and vertical ramus of the mandible (green arrow) are as labelled.
A paramedian skin incision approximately 3 cm long was made over the region of the bulla. The subcutaneous tissues and the platysma muscles were bluntly dissected. The bifurcation of the linguofacial and maxillary veins was retracted laterally. The muscles (digastricus, mylohyoid, hyoglossus and styloglossus) ventral to the area of the bulla, medial to the vertical ramus of the mandible and ventral to the trachea were bluntly separated to allow exposure of the ventral aspect of the skull. Drop‐handled Gelpi retractors were used to maintain exposure. Once the bulla was identified, a 3/32‘‘ Steinmann pin was aimed ventrodorsally in the region of the bulla, and the pin was subsequently advanced into the bulla once the location was confirmed by fluoroscopy. The defect was enlarged with Kerrison rongeurs. The interior of the bulla was examined, and the bulla lining was removed using curettage with samples obtained for culture and sensitivity (n = 8/8) and histopathological examination (n = 7/8). The bulla was flushed with sterile saline and visually inspected to ensure that the bulla epithelium had been removed.
The deeper subcutaneous tissue was closed with a simple continuous pattern with polydioxanone 2‐0 suture (PDS II, Ethicon, Johnson and Johnson). The subcutaneous tissue and skin were closed using a simple continuous pattern and intradermal pattern, respectively, with poliglecaprone 25 3‐0 suture (Monocryl, Ethicon).
RESULTS
Signalment and presenting clinical signs
Eight French bulldogs met the inclusion criteria (Table 1). The median age was 3 years (range: 9 months to 11 years) and the median weight was 13.1 kg (range: 9.6–15.6 kg). Neutered male dogs (n = 5/8) were the most common, followed by spayed females (n = 2/8) and entire males (n = 1/8).
All dogs presented with signs of a head tilt ipsilateral to the clinically affected ear, with four of eight dogs exhibiting a left‐sided head tilt and four exhibiting a right‐sided head tilt. On otoscopic examination, severe stenosis of the external ear canals was not appreciated in any of the eight dogs. Other reported clinical signs included vestibular ataxia (n = 6/8), nystagmus (n = 4/8), unilateral facial nerve paralysis (n = 2/8), inappetence (n = 3/8), unilateral aural discharge (n = 1/8), lethargy (n = 1/8), pain on opening mouth (n = 1/8) and restlessness (n = 1/8).
Duration of clinical signs and preoperative medical treatment
The median duration of clinical signs before evaluation was 7.5 days (range: 2–334 days) (Table 1). Six dogs were receiving systemic oral antibiotics before surgery. Three dogs (n = 3/6) received amoxicillin–clavulanate acid, and the remaining dogs received clindamycin, metronidazole and enrofloxacin, respectively.
Preoperative diagnostic testing
All dogs had preoperative serum biochemistry and complete blood count, with three dogs exhibiting an inflammatory leukocytosis characterised by mild neutrophilia (12.6 × 10^9^/L and 13.0 × 10^9^/L, respectively, range: 2.9–11.6 × 10^9^/L). Two dogs displayed a mildly elevated alanine aminotransferase (147 and 246 U/L, respectively; range: 10–125 U/L), one dog exhibited hyperglobulinemia (47 g/L; range: 25–45 g/L) and one dog exhibited a mild elevation in total bilirubin (17 µmol/L; range: 0–15 µmol/L) (Table 1).
All dogs underwent a head MRI scan preoperatively (Table 1). Homogenous and isointense T2 hyperintensity was observed in both bullae in three of eight dogs and the clinically affected bulla in the remaining five of eight dogs. Contrast enhancement of the muscles surrounding the affected bulla was observed in all dogs. Five dogs exhibited concurrent signs of extension into the cerebrum on the clinically affected side. There was a mildly compressive cervical intervertebral disc extrusion in one dog. Six of eight dogs underwent a preoperative CT to assist in surgical planning. Based on the preoperative CT images, the median vertical distance from the skin of the ventral mandible to the ventral bulla was 56.6 mm (range: 41.3–70.4 mm) (Figure 4).
Axial preoperative computed tomography image of a brachycephalic dog (French bulldog #8) skull with the distance from the ventral bulla to skin measured at 70.4 mm, respectively, using the Keystone Omni software (asterisk).
