Endobiliary metastasis of colorectal cancer: A rare presentation and diagnostic dilemma: A case report
Guelbi Mohamed, Hajri Mohamed, Tangour Monia, Ghariani Rayfa, Bayar Rached, Bacha Dhouha

TL;DR
This case report highlights the rare occurrence of colorectal cancer spreading to the bile duct, which can be hard to diagnose as it looks like a primary bile tumor.
Contribution
The paper presents a rare case of endobiliary metastasis from colorectal cancer and emphasizes the importance of immunohistochemistry for accurate diagnosis.
Findings
Endobiliary metastasis mimics primary biliary tumors, causing diagnostic challenges.
Immunohistochemical markers like CDX2 are crucial for confirming metastasis.
A multidisciplinary approach is needed for accurate diagnosis and management.
Abstract
Colorectal cancer is a common malignancy with liver metastases frequently encountered. However, endobiliary metastases are extremely rare and can pose significant diagnostic challenges as they can mimic primary biliary tumors. We report a 66-year-old female who underwent an extended right hemicolectomy for a well-differentiated adenocarcinoma of the transverse colon pT4aN1bM0. Two years after surgery, follow-up imaging revealed intrahepatic biliary dilation and subtle intraductal lesions, along with suspicious splenic nodules. Hepatic MRI confirmed the presence of endoluminal biliary nodules with upstream dilation. Percutaneous biopsy and immunohistochemical analysis showed tumor cells positive for CDX2 and negative for CD20, supported the diagnosis of intrabiliary colonic metastasis. The clinical and radiological features of endobiliary metastasis can mimic those of primary biliary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
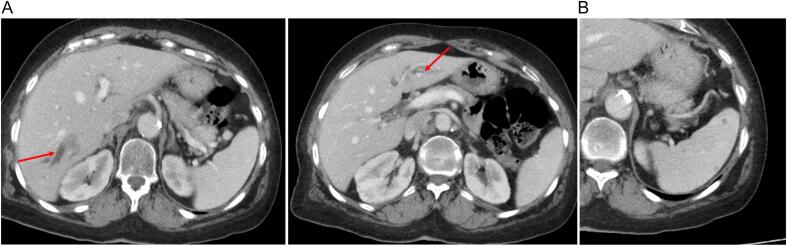 Figure 1
Figure 1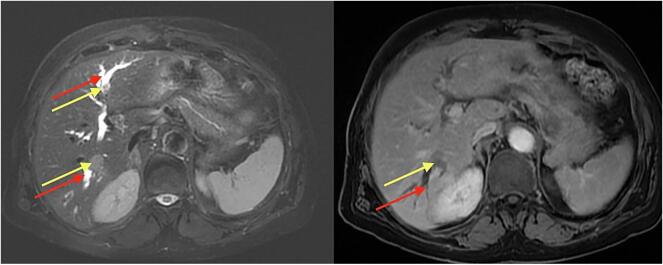 Figure 2
Figure 2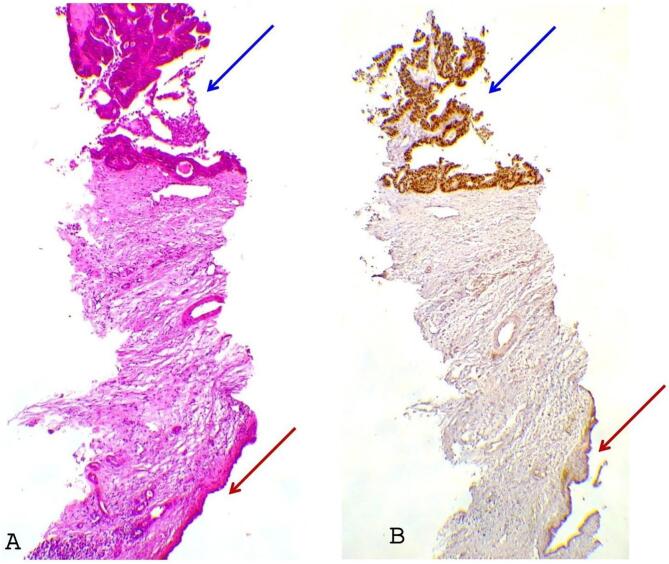 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Cholangiocarcinoma and Gallbladder Cancer Studies · Peptidase Inhibition and Analysis
Introduction
1
Colorectal cancer (CRC) is one of the most common malignancies ranking third worldwide [1], with liver being the primary metastatic site [2]. However, endobiliary metastasis of CRC is a rare and often underrecognized phenomenon with an incidence as low as 3,6 % [3] making its diagnosis and management a challenge. Through this case we aim to provide a clinical presentation, diagnostic strategies, and management options for endobiliary metastasis of colorectal cancer.