A CSF tap from the cerebellomedullary cistern was performed in the five dogs that were suspected of exhibiting signs of cerebrum extension based on MRI imaging. The median protein level of the CSF fluid was 191 mg/dL (range: 20–647 mg/dL; reference range: <30 mg/dL) and the median leukocyte count was 217/µL (range: 0–5304/µL, reference range: 0–4/µL). No atypical neoplastic cells or infectious organisms were identified in any of the five samples. The aerobic and anaerobic cultures of the CSF fluid were negative for growth in all dogs.
Intraoperative complications
Three surgeons performed the surgery on eight dogs with identification of the bulla successfully achieved, with two to three adjustments in pin placement before entry into the bulla. No significant intraoperative haemorrhage was encountered. Intraoperative damage to the nerves around the bulla was not identified postoperatively. All eight dogs recovered uneventfully from anaesthesia aside from one dog exhibiting drug‐associated dysphoria, which self‐resolved.
Duration of surgery and hospitalisation
The median duration of surgery was 152 minutes (range: 80–210 minutes). The median duration of hospitalisation was 2 days (range: 1–4 days) (Table 1).
Postoperative CT imaging findings
Three dogs received a postoperative CT immediately following surgery, which revealed subcutaneous emphysema of the ventral neck from surgery as well as a defect created in the ventral bulla, confirming appropriate anatomical identification.
Histopathology of the bulla
Histopathology of the affected bulla was obtained in seven of eight dogs. In the remaining dog where histopathology was not performed, a postoperative CT was performed, which confirmed that there was an osteotomy of the bulla. All samples were interpreted as suppurative lymphoplasmacytic inflammation suggestive of otitis media. Two of the seven samples had concurrent inflammatory polyps, one sample with granulation tissue and one sample with tympanokeratoma/cholesteatoma (Table 2).
Culture and sensitivity testing of the bulla samples
Intraoperative aerobic cultures were performed in all eight dogs, in which four of eight were positive for growth and remaining four negative for growth (Table 2).
Postoperative follow‐up
The median follow‐up duration was 325 days postoperatively (range: 120–1491 days). At the 14‐day postoperative recheck, six of eight dogs displayed a persistent head tilt, which was static to their preoperative status. None of these dogs showed improvement at their secondary follow‐up. One dog exhibited a decreased palpebral response at the 14‐day postoperative recheck, which was static at 729 days postoperatively.
Two out of five dogs that displayed evidence of secondary meningitis on MRI and CSF diagnostic testing exhibited residual ataxia at the 14‐day recheck. One of these dogs was reported to show signs of improvement at the 210‐day postoperative recheck and the other was found to have resolved signs 2 years postoperatively (Table 2).
One dog developed recurring otitis media in the affected ear 4 months postoperatively. The dog was chronically managed with prednisone and antibiotics by its primary referring veterinarian, with no significant improvement in clinical signs. A TECA‐LBO was recommended as a salvage procedure to eliminate the source of recurring infection but was declined by the owner.
DISCUSSION
This case series described the technique and outcomes of using intraoperative fluoroscopy to aid the surgical approach to the French bulldog bulla. The current described surgical approach for VBOs in dogs and cats relies heavily on palpation of the bulla and bony landmarks such as the ramus of the mandible.14 In a comparative study,15 French bulldogs and pugs exhibited more anatomical overlap of their temporomandibular joints and tympanic bullae than mesaticephalic dogs, with the bulla located directly medial to the temporomandibular joint. Anecdotally, distinguishing between the ventral surface of the tympanic bulla and the ventral aspect of the ramus of the mandible is extremely challenging on digital palpation in brachycephalic dogs due to this overlapping of surgical landmarks. In this case series, it was found that the distance between the skin and the bulla was a median of 56.6 mm, preventing palpation of the bulla easily. Due to the inability to palpate the normal anatomic landmarks, fluoroscopy allowed increased confidence in the dissection and identification of the bulla.
Other reported techniques for identification of the bulla for VBO, such as optic image‐guided and transoral VBOs, have their own limitations.8, 16 Optic image‐guided systems are not readily accessible in veterinary medicine and were only evaluated in dolichocephalic breeds in which identification of the bulla may be more feasible. The study describing a minimally invasive transoral approach for VBOs was performed in 12 cadavers, where only three of 12 dogs were brachycephalic and none were French bulldogs.16 The clinical application of the transoral technique has not been reported, and the effectiveness of this approach has not been assessed in live dogs. Given that fluoroscopy is commonly available in referral veterinary hospital settings, the authors believe that fluoroscopic guided VBO can be of added value due to its accessibility and simplicity of the approach.