Presentation of case
2
We report the case of a 66-year-old female patient with no prior medical history, she was operated for a transverse colon tumor she had an extended right hemicolectomy. Histopathological examination of the specimen revealed a well differentiated adenocarcinoma of the colon classified pT4aN1b.No distant metastases were detected by the pre-operative CT scan of chest and abdomen. The patient received an adjuvant chemotherapy (XELOX 6 cycles) and was regularly monitored in our outpatient department.
During follow up, the patient was asymptomatic with a soft abdomen on clinical examination, laboratory test especially liver enzymes and tumor markers ACE and CA19-9 were in normal range. However, the CT scan after two years of the surgery revealed intrahepatic biliary duct dilation particularly in segments VI and II of the liver, with subtle low dense lesions in these bile ducts (Fig. 1A). The CT scan revealed also multiple millimetric nodules of the spleen (Fig. 1B). Hepatic MRI showed two endoluminal biliary nodules in segments VII and I, measuring 30 mm and 10 mm respectively with upstream biliary duct dilation (Fig. 2), suggestive of secondary lesions with multiple metastatic splenic nodules.Fig. 1A: Axial abdominal CT scan with portal time injection showing a dilation of biliary tracts of liver segments II and VI.B: Axial abdominal CT scan with portal time injection showing multiples low dense lesion of the spleen.Fig. 1. Fig. 2MRI of the liver with and without gadolinium injection showing a dilation of biliary tracts (red arrow) upstream two endoluminal biliary nodules in segments VII and II (yellow arrow). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Fig. 2
The patient underwent a percutaneous biopsy of the hepatic lesions, histopathological and immuhistochemical findings confirmed the presence of adenocarcinoma cells of primary colonic origin.
The standard hematoxylin eosin-stained slides showed tubulo-papillary carcinomatous expansion budding in intra-lumen bordered by a biliary epithelium (Fig. 3A), the neoplastic cells were all positive for CDX2 and negative for CD20 supporting the diagnosis of intrabiliary colonic metastasis (Fig. 3B). After multidisciplinary discussion it was decided to put the patient under chemotherapy (FOLFIRINOX).Fig. 3A: Microscopic examination.Tubulo-papillary carcinomatous expansion (blue arrow) budding in intra-lumen bordered by a biliary epithelium (red arrows) (hematoxylin-eosin: HE×100).B: Immunohistochemistry.Tubulo-papillary carcinomatous expansion (blue arrow) shows nuclear staining with CDX2 supporting the diagnosis of intestinal/colonic epithelium, while the biliary one (red arrows) is negative. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Fig. 3
Discussion
3
Endobiliary metastasis of colorectal cancer remains an exceedingly rare clinical entity, presenting significant diagnostic challenges. Its infrequent occurrence often means that clinicians may not initially consider it in the differential diagnosis of biliary obstruction and may be easily misdiagnosed with a primitive biliary or hepatic neoplasm on morphologic and clinical grounds. The history of colorectal cancer must be taken into consideration in patients presenting with dilated biliary ducts [4].
The pathophysiology behind endobiliary metastasis remains unclear, it has been hypothesized that tumor cells implantation in bile duct epithelium could be through a peribiliary capillary plexus communicating with portal veins and hepatic arteries [5].
As in our case, the clinical examination and routine laboratory tests are typically nonspecific. Patients may present with signs of biliary obstruction, such as jaundice or abdominal pain, and laboratory investigations might only reveal elevated liver enzymes with cholestasis, especially in cases involving proximal bile ducts, which represent 50 % of occurrences [6]. These findings are common to a broad spectrum of biliary disorders, thereby underscoring the need for a comprehensive diagnostic approach.
Radiological imaging is paramount in evaluating patients with suspected endobiliary metastasis. A multiphasic CT scan with liver protocol often reveals upstream biliary dilation or even subtle, hypodense intraductal lesions, these findings can mimic other biliary pathologies, such as primary cholangiocarcinoma [7]. Magnetic resonance imaging (MRI), with its superior soft-tissue contrast and the additional information provided by Diffusion-Weighted Imaging and Magnetic resonance cholangiopancreatography (MRCP), can help in the differential diagnosis of these challenging lesions [8]. Despite these advantages, imaging findings can often be ambiguous, as there is significant overlap in the radiological appearances of benign, primary malignant, and metastatic biliary lesions. This limitation further reinforces the need for additional diagnostic confirmation.
Therapeutic approaches to endobiliary metastasis of colorectal cancer are still evolving. The decision-making process should be tailored to each patient based on tumor burden, liver function, and overall performance status. Hepatectomy with a 1 mm margin is considered an adequate oncologic resection for colorectal liver metastasis [9] [10], while anatomical resection is necessary for a primary cholangiocarcinoma or a endobiliary metastasis of colorectal cancer [11]. However, for patients with non-resectable disease, systemic chemotherapy, remains the mainstay of treatment, aiming for tumor control and prolonged survival.