To the best of the authors' knowledge, there are no previous reports of surgical times for VBOs in brachycephalic dogs. The surgical times reported for the limited number of cases here were comparable to what has been previously reported for TECA‐LBOs in brachycephalic dogs.17 Fluoroscopic guidance was introduced in the hope of accelerating bulla identification. With increased comfort with the technique, it is suspected that surgical times will improve, which in turn will increase patient safety.
Despite brachycephalic dogs being reported to have narrower ear canals compared to dolichocephalic dogs, VBO should still be considered as an alternative treatment option for otitis media, because the procedure is less invasive than TECA‐LBO and residual hearing can potentially be preserved.5, 11, 18 In addition, improvement in preoperative clinical signs was documented in seven of eight dogs in our study without resorting to TECA‐LBO, which is considered a salvage procedure.19 Even though VBO did not consistently resolve preoperative clinical signs such as head tilt, vestibular ataxia and facial nerve paralysis, these clinical signs were reported to be mild, and long‐term improvement of ataxia and facial nerve paralysis was observed.
Limitations of this study included the small sample size in this descriptive study. With no control group and standardised outcome measures, no statements can be made regarding the technique's superiority to any other described technique for bulla identification.
In conclusion, intraoperative use of fluoroscopy could be considered to guide the identification of the bulla in VBOs in brachycephalic breeds, where the surgical approach can be challenging due to their skull conformation.
AUTHOR CONTRIBUTIONS
Hui Yu Lu: Data curation (lead); writing—original draft (lead); writing—review and editing (lead). Jeffery J. Biskup and Lea R. Mehrkens: Conceptualisation (supporting); methodology (equal); writing—review and editing (supporting). Debbie Reynolds: Conceptualisation (lead); methodology (lead); writing—review and editing (lead).
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
FUNDING INFORMATION
The authors received no specific funding for this work.
ETHICS STATEMENT
The authors confirm that the ethical policies of the journal, as noted on the journal's author guidelines page, have been adhered to. No formal ethical approval was required because this was a series of clinical cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Reeve EJ , Sutton D , Friend EJ , Warren‐Smith CMR . Documenting the prevalence of hiatal hernia and oesophageal abnormalities in brachycephalic dogs using fluoroscopy. J Small Anim Pract. 2017;58:703–708. 10.1111/jsap.12734 28963795 · doi ↗ · pubmed ↗
- 2Milne E , Nuttall T , Marioni‐Henry K , Piccinelli C , Schwarz T , Azar A et al. Cytological and microbiological characteristics of middle ear effusions in brachycephalic dogs. J Vet Intern Med. 2020;34:1454–1463. 10.1111/jvim.15792 32407559 PMC 7379010 · doi ↗ · pubmed ↗
- 3Freiche V , German AJ . Digestive diseases in brachycephalic dogs. Vet Clin North Am Small Anim Pract. 2021;51:61–78. 10.1016/j.cvsm.2020.09.006 33187623 · doi ↗ · pubmed ↗
- 4Krainer D , Dupré G . Brachycephalic obstructive airway syndrome. Vet Clin North Am Small Anim Pract. 2022;52:749–780. 10.1016/j.cvsm.2022.01.013 35379494 · doi ↗ · pubmed ↗
- 5Schuenemann R , Kamradt A , Truar K , Oechtering G . Prevalence and characterization of middle ear effusion in 55 brachycephalic dogs. Tierarztl Prax Ausg K Kleintiere Heimtiere. 2022;50:329–336. 10.1055/a-1913-7216 36100247 · doi ↗ · pubmed ↗
- 6Töpfer T , Köhler C , Rösch S , Oechtering G . Brachycephaly in French bulldogs and pugs is associated with narrow ear canals. Vet Dermatol. 2022;33:214. 10.1111/vde.13067 35293639 · doi ↗ · pubmed ↗
- 7Gotthelf LN . Diagnosis and treatment of otitis media in dogs and cats. Vet Clin North Am Small Anim Pract. 2004;34:469–487. 10.1016/j.cvsm.2003.10.007 15062620 · doi ↗ · pubmed ↗
- 8Bellah JR . Ear. In: Bojrab MJ , Monnet E , editors. Mechanisms of disease in small animal surgery. 3rd ed. Jackson, WY, USA: Teton New Media; 2010. p. 1049–1050.