For cases where biliary obstruction leads to significant symptoms, palliative interventions such as endoscopic or percutaneous biliary drainage may be necessary to relieve obstruction and improve quality of life. The role of targeted therapies and immunotherapy in managing endobiliary metastases is an area of ongoing research, with emerging data suggesting that molecular profiling of tumors may guide personalized treatment strategies.
The unusual presentation in our case pushed us to complete the investigation by immunohistochemical analysis which plays a very important role in these cases. Tissue sampling obtained via percutaneous biopsy allows for the application of specific immunohistochemical markers that can conclusively differentiate colorectal metastases from primary biliary tumors. Markers such as CDX2 and CK20 are typically expressed in colorectal cancer cells and, when identified in biliary lesions, strongly indicate a colorectal origin [12]. The rarity of endobiliary metastasis from colorectal cancer, coupled with the nonspecific nature of clinical and laboratory findings, necessitates a high degree of clinical suspicion and a meticulous diagnostic approach. Patients' history should bring attention to this differential diagnosis, while radiological imaging plays a role in narrowing the diagnosis, it is ultimately the immunohistochemical analysis that provides the definitive diagnosis.
Conclusion
4
By improving awareness of this rare metastatic entity, clinicians can better differentiate it from other biliary pathologies and optimize patients' outcomes. Further research is essential to understand the pathophysiology behind it to optimize management strategies for this rare metastatic presentation.
Author contribution
Mohamed Guelbi: conceptualization, data curation, redaction, project manager.
Mohamed Hajri: conceptualization, redaction.
Monia Tangour: resources, visualization.
Rayfa Ghariani: resources, visualization.
Rached Bayar: supervision, validation, visualization.
Dhouha Bacha: supervision, validation, visualization.
Consent for publication
Written informed consent was obtained from legal authorized representatives before the study. On request, a copy of the written consent is available for review by the Editor-in-Chief of this journal.
Ethical approval
Ethical approval is exempt/waived at our institution.
Guarantor
Guelbi Mohamed.
Research registration number
Not applicable.
Funding
This work is not funded.
Conflict of interest statement
The authors declare no competing interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Biller L.H.Schrag D.Diagnosis and treatment of metastatic colorectal cancer: a review JAMA 325716 févr 20216693359135010.1001/jama.2021.0106 · doi ↗ · pubmed ↗
- 2Kow A.W.C.Hepatic metastasis from colorectal cancer J. Gastrointest. Oncol.106déc 2019127412983194994810.21037/jgo.2019.08.06PMC 6955002 · doi ↗ · pubmed ↗
- 3Estrella J.S.Othman M.L.Taggart M.W.Hamilton S.R.Curley S.A.Rashid A.Intrabiliary growth of liver metastases: clinicopathologic features, prevalence, and outcome Am. J. Surg. Pathol.3710 oct 2013157115792379772710.1097/PAS.0b 013e 318293 ddf 1PMC 3789528 · doi ↗ · pubmed ↗
- 4Takamatsu S.Teramoto K.Kawamura T.Kudo A.Noguchi N.Irie T.Liver metastasis from rectal cancer with prominent intrabile duct growth Pathol. Int.546juin 20044404451514440410.1111/j.1440-1827.2004.01636.x · doi ↗ · pubmed ↗
- 5Coppola S.Zucchini N.Romano F.Bovo G.Gilardoni E.Nespoli L.Colorectal liver metastasis with intrabiliary growth: case report and review of the literature Int. J. Surg. Pathol.223mai 20142722792377502010.1177/1066896913491317 · doi ↗ · pubmed ↗
- 6Traeger L.Kiroff G.Intrabilary obstruction by colorectal metastases J. Surg. Case Rep. [Internet]201811 janv 2018[cité 12 févr 2025]. Disponible sur:http://academic.oup.com/jscr/article/doi/10.1093/jscr/rjx 259/481259310.1093/jscr/rjx 259PMC 578624529383240 · doi ↗ · pubmed ↗
- 7Okano K.Yamamoto J.Okabayashi T.Sugawara Y.Shimada K.Kosuge T.CT imaging of intrabiliary growth of colorectal liver metastases: a comparison of pathological findings of resected specimens Br. J. Radiol.75894 juin 20024975011212423510.1259/bjr.75.894.750497 · doi ↗ · pubmed ↗
- 8Sugita R.Magnetic resonance evaluations of biliary malignancy and condition at high-risk for biliary malignancy: current status World J. Hepatol.51220136542443218310.4254/wjh.v 5.i 12.654PMC 3888665 · doi ↗ · pubmed ↗